

Abstract
Oral squamous cell carcinoma (OSCC) is the most common type of head and neck cancer. The 5-year survival rate has remained below 50% over the last two decades, and new tools for early diagnosis are needed. Saliva has been used for diagnosis of several systemic diseases, and its use for diagnosis of OSCC has been sought extensively. Among the many salivary analytes for diagnosis of OSCC, accumulating evidences indicate the possibility of using salivary cytokines. Overproduction of proinflammatory, proangiogenic cytokines by OSCC cells has been reported, and their role in tumor progression and angiogenesis is well established. However, many inflammatory conditions and immunological diseases could affect the levels of cytokines in serum and saliva. This article has reviewed publications in this matter, and some strengths and weaknesses have been pointed out. Conclusively, large-scale investigations are required for validation of the use of salivary cytokines for diagnosis of OSCC, with consideration to the influential role of periodontal inflammation in their levels.
Keywords: Cytokines, early diagnosis, interleukins, oral squamous cell carcinoma, saliva
INTRODUCTION
Oral cancer comprises 80–90% of head and neck cancer, with the most common tumor variant (80–90%) being oral squamous cell carcinoma (OSCC).[1,2] Worldwide, the 5-year survival rate of head and neck cancer has remained below 50% over the last two decades in spite of advances in treatment modalities.[2,3] The problems of distant metastasis, local recurrences, and difficulties in reconstruction, related to the late presentation of cases, comprise the main obstacles in treating OSCC. Therefore, early detection is a powerful approach in improving the treatment outcome and, accordingly, the survival rate.[4–7]
Conventionally, OSCC is diagnosed by histopathologic examination of biopsies from oral lesions that look suspicious upon direct visual examination. Although the histopathologic evaluation might differ from one interpreter to another, the method is very reliable if a representative sample is taken. In addition, the procedure is time and labor consuming for the health personnel and unpleasant for the patient, making it not suitable for community-based screening programs.[5] However, screening programs depending on visual examination solely are not always efficient since they depend on the anatomical site of the lesion (some more accessible than others), the examiner's expertise, and the pathological progression of the lesion.[8,9] Toluidine blue vital tissue staining has been suggested to enhance the outcome of visual examination or for selection of the best site of biopsy. Even though high sensitivity and specificity were reported by some authors, the experience of the observer seemed to have more influence than the dye itself.[5,10] Exfoliative cytology has been proposed as a possible substitute for the gold standard for diagnosis of OSCC. For reliable findings, full-thickness sampling is necessary as the cells lose their morphology upon maturation and keratinization. Although generally accepted by the patients, collection of full-thickness mucosal scraping induces pin point bleeding, and it is also prone to sampling errors. The average sensitivity of morphological analysis of scraped cells has been estimated as 87.4%, with lower detection rates in early stage disease. DNA image cytometry has improved the sensitivity of the method, but not to the extent that makes it a reliable diagnostic measure.[5,11,12] There is a need for more practical and simple methods for detection of OSCC to be used for definitive diagnosis, as well as for screening programs. In order to curb the growing incidence and mortality of this disease, such tests should also be convenient both for the patient and the health personnel.
OSCC is a multistep disease, and many genetic and epigenetic changes have been correlated to malignant transformation of potentially malignant oral lesions.[5] Several studies have examined possible genetic alterations related to OSCC that can be used as markers for early diagnosis.[13,14] Many of these alterations have been detected in exfoliated oral epithelial cells,[11] saliva,[15,16] or serum[17–19] of patients with OSCC. However, identification of a single marker or set of markers that could substitute conventional histopathology is yet to be confirmed.
SALIVA AS A DIAGNOSTIC BIOFLUID
The use of saliva as diagnostic biofluid has many advantages over other specimens like blood, exfoliated cells, and urine. It comprises a non-invasive, easy, and rapid to collect, and yet, a cost-effective specimen.[20] Analytes are present in low concentrations in saliva, and they are transferred from blood through the capillary walls, interstitial space, and the acini or duct cells into the lumen of the salivary gland duct.[21] Several protocols for collection of saliva have been proposed.[22] Although secretion of saliva could be stimulated by many ways, collection of unstimulated whole saliva between 9 and 11 a.m. has been considered the most informative way of performance. Whole saliva (oral biofluid) is a mixture of major and minor salivary gland secretions, gingival cervicular (sulcular) fluid, bronchial and nasal secretions, serum and blood derivatives from oral wounds, microorganisms, leukocytes, desquamated epithelial cells, and food debris.[21]
The use of saliva for diagnosis of disease has been sought centuries ago. However, the introduction of molecular laboratory techniques in 1980s has drawn more attention to saliva as a tool for detection of disease and for health monitoring in general.[23] Oral fluid analysis has been proved useful for detection of Sjögren's syndrome,[24,25] diabetes mellitus,[26] infection with Helicobacter pylori,[27] Cushing syndrome,[28] HIV,[29–31] and hepatitis C virus.[32,33] It is now being routinely used for the detection of abused as well as therapeutic drugs.[20] Saliva has also been suggested for breast cancer screening programs by detecting Her2\neu.[34–36] Withal, diseases of the oral cavity have been the most attractive ones for saliva diagnostics researchers, and the use of saliva for detection of dental caries[37] and periodontal diseases[38,39] has been suggested. Salivary diagnostics for OSCC, if becoming a routine, would also comprise a suitable tool for population screening, monitoring of patients at risk of recurrent tumor, and consequently for improving the survival rate of patients with this disease.[23,40]
SALIVA FOR OSCC DETECTION
Although many investigators have dealt with saliva of OSCC patients and have tried to find out the differences when compared to normal controls, the research in this field is still in its infancy and needs large-scale studies optimizing for many confounding factors introduced by the complexity of the oral environment.[16]
Both the genomic and proteomic approaches have been used to investigate salivary biomarkers for OSCC detection.[16] Antibodies against mutated P53,[41] mutations of TP53,[41] levels of hyaluronic acid,[42] SCC antigen,[43] Cyfra 21-1,[44] CD44,[45] and myosin and actin[46] have been suggested as possible markers for early diagnosis of OSCC. In addition, many other potential salivary markers have been reported.[15,16,40,47] However, the results of all these studies were lacking either proper samples size or the biological significance of the marker in carcinogenesis.
SALIVARY CYTOKINES AND OSCC
It has been proven that certain cytokines are produced by OSCC cells. Among these are interleukines (IL)-1, -6, -8, and tumor necrosis factor (TNF)-α.[48–50] Furthermore, expression profiling of OSCC using microarray indicated that IL-6 and -8 are significantly overexpressed by these tumors.[51] A role of cytokines in angiogenesis and tumor progression has been suggested.[52] Moreover, higher levels of some of the above-mentioned cytokines have been detected in the serum of OSCC patients when compared to the serum of healthy controls.[19,53] The serum levels of cytokines have been attributed to their production by the tumor cells as well as to the systemic response of the immune system to the tumor. Nonetheless, causes not related to the tumor could have contributed to that.
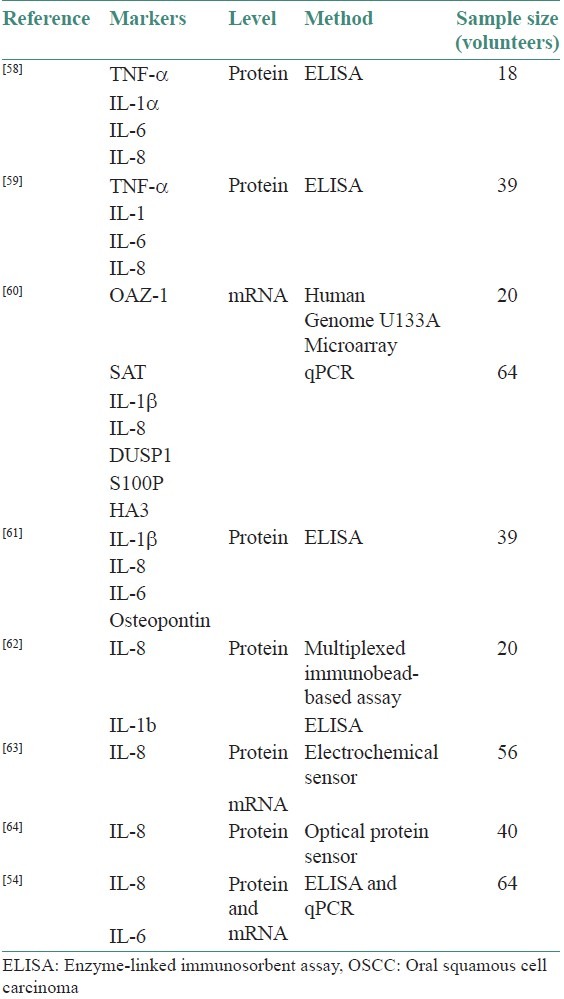
When the validity of IL-8 and -6 as biomarkers for OSCC diagnosis has been investigated, analysis of their levels in saliva of a group of 32 patients and 32 healthy controls, and in serum of 19 patients and 32 healthy controls, revealed high sensitivity and specificity of using salivary IL-8 and serum IL-6 levels simultaneously for predicting OSCC.[54] This investigation has been conducted by the “University of California, Los Angeles (UCLA) Collaborative Oral Fluid Diagnostic Research Centre,” a pioneer center that has been pursuing salivary diagnostics for OSCC for many years now.[40] Elevated levels of IL-6 and -8 have also been detected by others in saliva of patients with periodontitis and have been associated more with this inflammatory disease.[38,39,55,56] However, the above-mentioned study from UCLA[54] has indicated that significantly high salivary levels of only IL-8 and not IL-6 in OSCC patients suggested that the potential effect of periodontal inflammation on the levels of salivary IL-8 is disguised by the effect of OSCC. On the other hand, a drop to baseline in IL-6 levels has been reported by others in a group of OSCC patients after treatment, making it a possible marker for prognosis assessment.[57] Although an accumulating number of studies using different methods have indicated salivary IL-8 and -6 as diagnostic biomarkers for OSCC [Table 1], further validation on a larger scale of samples is still necessary.[54]
Table 1.
Studies suggesting salivary cytokine level for diagnosis of OSCC
Enzyme-linked immunosorbent assay (ELISA) has been used to investigate the differences in salivary levels of TNF-α, IL-1α, IL-6, and IL-8 between a group of nine patients with OSCC and matching healthy controls.[58] The strength of this study relies on the matched samples for gingival status using the modified gingival index. It reported that IL-6 difference between the two study groups was statistically significant and that the rest of the investigated cytokines were higher in the case group despite the statistical non-significance of these findings. However, this study has also a major limitation due to the fact that most of the patients were edentulous, in addition to the small sample size.[58] Another research group has studied the difference in the salivary level of TNF-α, IL-1α, IL-6, and IL-8, using ELISA, to differentiate between malignant (n = 13) and premalignant (n = 13) lesions, in comparison to healthy subjects (n = 13).[59] Their results revealed significant difference in levels of the four investigated cytokines between the three groups. They even suggested that it is possible to monitor the malignant transformation of premalignant oral lesions by using salivary levels of these cytokines.[65] ELISA has also been used to compare the levels of IL-1β, IL-6, IL-8, and osteopontin in cell-free saliva collected from 19 OSCC patients and 20 controls. The results showed significant difference of IL-6 between the two groups.[61] The use of cell-free saliva in this study has the advantage of excluding bacteria, leukocytes, and epithelial cells, which could bias the results. Furthermore, salivary IL-6 has also been suggested as a predictor of survival and prognosis of patients with OSCC.[18,66]
The UCLA Collaborative Oral Fluid Diagnostic Research Centre has sought to prove multiplexed immunobead-based assay as an efficient method in the analysis of cell-free saliva proteomics compared to conventional ELISA and immunoblotting.[62] This method has been able to detect higher levels of IL-8 and IL-1β in OSCC patients (n = 20) when compared to healthy controls (n = 20). In this investigation, IL-8 was also found to be higher in patients with periodontitis (n = 10) than in healthy controls, but much lower than the levels detected in patients with OSCC, which was in accordance with what have been reported before.[54] The authors have clearly acknowledged the limitation of the small sample size used in their investigation, and that further studies recruiting immunological disease control group are needed for confirmation of salivary IL-8 and IL-1b as diagnostic markers of OSCC.[62]
CYTOKINE mRNA IN CELL-FREE SALIVA
Transcriptome analysis on cell-free phase of saliva has been sought by UCLA Collaborative Oral Fluid Diagnostic Research Centre. First, they characterized the presence of mRNA in cell-free saliva and they identified a set of 185 mRNAs that are always detectable in saliva supernatant obtained from healthy subjects. They referred to them as Normal Salivary Core Transcripts (NSCT). A database of these transcripts has been established,[67] and the human origin of these transcripts has been determined by cDNA library analysis.[68] This research group has later investigated the best method of preserving salivary RNA in the ambient temperature, which has always been one of the main challenges for RNA-based studies.[69,70] In 2004, the group had published that analysis of saliva supernatant for mRNA of IL-8, IL-1β,dual specificity protein phosphatase 1 (DUSP1), H3 histone, family 3A (H3F3A or HA3), S100 calcium binding protein P (S100P), Ornithine Decarboxylase Antizyme-1 (OAZ-1), and spermidine/spermine N1-acetyltransferase 1 (SAT) as combination, had a sensitivity and specificity of 91%, respectively, in diagnosing OSCC.[60,71] This study also indicated remarkable increase of IL-8 mRNA in saliva of OSCC, and that salivary IL-8 mRNA alone can detect OSCC with a sensitivity and specificity of 81%, respectively. Nevertheless, that study has certain limitations regarding the number of patients recruited and the use of exploratory group in part of the experiment. Although the study has recruited participants of early stage disease with comparable smoking history, who have no history of autoimmune diseases, hepatitis, or HIV infection, it did not consider the periodontal status among other confounding factors that might alter the concentration of IL-8 mRNA in the oral cavity, depending on the previous conclusion about the effect of OSCC and periodontitis on IL-8 level.[54,62] The study addressed also the pertinent question of the origin of salivary RNA. The source of RNA in saliva could be the gingival cervicular fluid, the major salivary glands, or the desquamated epithelial cells from the oral mucosa. This study has also indicated that the mRNA's origin could be either the tumor itself or the systemic response to it.[60,71] However, expression profiling of serum of a comparable number of patients and controls has revealed that the best prediction mRNA combination was Homo sapiens thymosin beta 10 (THSMB) and ferritin heavy polypeptide 1 (FTH1), with a sensitivity and specificity of 91% and 71%, respectively.[72] Later on, in 2010, the same investigators[60] reported the validation of the same salivary biomarkers in a group of Serbian patients and controls (35 patients and 51 controls) to exclude populations differences.[73]
The use of saliva supernatant could be of better value in detecting biomarkers since it should exclude leukocytes and microbes.[40,71] Kumar et al. in 2006 had challenged the presence of mRNA in saliva, claiming that mRNA cannot be purified from saliva even when cellular pallet is included.[74] In that study, no reverse transcription polymerase chain reaction (RT-PCR) product for housekeeping genes like GAPDH could be obtained even from the cellular phase of saliva, and only weak signal was detected in the microarray, a signal that the authors have attributed to contamination with pseudogene of genomic origin. The results of that study were, however, questioned by other researchers,[75,76] mainly due to the method of RNA extraction,[67] the choice of RNALater® being evaluated by others as not appropriate for preservation of RNA in saliva,[69,70] and the lack of positive controls in the RNA extraction procedures. This makes questionable the conclusion of that study that extraction of RNA from the cellular phase of saliva is impossible and is prone to errors.[71] Salivary mRNA has been used in forensic determination of body fluids from crime scenes even weeks after the sample has been deposited.[77–80] It has also been suggested for determination of sleep driving as a potential cause of traffic accidents by detecting mucin expression level.[81] The relative stability of mRNA in saliva has been attributed to its association to other macromolecules in the oral biofluid.[82,83] Nevertheless, despite the reported high sensitivity and specificity and its relative stability in the oral environment, the study of Kumar et al. points to the delicate nature of mRNA and the difficulties in dealing with it that might hinder its use for screening of populations at high risk unless a rapid chairside test is developed.
In 2009, the UCLA group introduced an electrochemical sensor for multiplex biomarkers detection. Also, it has scored a sensitivity and specificity of 90%, respectively, in detecting OSCC, by using IL-8 mRNA and protein simultaneously.[63] This investigation has recruited 28 cases and matching controls that have not been matched according to the periodontal status. The study reported that the results of the electrochemical sensor were very close to the ones obtained by PCR and ELISA. High levels of IL-8 have also been detected in the saliva of OSCC using an optical protein sensor,[64] and the results were comparable to the ones obtained by ELISA, with higher ability of this sensor to detect lower concentration of the biomarkers than possible with conventional ELISA.
FUTURE DIRECTIONS AND CONCLUSION
There are still some miles to go for the salivary diagnostics of OSCC to be one of the routine practices in health provision. The current investigations indicate IL-8 and IL-6 as the most likely candidates for this purpose.[54,58–60,62,63,65] However, the expression of these cytokines can be biased by many other factors that should be considered in a large-scale population study before introducing them as reliable discriminatory OSCC markers.[55]
The comparison of the levels of these putative markers in OSCC patients with patients with potentially malignant oral lesions should also be considered as the next step to go in a large-scale population-based study within an international, multicenter collaborative investigation.
ACKNOWLEDGMENT
We would like to thank University of Bergen and Norwegian Educational Loan Fund for financial support.
Footnotes
Source of Support: Study was supported by University of Bergen and Norwegian Educational Loan Fund, through the Qouta program..
Conflict of Interest: None declared.
REFERENCES
- 1.Boyle P, Levin B. Lyon: International Agency for Research on Cancer; 2008. World Cancer Report 2008. [Google Scholar]
- 2.Funk GF, Karnell LH, Robinson RA, Zhen WK, Trask DK, Hoffman HT. Presentation, treatment, and outcome of oral cavity cancer: A National Cancer Data Base Report. Head Neck. 2002;24:165–80. doi: 10.1002/hed.10004. [DOI] [PubMed] [Google Scholar]
- 3.Vokes EE, Weichselbaum RR, Lippman SM, Hong WK. Head and neck cancer. N Engl J Med. 1993;328:184–94. doi: 10.1056/NEJM199301213280306. [DOI] [PubMed] [Google Scholar]
- 4.Allison P, Locker D, Feine JS. The role of diagnostic delays in the prognosis of oral cancer: A review of the literature. Oral Oncol. 1998;34:161–70. doi: 10.1016/s1368-8375(97)00071-7. [DOI] [PubMed] [Google Scholar]
- 5.Epstein JB, Zhang L, Rosin M. Advances in the diagnosis of oral premalignant and malignant lesions. J Can Dent Assoc. 2002;68:617–21. [PubMed] [Google Scholar]
- 6.Mashberg A, Samit A. Early diagnosis of asymptomatic oral and oropharyngeal squamous cancers. CA Cancer J Clin. 1995;45:328–51. doi: 10.3322/canjclin.45.6.328. [DOI] [PubMed] [Google Scholar]
- 7.Petersen PE. Oral cancer prevention and control-the approach of the World Health Organization. Oral Oncol. 2009;45:454–60. doi: 10.1016/j.oraloncology.2008.05.023. [DOI] [PubMed] [Google Scholar]
- 8.Hawkins RJ, Wang EE, Leake JL. Preventive health care, 1999 update: Prevention of oral cancer mortality.The Canadian task force on preventive health care. J Can Dent Assoc. 1999;65:617. [PubMed] [Google Scholar]
- 9.Kujan O, Glenny AM, Duxbury J, Thakker N, Sloan P. Evaluation of screening strategies for improving oral cancer mortality: A Cochrane systematic review. J Dent Educ. 2005;69:255–65. [PubMed] [Google Scholar]
- 10.Su WW, Yen AM, Chiu SY, Chen TH. A community-based RCT for oral cancer screening with toluidine blue. J Dent Res. 2010;89:933–7. doi: 10.1177/0022034510373763. [DOI] [PubMed] [Google Scholar]
- 11.Mehrotra R, Gupta A, Singh M, Ibrahim R. Application of cytology and molecular biology in diagnosing premalignant or malignant oral lesions. Mol Cancer. 2006;5:11. doi: 10.1186/1476-4598-5-11. [DOI] [PMC free article] [PubMed] [Google Scholar] [Retracted]
- 12.Acha A, Ruesga MT, Rodriguez MJ, Martinez de Pancorbo MA, Aguirre JM. Applications of the oral scraped (exfoliative) cytology in oral cancer and precancer. Med Oral Patol Oral Cir Bucal. 2005;10:95–102. [PubMed] [Google Scholar]
- 13.Lippman SM, Hong WK. Molecular markers of the risk of oral cancer. N Engl J Med. 2001;344:1323–6. doi: 10.1056/NEJM200104263441710. [DOI] [PubMed] [Google Scholar]
- 14.Spafford MF, Koch WM, Reed AL, Califano JA, Xu LH, Eisenberger CF, et al. Detection of head and neck squamous cell carcinoma among exfoliated oral mucosal cells by microsatellite analysis. Clin Cancer Res. 2001;7:607–12. [PubMed] [Google Scholar]
- 15.Nagler RM. Saliva as a tool for oral cancer diagnosis and prognosis. Oral Oncol. 2009;45:1006–10. doi: 10.1016/j.oraloncology.2009.07.005. [DOI] [PubMed] [Google Scholar]
- 16.Wu JY, Yi C, Chung HR, Wang DJ, Chang WC, Lee SY, et al. Potential biomarkers in saliva for oral squamous cell carcinoma. Oral Oncol. 2010;46:226–31. doi: 10.1016/j.oraloncology.2010.01.007. [DOI] [PubMed] [Google Scholar]
- 17.Feng XY, Li JH, Li JZ, Han ZX, Xing RD. Serum SCCA, Cyfra 21-1, EGFR and Cyclin D1 levels in patients with oral squamous cell carcinoma. Int J Biol Markers. 2010;25:93–8. doi: 10.1177/172460081002500206. [DOI] [PubMed] [Google Scholar]
- 18.Meyer F, Samson E, Douville P, Duchesne T, Liu G, Bairati I. Serum prognostic markers in head and neck cancer. Clin Cancer Res. 2010;16:1008–15. doi: 10.1158/1078-0432.CCR-09-2014. [DOI] [PubMed] [Google Scholar]
- 19.Jablonska E, Piotrowski L, Grabowska Z. Serum levels of IL-1β, IL-6, TNF-α, sTNF-RI and CRP in patients with oral cavity cancer. Pathol Oncol Res. 1997;3:126–9. doi: 10.1007/BF02907807. [DOI] [PubMed] [Google Scholar]
- 20.Choo RE, Huestis MA. Oral fluid as a diagnostic tool. Clin Chem Lab Med. 2004;42:1273–87. doi: 10.1515/CCLM.2004.248. [DOI] [PubMed] [Google Scholar]
- 21.Kaufman E, Lamster IB. The diagnostic applications of saliva-a review. Crit Rev Oral Biol Med. 2002;13:197–212. doi: 10.1177/154411130201300209. [DOI] [PubMed] [Google Scholar]
- 22.Navazesh M. Methods for collecting saliva. Ann N Y Acad Sci. 1993;694:72–7. doi: 10.1111/j.1749-6632.1993.tb18343.x. [DOI] [PubMed] [Google Scholar]
- 23.Zhang L, Xiao H, Wong DT. Salivary biomarkers for clinical applications. Mol Diagn Ther. 2009;13:245–59. doi: 10.1007/BF03256330. [DOI] [PubMed] [Google Scholar]
- 24.Berra A, Sterin-Borda L, Bacman S, Borda E. Role of salivary IgA in the pathogenesis of Sjogren syndrome. Clin Immunol. 2002;104:49–57. doi: 10.1006/clim.2002.5228. [DOI] [PubMed] [Google Scholar]
- 25.Hu S, Wang J, Meijer J, Ieong S, Xie Y, Yu T, et al. Salivary proteomic and genomic biomarkers for primary Sjogren's syndrome. Arthritis Rheum. 2007;56:3588–600. doi: 10.1002/art.22954. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Marchetti P, Benzi L, Masoni A, Cecchetti P, Giannarelli R, Di Cianni G, et al. Salivary insulin concentrations in type 2 (non-insulin-dependent) diabetic patients and obese non-diabetic subjects: Relationship to changes in plasma insulin levels after an oral glucose load. Diabetologia. 1986;29:695–8. doi: 10.1007/BF00870278. [DOI] [PubMed] [Google Scholar]
- 27.Reilly TG, Poxon V, Sanders DS, Elliott TS, Walt RP. Comparison of serum, salivary, and rapid whole blood diagnostic tests for Helicobacter pylori and their validation against endoscopy based tests. Gut. 1997;40:454–8. doi: 10.1136/gut.40.4.454. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Castro M, Elias PC, Martinelli CE, Jr, Antonini SR, Santiago L, Moreira AC. Salivary cortisol as a tool for physiological studies and diagnostic strategies. Braz J Med Biol Res. 2000;33:1171–5. doi: 10.1590/s0100-879x2000001000006. [DOI] [PubMed] [Google Scholar]
- 29.Scully C. HIV topic update: Salivary testing for antibodies. Oral Dis. 1997;3:212–5. doi: 10.1111/j.1601-0825.1997.tb00043.x. [DOI] [PubMed] [Google Scholar]
- 30.Emmons W. Accuracy of oral specimen testing for human immunodeficiency virus. Am J Med. 1997;102:15–20. doi: 10.1016/s0002-9343(97)00033-8. [DOI] [PubMed] [Google Scholar]
- 31.Malamud D. Oral diagnostic testing for detecting human immunodeficiency virus-1 antibodies: A technology whose time has come. Am J Med. 1997;102:9–14. doi: 10.1016/s0002-9343(97)00032-6. [DOI] [PubMed] [Google Scholar]
- 32.Bello PY, Pasquier C, Gourney P, Puel J, Izopet J. Assessment of a hepatitis C virus antibody assay in saliva for epidemiological studies. Eur J Clin Microbiol Infect Dis. 1998;17:570–2. doi: 10.1007/BF01708621. [DOI] [PubMed] [Google Scholar]
- 33.Elsana S, Sikuler E, Yaari A, Shemer-Avni Y, Abu-Shakra M, Buskila D, et al. HCV antibodies in saliva and urine. J Med Virol. 1998;55:24–7. [PubMed] [Google Scholar]
- 34.Streckfus C, Bigler L, Dellinger T, Pfeifer M, Rose A, Thigpen JT. CA 15-3 and c-erbB-2 presence in the saliva of women. Clin Oral Investig. 1999;3:138–43. doi: 10.1007/s007840050092. [DOI] [PubMed] [Google Scholar]
- 35.Streckfus C, Bigler L, Dellinger T, Dai X, Kingman A, Thigpen JT. The presence of soluble c-erbB-2 in saliva and serum among women with breast carcinoma: a preliminary study. Clin Cancer Res. 2000;6:2363–70. [PubMed] [Google Scholar]
- 36.Bigler LR, Streckfus CF, Copeland L, Burns R, Dai X, Kuhn M, et al. The potential use of saliva to detect recurrence of disease in women with breast carcinoma. J Oral Pathol Med. 2002;31:421–31. doi: 10.1034/j.1600-0714.2002.00123.x. [DOI] [PubMed] [Google Scholar]
- 37.Bai J, Zhou Q, Bao ZY, Li XX, Qin M. [Comparison of salivary proteins between children with early childhood caries and children without caries] Zhonghua Kou Qiang Yi Xue Za Zhi. 2007;42:21–3. [PubMed] [Google Scholar]
- 38.Giannobile WV, Beikler T, Kinney JS, Ramseier CA, Morelli T, Wong DT. Saliva as a diagnostic tool for periodontal disease: Current state and future directions. Periodontol 2000. 2009;50:52–64. doi: 10.1111/j.1600-0757.2008.00288.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Kinney JS, Ramseier CA, Giannobile WV. Oral fluid-based biomarkers of alveolar bone loss in periodontitis. Ann N Y Acad Sci. 2007;1098:230–51. doi: 10.1196/annals.1384.028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Lee JM, Garon E, Wong DT. Salivary diagnostics. Orthod Craniofac Res. 2009;12:206–11. doi: 10.1111/j.1601-6343.2009.01454.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Boyle JO, Mao L, Brennan JA, Koch WM, Eisele DW, Saunders JR, et al. Gene mutations in saliva as molecular markers for head and neck squamous cell carcinomas. Am J Surg. 1994;168:429–32. doi: 10.1016/s0002-9610(05)80092-3. [DOI] [PubMed] [Google Scholar]
- 42.Franzmann EJ, Schroeder GL, Goodwin WJ, Weed DT, Fisher P, Lokeshwar VB. Expression of tumor markers hyaluronic acid and hyaluronidase (HYAL1) in head and neck tumors. Int J Cancer. 2003;106:438–45. doi: 10.1002/ijc.11252. [DOI] [PubMed] [Google Scholar]
- 43.Yoshimura Y, Oka M, Harada T. Squamous cell carcinoma-antigen for detection of squamous cell and mucoepidermoid carcinoma after primary treatment: A preliminary report. J Oral Maxillofac Surg. 1990;48:1288–92. doi: 10.1016/0278-2391(90)90484-j. discussion 1292-3. [DOI] [PubMed] [Google Scholar]
- 44.Nagler R, Bahar G, Shpitzer T, Feinmesser R. Concomitant analysis of salivary tumor markers–a new diagnostic tool for oral cancer. Clin Cancer Res. 2006;12:3979–84. doi: 10.1158/1078-0432.CCR-05-2412. [DOI] [PubMed] [Google Scholar]
- 45.Franzmann EJ, Reategui EP, Pedroso F, Pernas FG, Karakullukcu BM, Carraway KL, et al. Soluble CD44 is a potential marker for the early detection of head and neck cancer. Cancer Epidemiol Biomarkers Prev. 2007;16:1348–55. doi: 10.1158/1055-9965.EPI-06-0011. [DOI] [PubMed] [Google Scholar]
- 46.de Jong EP, Xie H, Onsongo G, Stone MD, Chen XB, Kooren JA, et al. Quantitative proteomics reveals myosin and actin as promising saliva biomarkers for distinguishing pre-malignant and malignant oral lesions. PLoS One. 2010;5:e11148. doi: 10.1371/journal.pone.0011148. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Arellano M, Jiang J, Zhou X, Zhang L, Ye H, Wong DT, et al. Current advances in identification of cancer biomarkers in saliva. Front Biosci (Schol Ed) 2009;1:296–303. doi: 10.2741/S27. [DOI] [PubMed] [Google Scholar]
- 48.Chen Z, Malhotra PS, Thomas GR, Ondrey FG, Duffey DC, Smith CW, et al. Expression of proinflammatory and proangiogenic cytokines in patients with head and neck cancer. Clin Cancer Res. 1999;5:1369–79. [PubMed] [Google Scholar]
- 49.Cohen RF, Contrino J, Spiro JD, Mann EA, Chen LL, Kreutzer DL. Interleukin-8 expression by head and neck squamous cell carcinoma. Arch Otolaryngol Head Neck Surg. 1995;121:202–9. doi: 10.1001/archotol.1995.01890020064013. [DOI] [PubMed] [Google Scholar]
- 50.Mann EA, Spiro JD, Chen LL, Kreutzer DL. Cytokine expression by head and neck squamous cell carcinomas. Am J Surg. 1992;164:567–73. doi: 10.1016/s0002-9610(05)80708-1. [DOI] [PubMed] [Google Scholar]
- 51.Alevizos I, Mahadevappa M, Zhang X, Ohyama H, Kohno Y, Posner M, et al. Oral cancer in vivo gene expression profiling assisted by laser capture microdissection and microarray analysis. Oncogene. 2001;20:6196–204. doi: 10.1038/sj.onc.1204685. [DOI] [PubMed] [Google Scholar]
- 52.Ardestani SK, Inserra P, Solkoff D, Watson RR. The role of cytokines and chemokines on tumor progression: A review. Cancer Detect Prev. 1999;23:215–25. doi: 10.1046/j.1525-1500.1999.99021.x. [DOI] [PubMed] [Google Scholar]
- 53.Hoffmann TK, Sonkoly E, Homey B, Scheckenbach K, Gwosdz C, Bas M, et al. Aberrant cytokine expression in serum of patients with adenoid cystic carcinoma and squamous cell carcinoma of the head and neck. Head Neck. 2007;29:472–8. doi: 10.1002/hed.20533. [DOI] [PubMed] [Google Scholar]
- 54.St John MA, Li Y, Zhou X, Denny P, Ho CM, Montemagno C, et al. Interleukin 6 and interleukin 8 as potential biomarkers for oral cavity and oropharyngeal squamous cell carcinoma. Arch Otolaryngol Head Neck Surg. 2004;130:929–35. doi: 10.1001/archotol.130.8.929. [DOI] [PubMed] [Google Scholar]
- 55.Giannopoulou C, Kamma JJ, Mombelli A. Effect of inflammation, smoking and stress on gingival crevicular fluid cytokine level. J Clin Periodontol. 2003;30:145–53. doi: 10.1034/j.1600-051x.2003.300201.x. [DOI] [PubMed] [Google Scholar]
- 56.Wang PL, Ohura K, Fujii T, Oido-Mori M, Kowashi Y, Kikuchi M, et al. DNA microarray analysis of human gingival fibroblasts from healthy and inflammatory gingival tissues. Biochem Biophys Res Commun. 2003;305:970–3. doi: 10.1016/s0006-291x(03)00821-0. [DOI] [PubMed] [Google Scholar]
- 57.Sato J, Goto J, Murata T, Kitamori S, Yamazaki Y, Satoh A, et al. Changes in saliva interleukin-6 levels in patients with oral squamous cell carcinoma. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;110:330–6. doi: 10.1016/j.tripleo.2010.03.040. [DOI] [PubMed] [Google Scholar]
- 58.SahebJamee M, Eslami M, AtarbashiMoghadam F, Sarafnejad A. Salivary concentration of TNF-alpha, IL-1alpha, IL6, and IL8 in oral squamous cell carcinoma. Med Oral Patol Oral Cir Bucal. 2008;13:E292–5. [PubMed] [Google Scholar]
- 59.Rhodus NL, Ho V, Miller CS, Myers S, Ondrey F. NF-kappaB dependent cytokine levels in saliva of patients with oral preneoplastic lesions and oral squamous cell carcinoma. Cancer Detect Prev. 2005;29:42–5. doi: 10.1016/j.cdp.2004.10.003. [DOI] [PubMed] [Google Scholar]
- 60.Li Y, St John MA, Zhou X, Kim Y, Sinha U, Jordan RC, et al. Salivary transcriptome diagnostics for oral cancer detection. Clin Cancer Res. 2004;10:8442–50. doi: 10.1158/1078-0432.CCR-04-1167. [DOI] [PubMed] [Google Scholar]
- 61.Katakura A, Kamiyama I, Takano N, Shibahara T, Muramatsu T, Ishihara K, et al. Comparison of salivary cytokine levels in oral cancer patients and healthy subjects. Bull Tokyo Dent Coll. 2007;48:199–203. doi: 10.2209/tdcpublication.48.199. [DOI] [PubMed] [Google Scholar]
- 62.Arellano-Garcia ME, Hu S, Wang J, Henson B, Zhou H, Chia D, et al. Multiplexed immunobead-based assay for detection of oral cancer protein biomarkers in saliva. Oral Dis. 2008;14:705–12. doi: 10.1111/j.1601-0825.2008.01488.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Wei F, Patel P, Liao W, Chaudhry K, Zhang L, Arellano-Garcia M, et al. Electrochemical sensor for multiplex biomarkers detection. Clin Cancer Res. 2009;15:4446–52. doi: 10.1158/1078-0432.CCR-09-0050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Tan W, Sabet L, Li Y, Yu T, Klokkevold PR, Wong DT, et al. Optical protein sensor for detecting cancer markers in saliva. Biosens Bioelectron. 2008;24:266–71. doi: 10.1016/j.bios.2008.03.037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Rhodus NL, Cheng B, Myers S, Miller L, Ho V, Ondrey F. The feasibility of monitoring NF-kappaB associated cytokines: TNF-alpha, IL-1alpha, IL-6, and IL-8 in whole saliva for the malignant transformation of oral lichen planus. Mol Carcinog. 2005;44:77–82. doi: 10.1002/mc.20113. [DOI] [PubMed] [Google Scholar]
- 66.Duffy SA, Taylor JM, Terrell JE, Islam M, Li Y, Fowler KE, et al. Interleukin-6 predicts recurrence and survival among head and neck cancer patients. Cancer. 2008;113:750–7. doi: 10.1002/cncr.23615. [DOI] [PubMed] [Google Scholar]
- 67.Li Y, Zhou X, St John MA, Wong DT. RNA profiling of cell-free saliva using microarray technology. J Dent Res. 2004;83:199–203. doi: 10.1177/154405910408300303. [DOI] [PubMed] [Google Scholar]
- 68.Park NJ, Zhou X, Yu T, Brinkman BM, Zimmermann BG, Palanisamy V, et al. Characterization of salivary RNA by cDNA library analysis. Arch Oral Biol. 2007;52:30–5. doi: 10.1016/j.archoralbio.2006.08.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Jiang J, Park NJ, Hu S, Wong DT. A universal pre-analytic solution for concurrent stabilization of salivary proteins, RNA and DNA at ambient temperature. Arch Oral Biol. 2009;54:268–73. doi: 10.1016/j.archoralbio.2008.10.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Park NJ, Yu T, Nabili V, Brinkman BM, Henry S, Wang J, et al. RNAprotect saliva: An optimal room-temperature stabilization reagent for the salivary transcriptome. Clin Chem. 2006;52:2303–4. doi: 10.1373/clinchem.2006.075598. [DOI] [PubMed] [Google Scholar]
- 71.Zimmermann BG, Wong DT. Salivary mRNA targets for cancer diagnostics. Oral Oncol. 2008;44:425–9. doi: 10.1016/j.oraloncology.2007.09.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Li Y, Elashoff D, Oh M, Sinha U, St John MA, Zhou X, et al. Serum circulating human mRNA profiling and its utility for oral cancer detection. J Clin Oncol. 2006;24:1754–60. doi: 10.1200/JCO.2005.03.7598. [DOI] [PubMed] [Google Scholar]
- 73.Brinkmann O, Kastratovic DA, Dimitrijevic MV, Konstantinovic VS, Jelovac DB, Antic J, et al. Oral squamous cell carcinoma detection by salivary biomarkers in a Serbian population. Oral Oncol. 2011;47:51–5. doi: 10.1016/j.oraloncology.2010.10.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Kumar SV, Hurteau GJ, Spivack SD. Validity of messenger RNA expression analyses of human saliva. Clin Cancer Res. 2006;12:5033–9. doi: 10.1158/1078-0432.CCR-06-0501. [DOI] [PubMed] [Google Scholar]
- 75.Ballantyne J. Validity of messenger RNA expression analyses of human saliva. Clin Cancer Res. 2007;13:1350. doi: 10.1158/1078-0432.CCR-06-2796. author reply 1351. [DOI] [PubMed] [Google Scholar]
- 76.Wong DT. Salivary transcriptome. Clin Cancer Res. 2007;13:1350–1. doi: 10.1158/1078-0432.CCR-06-2227. author reply 1351. [DOI] [PubMed] [Google Scholar]
- 77.Haas C, Klesser B, Maake C, Bar W, Kratzer A. mRNA profiling for body fluid identification by reverse transcription endpoint PCR and realtime PCR. Forensic Sci Int Genet. 2009;3:80–8. doi: 10.1016/j.fsigen.2008.11.003. [DOI] [PubMed] [Google Scholar]
- 78.Juusola J, Ballantyne J. Messenger RNA profiling: A prototype method to supplant conventional methods for body fluid identification. Forensic Sci Int. 2003;135:85–96. doi: 10.1016/s0379-0738(03)00197-x. [DOI] [PubMed] [Google Scholar]
- 79.Juusola J, Ballantyne J. Multiplex mRNA profiling for the identification of body fluids. Forensic Sci Int. 2005;152:1–12. doi: 10.1016/j.forsciint.2005.02.020. [DOI] [PubMed] [Google Scholar]
- 80.Sakurada K, Ikegaya H, Fukushima H, Akutsu T, Watanabe K, Yoshino M. Evaluation of mRNA-based approach for identification of saliva and semen. Leg Med (Tokyo) 2009;11:125–8. doi: 10.1016/j.legalmed.2008.10.002. [DOI] [PubMed] [Google Scholar]
- 81.Seugnet L, Boero J, Gottschalk L, Duntley SP, Shaw PJ. Identification of a biomarker for sleep drive in flies and humans. Proc Natl Acad Sci U S A. 2006;103:19913–8. doi: 10.1073/pnas.0609463104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Palanisamy V, Park NJ, Wang J, Wong DT. AUF1 and HuR proteins stabilize interleukin-8 mRNA in human saliva. J Dent Res. 2008;87:772–6. doi: 10.1177/154405910808700803. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Park NJ, Li Y, Yu T, Brinkman BM, Wong DT. Characterization of RNA in saliva. Clin Chem. 2006;52:988–94. doi: 10.1373/clinchem.2005.063206. [DOI] [PMC free article] [PubMed] [Google Scholar]