

Abstract
Ameloblastomas seldom cause diagnostic difficulties due to classic histopathological presentations. Adenoid ameloblastoma is a rare variant in this category which can cause problem in diagnosis due to the presence of areas resembling adenomatoid odontogenic tumor (AOT) and occurrence of varying degrees of dentinoid formation. In this article, we report a case of adenoid ameloblastoma with dentinoid, which was diagnosed accurately after the third recurrence. To the best of our knowledge, so far, only 13 cases have been reported of tumors that histologically show features of amelobalstoma and AOT with hard tissue formation. The recurrences were due to under diagnosis of the lesion followed by a conservative treatment.
Keywords: Adenoid ameloblastoma, adenomatoid odontogenic tumor, ameloblastoma, dentinoid
INTRODUCTION
Ameloblastoma is the second most common odontogenic tumor, with benign but aggressive clinical behavior. This tumor microscopically presents with classic features and seldom causes diagnostic difficulty. However, ameloblastoma can occasionally demonstrate unusual histopathological features with dentinoid formation.[1]
The adenomatoid odontogenic tumor (AOT), which was previously considered as a variant of ameloblastoma, represents 3–7% of all odontogenic tumors and generally occurs in the maxillary anterior region. Microscopic features of AOT show presence of tubular characteristic and duct-like structures that led to the term “adenoameloblastoma”, which previously used to designate this lesion.[2] Contrary to ameloblastoma, AOT is a circumscribed lesion; it is less aggressive and has limited growth potential. Keeping this in mind, the surgeons generally take a more conservative approach in the treatment of AOT as compared to ameloblastoma. If the treatment of AOT is adequate, the tumor seldom recurs. Of the numerous cases of AOT reported in the literature, only the cases reported by Fukaya et al.[3] and Xiang et al.[4] showed recurrence although Takigami has reported a case of AOT that recurred three times.[5] A thorough review of literature conducted in 2004 concluded that the lesions that are reported as recurrent AOT, are almost certainly adenoid ameloblastoma with dentinoid.[6]
Adenoid ameloblastoma with dentinoid is a rare odontogenic tumor showing histopathological features similar to ameloblastoma and AOT along with hard tissue formation. The occurrence of dentinoid along with ameloblastoma was first reported by Slabbert et al., in 1992.[1] However, the name ‘adenoid ameloblastoma with dentinoid’ was introduced by the Armed Forces Institute of Pathology.[2] Since then only few cases of this entity are reported in literature.
This case report describes a patient with adenoid ameloblastoma with dentinoid involving the maxillary anterior region which was accurately diagnosed only after the third recurrence. The lesion was previously under diagnosed due to its characteristic location, radiographic features and microscopic features which predominantly showed the ductal pattern over shadowing the ameloblastomatous areas.
CASE REPORT
A 45–year-old male patient presented to the out patient department of Yenepoya Dental College with the chief complaint of swelling in upper left anterior region of the jaw since two weeks. The patient gave history of root canal treatment for few teeth in that region and two previous surgeries for similar swellings in the same region. Extra oral examination revealed a diffuse swelling in the left side of the anterior maxillary region. Intra-orally, a well-defined, swelling of about 3 × 1 cm size was observed in relation to the 21 to 23 region causing partial obliteration of vestibule. The surface of the swelling was smooth and no draining sinus or ulceration was seen. The swelling was non-tender on palpation, soft in consistency with a smooth surface [Figure 1].
Figure 1.

Clinical presentation of patient with swelling in upper left vestibule
An Intra Oral Peri Apical (IOPA) radiograph showed a diffuse radiolucency of about 3 × 3 cm in the apical region of 22 and 23 [Figure 2].
Figure 2.

Intra oral peri apical radiograph showing diffuse radiolucency in periapical region of canine and incisors
The findings of IOPA were subsequently confirmed on orthopantomography and occlusal radiographs. A provisional diagnosis of recurrent radicular cyst/AOT was given and enucleation was advised [Figures 3 and 4].
Figure 3.

Ortho pantomogram showing diffuse radiolucency in left incisor and canine region
Figure 4.

Occlusal radiograph showing diffuse radiolucency in left incisor and canine region
Histopathological Features
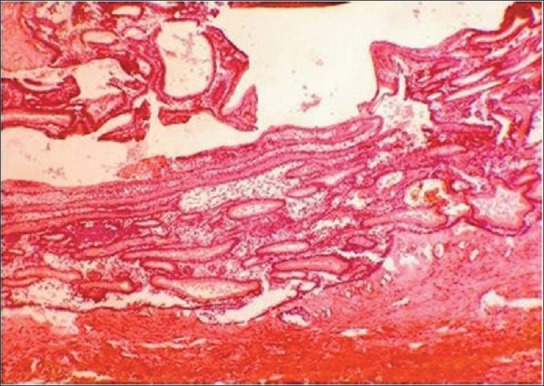
The sections showed densely collagenous connective tissue stroma with scanty areas of odontogenic epithelium, showing characteristic features of a plexiform type ameloblastoma and microcyst formation which resembled the ductal pattern of AOT [Figure 5]. Areas between microcysts demonstrated loose arrangement of cells similar to stellate reticulum. Areas showing few epithelial whorls without cystic degeneration were also seen [Figure 6]. The eosinophilic extracellular material observed was consistent with dentinoid with occasional foci demonstrating tubule formations [Figure 7].
Figure 5.
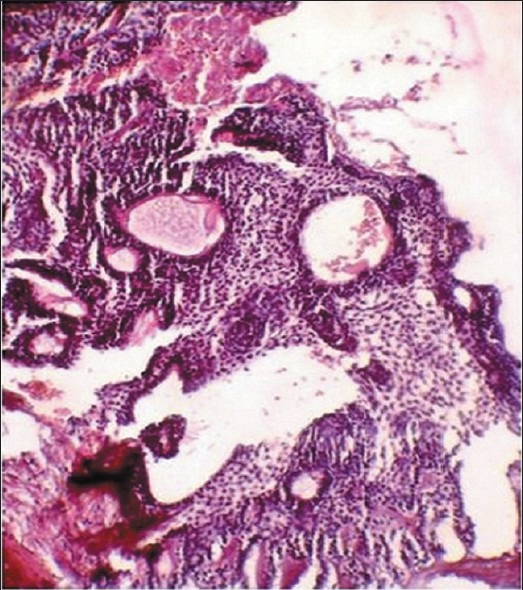
Histological picture showing H and E stained sections with odontogenic cells in plexiform arrangement and microcysts
Figure 6.
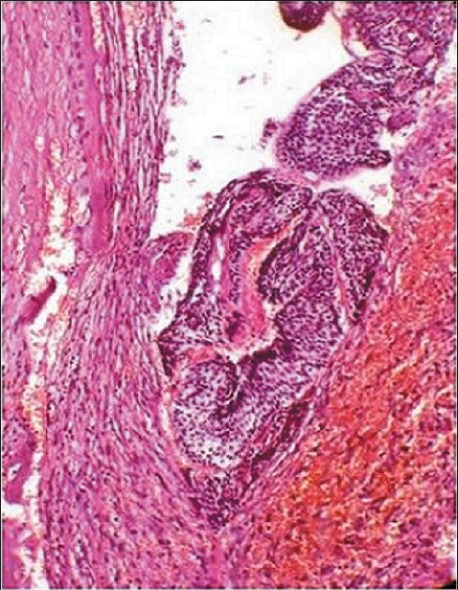
H and E stained sections showing odontogenic cells arranged in whorls
Figure 7.
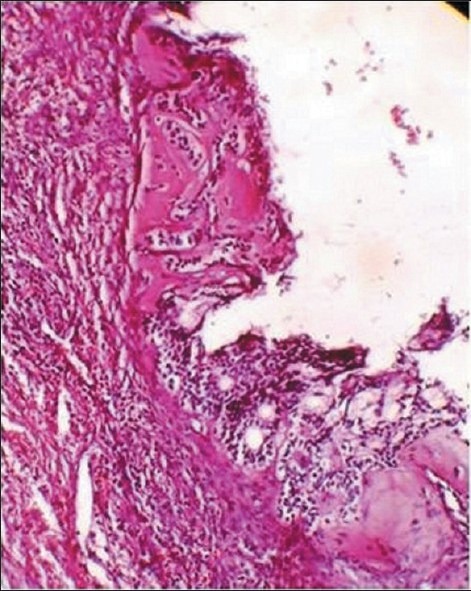
Presence of dentinoid seen as eosinophilic stained material
Considering these features, a provisional histopathological diagnosis of adenoid ameloblastoma with dentinoid or AOT with dentinoid was considered.
Previous biopsy report and microscopic slides were retrieved from the hospital where the previous treatment was performed. On thorough review, the slides revealed areas of ductal patterns of AOT, [Figure 8] with few but distinct areas of plexiform ameloblastoma [Figure 9]. Considering the histopathological features of present and previous tissue sections, the diagnosis of adenoid ameloblastoma with dentinoid was confirmed.
Figure 8.
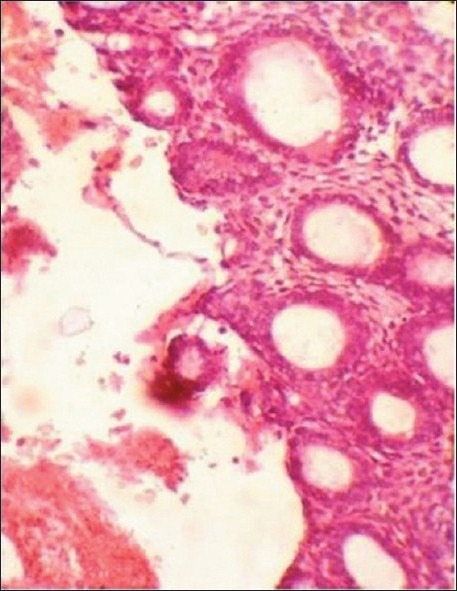
H and E stained sections showing presence of areas with odontogenic cells arranged in ductal pattern
Figure 9.
H and E stained sections showing odontogenic cells in typical plexiform ameloblastoma kind of arrangement
DISCUSSION
While the ameloblastoma is one of the most common odontogenic tumor, adenoid ameloblastoma with dentinoid is an extremely rare occurrence. This unusual odontogenic neoplasm along with dental hard tissue formation was first reported by Slabbert et al., who described a unicystic neoplasm containing typical follicles of ameloblastoma with large amounts of dentinoid and psammomatous-type dystrophic calcifications in an Asian male patient.[1] Although the histopathologic features were well described, the authors has not assigned any specific terminology. Later Armed Forces Institute of Pathology (AFIP) USA, described a similar neoplasm with recurrence potential and suggested the term “adenoid ameloblastoma with dentinoid” for these lesions.[2]
Since then, 13 cases have been reported of tumors that histologically show features of ameloblastoma and AOT along with hard tissue formation. Of these, the cases reported by Slabbert et al,[1] Evans et al,[7] Orlowski et al,[8] Tajima et al,[9] Matsumoto et al[10] and in the present report, the tumor was diagnosed as ameloblastoma, while in six other reports the tumor was considered to be AOT. Teakeda et al reported bone formation in their report[11] while the other cases have mentioned the hard tissue as dentin or dentinoid.
In our case, the lesion was diagnosed previously both clinically and histopathologically as AOT. The clinical diagnosis of AOT was considered due to the typical location, clinical and radiographic presentation, which was histopathologically confirmed after observing the odontogenic epithelium exhibiting typical ductal pattern. The lesion appeared first in 2006 June and enucleation was done. First recurrence was noted in 2007 August and was treated via conservative surgical excision considering the rare possibility of recurrence of AOT. Accurate diagnosis was made and adequate treatment was given only after the third recurrence. Subtotal maxillectomy was done to remove the lesion with part of maxilla. On a regular follow up postoperatively, patient was free of any symptoms.
Although the present case was diagnosed as AOT, the behavior of the lesion actually was typical of an ameloblastoma with local recurrences following subtotal removal. In addition the lesion demonstrated deposition of well formed dentin that showed the presence of dentinal tubules with no evidence of concomitant enamel matrix formation. The use of immunohistochemistry or special stains in the diagnosis of odontogenic tumors is debatable. There are no specific markers to conclusively diagnose the odontogenic lesions included in the current WHO classification, but some studies have shown that cytokeratin 14 and 19 are expressed more frequently by odontogenic epithelium.[12] Additionally, the use of Amelogenin, a protein of enamel matrix has also been employed. More recently, Calretinin, a 29-kDa calcium-binding protein has been shown to be expressed in both unicystic and solid ameloblastomas but not in other types of odontogenic cysts, and this finding led some authors to propose it may be considered a specific immunohistochemical marker for neoplastic ameloblastic epithelium.[12] But since in the present case, the histological picture was fairly conclusive, IHC marker was not used.
After perusing the available literature, striking similarities were observed between the present case and some of the cases previously reported, especially by Evans et al.[3] and Ide et al.[6]
Evans et al.[3] had described a case of a recurrent lesion that was initially diagnosed as AOT after the third recurrence and after reviewing all histologic findings, they named it adenoid ameloblastoma with dentinoid. The tumor demonstrated duct-like structures, epithelial whorls, and dentinoid with foci of tubular dentin.
Ide et al.[6] reported adenoid ameloblastoma with dentinoid in a 44-year-old man who presented with a heart-shaped, unilocular radiolucency in the left globulomaxillary area involving the apex of the central incisor. The lesion was enucleated considering the clinical diagnosis of odontogenic cyst, but was histologically diagnosed as AOT. The lesion was diagnosed as adenoid ameloblastoma with dentinoid, after fourth recurrence.
In general practice, an oral pathologist rarely gets confused between an ameloblastoma and an AOT, as the two lesions have distinct histologic features. But since the adenoid ameloblastoma with dentinoid shows the presence of ductal pattern and dentinoid formation, which is not present in conventional ameloblastoma, it presents a diagnostic dilemma to the oral pathologist. At times, the AOT like areas predominate, which may overshadow the ameloblastomatous areas leading to under diagnosis and conservative treatment, which will ultimately result in recurrence.
Because of the paucity of reported cases of adenoid ameloblastoma with dentinoid, the behavior and appropriate management of these tumors are uncertain. As in case of conventional ameloblastoma, resection may be ideal. Multiple recurrences reported in the literature by Evans et al.[3] and Ide et al.[6] and also as in our case, could have been caused by under diagnosis and inadequate treatment done in presumption of AOT.
Hence, we conclude the present lesion to be a rare case of adenoid ameloblastoma with dentinoid which may be under diagnosed. Therefore, all the pathologists should have a thorough understanding of this entity and review the microscopic slides thoroughly and completely in order to make an accurate diagnosis.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Slabbert H, Altini M, Crooks J, Uys P. Ameloblastoma with dentinoid induction: dentinoameloblastoma. J Oral Pathol Med. 1992;21:46–8. doi: 10.1111/j.1600-0714.1992.tb00969.x. [DOI] [PubMed] [Google Scholar]
- 2.Ghasemi-Moridani S, Yazdi I. Adenoid ameloblastoma with dentinoid: A case report. Arch Iran Med. 2008;11:110–2. [PubMed] [Google Scholar]
- 3.Fukaya M, Sato H, Umakoshi H, Kurauti T, Hanzi J. A case report of adenoameloblastoma on the maxilla. Japanese Journal of Oral Surgery. 1971;17:155–8. doi: 10.5794/jjoms.17.155. [DOI] [PubMed] [Google Scholar]
- 4.Chuan-Xiang Z, Yan G. Adenomatoid odontogenic tumor: A report of a rare case with recurrence. J Oral Pathol Med. 2007;36:440–3. doi: 10.1111/j.1600-0714.2007.00521.x. [DOI] [PubMed] [Google Scholar]
- 5.Takigami M, Uede T, Imaizumi T, Ohtaki M, Tanabe S, Hashi K. A case of adenomatoid odontogenic tumor with intracranial extension. Neurological Surgery. 1988;16:775–9. [PubMed] [Google Scholar]
- 6.Ide F, Mishima K, Saito I, Kusama K. Diagnostically challenging epithelial odontogenic tumors: A selective review of 7 jawbone lesions. Head Neck Pathol. 2009;3:18–26. doi: 10.1007/s12105-009-0107-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Evans BL, Carr RF, Phillipe LJ. Adenoid ameloblastoma with dentinoid: A case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004;98:583–8. doi: 10.1016/j.tripleo.2004.02.077. [DOI] [PubMed] [Google Scholar]
- 8.Orlowski WA, Doyle JL, Salb R. Unique odontogenic tumor with dentinogenesis and features of unicystic plexiform ameloblastoma. Oral Surg Oral Med Oral Pathol. 1991;72:91–4. doi: 10.1016/0030-4220(91)90196-j. [DOI] [PubMed] [Google Scholar]
- 9.Tajima Y, Yokose S, Sakamoto E, Yamamoto Y, Utsumi N. Ameloblastoma arising in calcifying odontogenic cyst. Report of a case. Oral Surg Oral Med Oral Pathol. 1992;74:776–9. doi: 10.1016/0030-4220(92)90407-h. [DOI] [PubMed] [Google Scholar]
- 10.Matsumoto Y, Mizoue K, Seto K. Atypical plexiform ameloblastoma with dentinoid: Adenoid ameloblastoma with dentinoid. J Oral Pathol Med. 2001;30:251–4. doi: 10.1034/j.1600-0714.2001.300410.x. [DOI] [PubMed] [Google Scholar]
- 11.Takeda Y, Kuroda M, Suzuki A. Ameloblastoma with prominent stromal ossification. Acta Pathol Jpn. 1990;40:780–4. doi: 10.1111/j.1440-1827.1990.tb01544.x. [DOI] [PubMed] [Google Scholar]
- 12.Mosqueda-Taylor A. New findings and controversies in odontogenic tumors. Med Oral Patol Oral Cir Bucal. 2008;13:E555–8. [PubMed] [Google Scholar]