

Abstract
Objectives:
To assess areca nut chewing habit among middle school-aged children in Indore, India. Areca nut is chewed by itself, and in various scented preparations. It is associated with carcinogenesis, foreign body aspiration in children, and oral submucous fibrosis and may aggravate asthma.
Materials and Methods:
A retrospective collection of data to evaluate the prevalence of areca nut chewing among 3896 children was done. A simple random sampling was done. Children of both sexes were included in this study.
Results:
27.06% of the school-going children (1054/3896) had areca nut chewing habit. More boys chewed areca nut than girls (2:1). 45.42% of school going children of rural area pander to areca nut chewing habit, whereas in urban area 20.09% children are indulged. Government school children are more involved in areca nut chewing habit. 81.02% of the children used sweetened and flavoured form of areca nut. The majority of the users were not aware of harmful effects that the use of areca nut might be harmful for health
Conclusion:
To diminish the use of areca nut, the Indian Government should consider limiting trade, advertising, and actively communicating its health risks to the public and should deem heavy taxes on it.
Keywords: Areca nut, prevalence, school-going children
Introduction
Areca nut chewing habit is common in India. Areca nut is the fourth most commonly used social drug, ranking after nicotine, ethanol, and caffeine.[1] It is chewed by itself, in various scented preparations and in betel quid in various parts of India.[2] Commercially, areca nut is marketed in the form of sweetened areca nut (locally known as sweet supari) to target young children. A high proportion of school children used areca nut daily in some form. We conducted this study to assess the prevalence of areca nut use, in middle school-going children of Indore, India.
Materials and Methods
A retrospective collection of data was done to evaluate the prevalence of mesiodens conducted, for which the study was carried out on 3896 middle school-going children aged 8–17 years in Indore. A simple random sampling was done; school-going children belonging to different zones of Indore were randomly selected. Children of both sexes were included in the study.
Prior to the study, a letter of permission to examine the school children was given to the concerned head of the schools and the permission was obtained. A letter of information to the parents regarding the examination was sent through the concerned class teachers.
Result
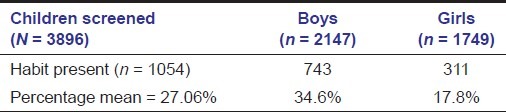
Out of 3896 children surveyed, 2147 were boys and 1749 were girls. 1054 children had areca nut with the mean prevalence of 27.06%. Out of total children who had chewing habit, 743 were boys and 311 were girls. It was observed that the prevalence of areca nut chewing is more in boys than in girls with a ratio of 2:1. The overall prevalence of areca nut among the boys was 34.6%, whereas the overall prevalence among the girls was 17.8% [Table 1].
Table 1.
Age and prevalence of areca nut chewing among school students
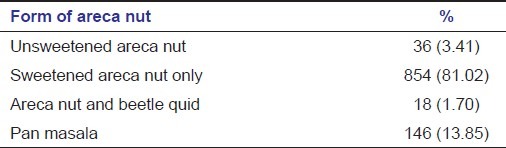
45.42% of school-going children of rural area pander to areca nut chewing habit, whereas in urban area 20.09% children are indulged. Government school children are more involved in areca nut chewing habit [Table 2]. Most of the children are non-regular users [Table 3]. 854 (81.02%) out of 1054 use sweetened areca nut; only 36 used children used unsweetened betel nut alone and most striking was 146 used pan masala [Table 4]. Most of the children used one packet of areca nut per day. “Chanchal” and “Ritik gold” are the common local brand and favorite brand of sweetened and flavored areca nut among the children.
Table 2.
School and distribution of school with areca nut chewing habit
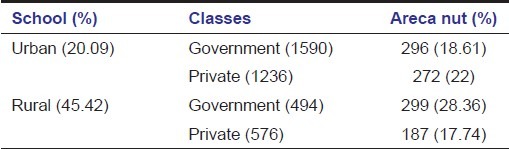
Table 3.
Frequency of use among current users
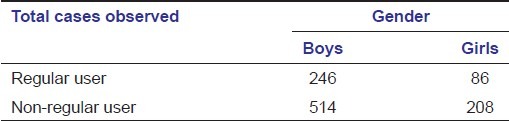
Table 4.
Form of areca nut variety chewed
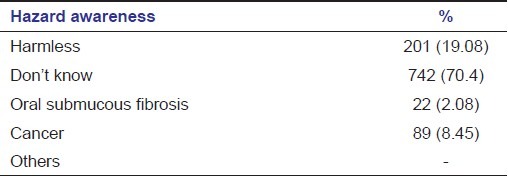
More than half of the users of areca nut reported learning the habit from their friends or siblings [Table 5]. The majority of the users (742; 70.4%) were not aware of harmful effects that the use of areca nut might be harmful for health but few were aware that it may cause cancer or reduced mouth opening [Table 6].
Table 5.
From whom school children learned to use areca nut
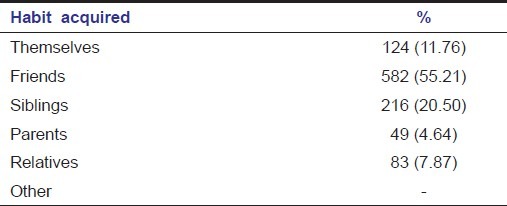
Table 6.
Health hazards awareness among those who chew areca nut
Discussion
Areca nut is an important agricultural product in many regions of the world, which is believed to be native to Sri Lanka, West Malaysia, and Melanesia.[3] In India, production of the nut has risen nearly threefold and may reflect the commercialization of areca products since the early 1980s. In 2001, production of areca nut in India was around 330,000 millions of tonnes.[4]
Areca nut is known as “supari” in India. It is the basic ingredient of a variety of widely used chewed products. Areca nut products are easily available even in the small shops. It plays an integral part of religious, social, and cultural functions. Areca nut is a psychoactive substance used by several hundred million persons worldwide, predominantly in southern Asia.[5] Areca nut is available in processed and unprocessed forms.
The major chemical constituents of the nut are carbohydrates, fats, proteins, crude fiber, polyphenols, alkaloids, and mineral matter.[6] Polyphenols (flavonols, tannins) constitute a large proportion of the dry weight of the nut. Polyphenols are responsible for the astringent taste of the nut. The nut has been shown to contain at least six related alkaloids, of which four (arecoline, arecaidine, guvacine, and guvacoline) have been conclusively identified in biochemical studies.[7] Arecoline is generally the main alkaloid, which is carcinogenic.[8] Application of these substances to human fibroblasts induces fibroblast proliferation and collagen production.[9,10] Areca nut chewing is strongly associated with oral submucous fibrosis, a crippling and precancerous condition.[11–13] Areca nut is implicated in causing oral cancer.[14,15] It has been found to be a common cause of airway obstruction in children leading to emergency admissions with potential fatal complications.[16] Areca nut chewing causes broncho-constriction and may aggravate asthma.[17] Complications of areca nut also include gingivitis, leukoplakia, and staining of teeth and gums.[18] Studies have shown that areca nut chewing is an addictive practice, much like the use of nicotine.[19] The euphoric effects of areca nuts are due to its alkaloid contents such as arecoline, a cholinergic agent and central nervous system stimulant that increases the amount of acetylcholine in the brain, and arecaidine, a hydrolyzed product of arecoline.[20]
Several small surveys conducted in schools and colleges in several states of India have reported that 13–50% of students chew pan masala and gutka[21]; we also found similar array in our study, and the mean prevalence for areca nut chewing among school-going children was found to be 27.06%. More boys chewed areca nut than girls (2:1). 45.42% of school-going children of rural area pander to areca nut chewing habit, whereas in urban area 20.09% children are indulged. Government school children are more involved in areca nut chewing habit. 81.02% of the children used sweetened and flavored form of areca nut. The majority of the users (742) were not aware of harmful effects that the use of areca nut might be harmful for health.[22]
Conclusion
Areca nut use is common among school children in India. Areca nut use by the parents or friends, lack of knowledge on the harmful effects of areca nut products, and elders being indifferent toward this habit affects the younger generation's perception toward high-risk behavior. Areca nut, like cigarettes, is addictive and dangerous. Areca nut use has the potential to cause immense harm to health. Unless effective health actions are undertaken, and known addictive nature, children may carry this insidious habit into adulthood and conceivably to adopt other addictive habits including tobacco use and cigarette smoking.
To diminish the use of areca nut, the Indian Government should consider restraining the trade, advertisements, and should deem heavy taxes on it which would raise its price. Actively communicating its health risks to the public, strategy involving parents, teachers, and local communities could be initiated to discourage areca nut use.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Nelson BS, Heischober B. Betel nut: A common drug used by naturalized citizens from India, Far East, & the South Pacific Islands. Ann Emerg Med. 1990;34:238–43. doi: 10.1016/s0196-0644(99)70239-8. [DOI] [PubMed] [Google Scholar]
- 2.Bhonsle RB, Murti PR, Gupta PC. Tobacco habits in India. In: Gupta PC, Hamner JE III, Murti PR, editors. Control of Tobacco-Related Cancers and Other Diseases. Bombay: Oxford University Press; 1992. pp. 2–46. [Google Scholar]
- 3.Williams S, Malik A, Chowdhury S, Chauhan S. Socio-cultural aspects of areca nut use. Addict Biol. 2002;7:147–54. doi: 10.1080/135562101200100147. [DOI] [PubMed] [Google Scholar]
- 4.2004. pp. 41–49. Monographs.iarc.fr/ENG/Monographs/vol85/mono85.pdf.
- 5.Tobacco habits other than smoking; Betel-quid and areca Nut chewing; and some related nitrosamines. Lyon: International Agency for Research on Cancer; 1984. International Agency for Research on Cancer: IARC Monographs on the evaluation of the carcinogenic risk of chemicals to humans; p. 37. [PubMed] [Google Scholar]
- 6.Jayalakshmi A, Mathew AG. Chemical composition and processing. In: Bavappa KVA, Nair MK, Kumar, editors. The Arecanut Palm, Kerala: Central Plantation Crops Research Institute; 1982. pp. 225–44. [Google Scholar]
- 7.Lord GA, Lim CK, Warnakulasuriya S, Peters TJ. Chemical and analytical aspects of areca nut. Addict Biol. 2002;7:99–102. doi: 10.1080/13556210120091455. [DOI] [PubMed] [Google Scholar]
- 8.Hoffmann D, Rivenson A, Prockopczyk B. Advances in tobacco carcinogenesis. Smokeless tobacco and betel quid. In: Gupta PC, Hamner JE III, Murti PR, editors. Control of Tobacco-Related Cancers and Other Diseases. Bombay: Oxford University Press; 1992. pp. 193–204. [Google Scholar]
- 9.Harvey W, Scut A, Harvey W, Canniff JP. Stimulation of human buccal mucosa fibroblasts from normal and oral submucous fibrosis. Arch Oral Biol. 1986;31:45–9. doi: 10.1016/0003-9969(86)90112-3. [DOI] [PubMed] [Google Scholar]
- 10.Murti PR, Bhonsle RB, Gupta PC. Etiology of oral submucous fibrosis with special reference to the role of areca nut chewing. J Oral Pathol Med. 1995;24:145–52. doi: 10.1111/j.1600-0714.1995.tb01156.x. [DOI] [PubMed] [Google Scholar]
- 11.Maher R, Lee AJ, Warnakulasuriya KA. Role of areca nut in the causation of oral submucous fibrosis: A case-control study in Pakistan. J Oral Pathol Med. 1994;23:65–9. doi: 10.1111/j.1600-0714.1994.tb00258.x. [DOI] [PubMed] [Google Scholar]
- 12.Prokopczyk B, Rivinson A, Hoffmann D. A study of betel quid carcinogenesis. Cancer Lett. 1991;60:153–7. doi: 10.1016/0304-3835(91)90222-4. [DOI] [PubMed] [Google Scholar]
- 13.Adhvaryu SG, Dave BJ, Trivedi AH. Cytogenic surveillance of tobacco-areca nut chewers, including patients with oral cancers and premalignant conditions. Mutat Res. 1991;261:41–9. doi: 10.1016/0165-1218(91)90096-5. [DOI] [PubMed] [Google Scholar]
- 14.Thomas SJ, Maclennan R. Slaked lime and betel nut cancer in Papua New Guinea. Lancet. 1992;340:577–8. doi: 10.1016/0140-6736(92)92109-s. [DOI] [PubMed] [Google Scholar]
- 15.Gupta PC. Betel quid and oral cancer: Prospects for prevention. IARC. 1991;105:466–70. [PubMed] [Google Scholar]
- 16.Tariq P. Foreign body aspiration in children: A persistent problem. J Pak Med Assoc. 1999;49:33–6. [PubMed] [Google Scholar]
- 17.Taylor RF, Al-Jarad N, John LM, Conroy DM, Barnes NC. Betel-nut chewing and asthma. Lancet. 1992;339:1134–6. doi: 10.1016/0140-6736(92)90732-i. [DOI] [PubMed] [Google Scholar]
- 18.Norton SA. Betel nut: Consumption and consequences. J Am Acad Dermatol. 1997;37:81–8. doi: 10.1016/s0190-9622(98)70543-2. [DOI] [PubMed] [Google Scholar]
- 19.Burton-Bradley BG. Papua and New Guinea transcultural psychiatry: Some implications of betel chewing. Med J Aust. 1966;2:744–6. doi: 10.5694/j.1326-5377.1966.tb97486.x. [DOI] [PubMed] [Google Scholar]
- 20.Holmstedt B, Lindgren G. Arecoline, nicotine, and related compounds: Tremorgenic activity and effect upon brain acetylcholine. Ann N Y Acad Sci. 1967;142:126. [Google Scholar]
- 21.Gupta PC, Ray CS. Smokeless tobacco and health in India and South Asia. Respirology. 2003;8:419–31. doi: 10.1046/j.1440-1843.2003.00507.x. [DOI] [PubMed] [Google Scholar]
- 22.Gupta PC, Ray CS. Epidemiology of Betel quid usage. Ann Acad Med Singapore. 2004;33(4 Suppl):31–6. [PubMed] [Google Scholar]