

Abstract
Objective:
To compare the accuracy of linear measurements on lateral and frontal cephalograms with gold standard skull measurements.
Materials and Methods:
Based on the specific criteria including reliable occlusion and condyles fitting in glenoid fossa, 15 dry human skulls were selected from a larger collection. Lateral and frontal cephalograms were taken of each skull by standardized methods. Steel ball bearings were used to identify the anatomic landmarks. Linear measurements in midsagittal plane were made on all three records. Intraclass correlation coefficients, Pearson's correlation coefficient and regression constant were calculated to assess the records simultaneously.
Results:
The frontal cephalometric measurements showed high correlation to the direct skull measurements (Pearson's coefficient 0.943<r<0.998)
Conclusions:
The linear measurements of the lateral cephalometric record are greater than the corresponding frontal cephalometric images. The overall findings of the present study showed that the frontal cephalometric measurements are closely related to the direct skull measures.
Keywords: Cephalometrics, frontal cephalograms, lateral cephalograms, skull measurements
Introduction
Radiographic imaging is an important adjunct in the assessment of skeletal and dental relationships for the orthodontic patient. Imaging is one of the most ubiquitous tools used by orthodontists to measure and record the size and form of craniofacial structures. It is used to record the status quo of limited or grouped anatomic structures. Despite the diverse image acquisition technologies currently available, standards have been adopted in an effort to balance the anticipated benefits with associated costs and risks. The erroneous assumptions inherent in traditional two dimensional cephalometry questioned the method for deriving clinical information as a basis for planning treatment.[1–3]
The scientific value of these analyses was questioned by Han et al.[4] Vig[5] doubted the lack of validity that cephalometric radiographs as a diagnostic instrument, and demonstrated that conclusions drawn on the basis of the same cephalograms may vary significantly depending on the analyses used. The cumulative errors associated with traditional two-dimensional cephalometry have been significant enough to affect diagnosis and treatment planning.[6]
Objective of this study
To compare the linear accuracy and reliability of lateral and frontal cephalometric measurements with the direct skull measurements.
Materials and Methods
The sample consisted of 15 dry dentate human skulls from the Department of Anatomy, Mamata Medical College, Khammam.
The skulls were selected from a larger collection according to criteria of reliable and reproducible occlusion, adult age on the basis of a permanent dentition, partial extractions, and presence of at least one molar on either side to maintain the vertical dimension.
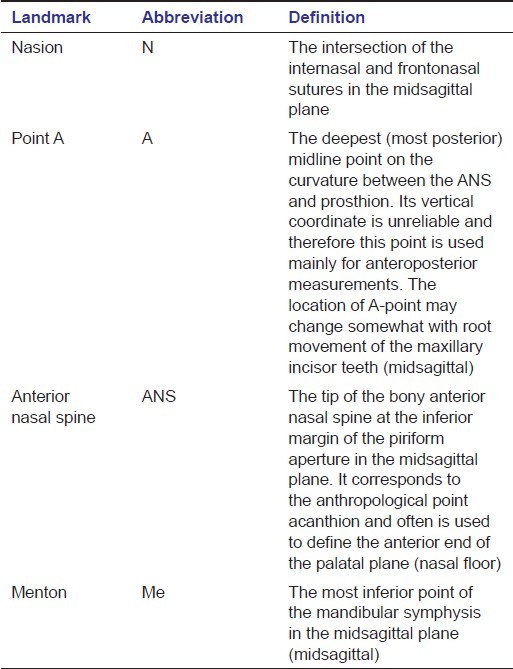
The mandible was stabilized to the maxilla on the basis of occlusal interdigitation or at least maximal contact, and condyles seating in the glenoid fossa, and was secured in this position with masking tape. Four landmarks in the midsagittal plane are identified. Each anatomical landmark is marked by a steel ball bearing of 5/32”. The operational definitions of the land marks are tabulated in Table 1. For all the images in lateral and frontal cephalograms, the teeth are placed in centric occlusion.
Table 1.
Definition of craniometric surface landmarks used in the cephalometric analysis
Each skull was placed in the cephalostat (Rotograph Plus MR05, Villa System Medical, Italy) with ear rods in the external auditory meatus. The distance between the film and mid sagittal plane for lateral cephalogram or porionic plane for posteroanterior radiograph is fixed at 15 cm.
To ensure that the Frankfurt plane is parallel to the floor, the skull was secured to the cephalostat with masking tape. Lateral and frontal radiographs were taken simultaneously for each skull. The radiographic settings used were 85 kvp, 15mA, 3s. The radiographs were traced on acetate paper using the same view box and using Staedtler Mars Micro 0.3mm 2H pencil.
Linear measurements were made on the cephalometric tracings, and directly on the skulls for readily measurable distances. The distances measured are tabulated in Table 2. The mid sagittal measurements are measured with vernier calliper with least count of 0.01mm
Table 2.
Definition of linear distances used in the cephalometric analysis

Statistical methods
The statistical methods employed for the study are intraclass correlation coefficient, Pearson's correlation coefficient, and regression constant.
The intraclass correlation (or the intraclass correlation coefficient, abbreviated ICC) is a descriptive statistic test that can be used when quantitative measurements are made on units that are organized into groups. It describes how strongly units in the same group resemble each other. The most common measure of “correlation” or “predictability” is Pearson's coefficient of correlation. Pearson's r, as it is often symbolized, can have a value anywhere between -1 and 1. The larger r, ignoring sign, the stronger the association between the two variables and the more accurately one can predict a variable from knowledge of the other variable.
Results
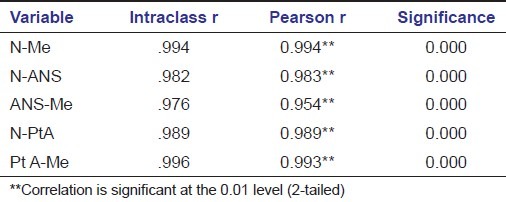
Intra examiner reliability was high for frontal (intraclass coefficient 0.938<r<0.998) and lateral cephalometric measurements (intraclass Coefficient 0.908<r<0.991) [Table 3]. Highest intraclass correlations were observed for frontal cephalometric measurement Pt A – Me (r = .998) [Figure 1] [Table 4]. Pearson's correlation coefficients were similar to intraclass correlations for most of the measurements [Figures 2 and 3] [Table 5]. High intraclass coefficient indicates near similarity between the means of the two records, whereas high Pearson's correlation coefficients reflect variation in direction about the records mean values. All calculations were performed on SPSS (version 14, SPSS, Chicago III).
Table 3.
Comparison of direct skull and lateral cephalogram measurements
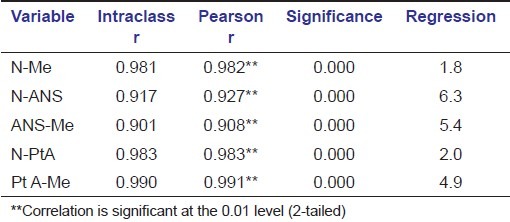
Figure 1.

Pt A-Me measurements
Table 4.
Comparison of direct skull and frontal cephalogram measurements
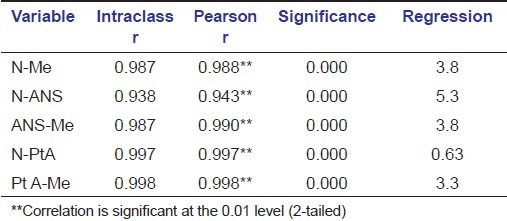
Figure 2.

N-Pt A measurements
Figure 3.

ANS-Me measurements
Table 5.
Comparison of frontal and lateral cephalogram measurements
Discussion
The cephalometric images are the 2D interpretation of the 3D structures. In cephalometry, the X-ray source is fixed at a distance of five feet from the mid sagittal plane, and the film is placed at a distance of 15 cm from the mid sagittal plane. The cephalometric image magnification is directly related to the distance between the object and the film. The distance between the source and the object is relatively larger (5 feet) than the object to film distance (15 cm); therefore, the magnification of the anatomical landmarks oriented in all three dimensions of space is minimized. In lateral and frontal cephalograms, many structures overlap as complex 3D structures are projected on a 2D plane. The magnification and distortion inherent to conventional radiography makes it difficult to accurately assess the patient's anatomy.[7] The properly adjusted cephalostat cannot prevent slight translation or rotation of the midsagittal plane. These variations in skull position may lead to variations in cephalometric measurements.[8] In our study, the linear measurements of the lateral cephalometric record were greater than the corresponding frontal cephalograms. The magnification factor for conventional cephalograms is calculated by the distance between the source and the midsagittal plane of the cephalostat (5 feet or 152.4cm); the distance between the receptor and the midsagittal distance (15 cm).[8] The magnification factor for the cephalometric machine is 6.84%. Highest distortion was observed with N-ANS [Figure 4] measurement. The present data of increased vertical dimensions on lateral cephalograms is in accordance with Chidac,[9] in which there was an increase of 8.5%. This study correlates with the conclusions of Tng et al,[10] that the distance between the N-Me [Figure 5] was invalid.
Figure 4.

N-ANS measurements
Figure 5.

N-Me measurements
Conclusion
The linear measurements of the lateral cephalometric record are greater than the corresponding frontal cephalogram measurements. The overall findings of the present study show that the frontal cephalometric measurements are closely related to the direct skull measures.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Bookstein F. The geometry of craniofacial invariants. Am J Orthod. 1983;83:221–34. doi: 10.1016/0002-9416(83)90086-6. [DOI] [PubMed] [Google Scholar]
- 2.Hixon E. The norm concept in cephalometrics. Am J Orthod. 1956;42:898–906. [Google Scholar]
- 3.Moyers R, Bookstein F. The inappropriateness of conventional cephalometrics. Am J Orthod. 1979;75:599–617. doi: 10.1016/0002-9416(79)90093-9. [DOI] [PubMed] [Google Scholar]
- 4.Han U, Vig K, Weintraub J, Vig P, Kowalski C. Consistency of orthodontic treatment decisions relative to diagnostic records. Am J Orthod Dentofacial Orthop. 1991;100:212–19. doi: 10.1016/0889-5406(91)70058-5. [DOI] [PubMed] [Google Scholar]
- 5.Vig P. Orthodontic contraversies: Their origins, consequences and resolution. In: Melsen B, editor. Current Contraversies in Orthodontics. Chicago: Quintessence Publishing; 1991. pp. 269–310. [Google Scholar]
- 6.Gron P. A geometric evaluation of image size in dental radiography. J Dent Res. 1960;39:289–301. doi: 10.1177/00220345600390021101. [DOI] [PubMed] [Google Scholar]
- 7.Grayson B, Cutting C, Bookstein F, Kim H, McCarthy J. The threedimensional cephalogram: theory, technique, and clinical application. Am J Orthod Dentofacial Orthop. 1988;94:327–37. doi: 10.1016/0889-5406(88)90058-3. [DOI] [PubMed] [Google Scholar]
- 8.Kumar V, Ludlow J, Mol A, Cevidanes L. Comparison of conventional and cone beam CT synthesized cephalograms. Dentomaxillofac Radiol. 2007;36:263–69. doi: 10.1259/dmfr/98032356. [DOI] [PubMed] [Google Scholar]
- 9.Chidiac J, Shofer F, Al-Kutoubi A, Laster L, Ghafari J. Comparison of CT scanograms and cephalometric radiographs in craniofacial imaging. Orthod Craniofacial Res. 2002;5:104–13. doi: 10.1034/j.1600-0544.2002.01170.x. [DOI] [PubMed] [Google Scholar]
- 10.Tng TT, Chan T, Hagg U, Cooke M. Validity of cephalometric landmarks. An experimental study. Euro J Orthod. 1994;16:110–20. doi: 10.1093/ejo/16.2.110. [DOI] [PubMed] [Google Scholar]