

Abstract
Here we report a case of adenomatoid odontogenic tumor (AOT) in the maxilla in a young girl aged 14 years and its surgical management. We also review the literature and variations in the nomenclature and classifications of this interesting tumor. The review of literature gives an interesting picture regarding terminologies in the past and dilemma in classifying this tumor. The introduction of the name adenomatoid odontogenic tumour has resulted in the simpler and fruitful surgical management like enucleation and curettage with no reports of recurrences. In the past, similar lesion with the terminology like adeno ameloblastoma has resulted in unnecessary mutilating surgery. The conflicting views whether the lesion is being neoplasm or an anomalous hamartomatous growth is also being discussed.
Keywords: Adenomatoid odontogenic cyst, adenomatoid odontogenic tumor, hamartoma
Introduction
Adenomatoid odontogenic tumor (AOT) is an uncommon benign odontogenic lesion that affects young patients associated with an impacted tooth, usually canine. AOT represents 3–7% of all odontogenic tumors.[1–3]
The histogenesis of AOT is still uncertain and sometimes categorized as a hamartomatous lesion. The tumor is sometimes referred as Two Third's tumor become it occurs in the maxilla in about 2/3 cases, about 2/3 cases in young females, 2/3 case associated with impacted tooth, 2/3 case affected tooth is canine.[4]
Review of Literature
In the past, various names have been used for cases similar to AOT in the literature.
In 1909 James and Forbes from England reported a case of epithelial odontome which is similar to AOT.[5]
In 1915 Harbitz of Norway reported a case of cystic adamantoma.[5]
In 1916 Wohl of Omaha reported AOT-like case as tooth germ cyst of the jaw (or chorioblastoma)[5]
In 1948 stafne reported first series of AOT under the title epithelial tumors associated with developments cyst of maxilla.
Bernier and Tiecke were the first to publish a case using the name adeno ameloblastoma.[6]
In 1968 Abrams et al suggested the term odontogenic adenomatoid tumor.
In 1969 Philipson and Birn proposed the name adenomatoid odontogenic tumor.[7]
Later the AOT was adopted in the initial edition of World Health Organization (WHO)'s histological typing of odontogenic tumor, jaw cysts, and allied lesion in 1971[8] and retained in the 2nd edition of WHO in 1992.
In 1998 Reichart and Philipsen presented the update on AOT based on more than 600 cases in their recent reference work “Odontogenic Tumour and Allied Lesions”.[9]
Case Report
A 14-year-old female child reported to our clinic with a complaint of missing teeth in the right maxilla with a medical history taking epileptic drugs.
Extra oral examination
There is diffused swelling involving right anterior maxilla with moderate obliteration of nasolabial fold [Figure 1].
Figure 1.

Intra-oral view
Intra oral examination
There is a smooth circumscribed swelling 2 cm × 3 cm size, with well-defined margins in the right maxillary region obliterating the buccal vestibule. The buccal cortex is expanded and the surface of the swelling is smooth. Mild tenderness is present. The consistency is firm and fluctuation of the cortex in one area is present. The teeth 13, 14, and 15 were missing. Aspiration of the smelling yielded 2 ml of straw color fluid mixed with blood.
Radiographic findings
Well-circumscribed radiolucent lesion same in right maxilla with impacted teeth 13 and 14, with well-defined radio-opaque border. [Figure 2] Radiograph clearly showed the juxta position of the impacted canine and premolar with flakes of calcifications inside the lesion [Figure 3].
Figure 2.

OPG showing circumscribed radio-lucent lesion with calcifications and impacted teeth
Figure 3.
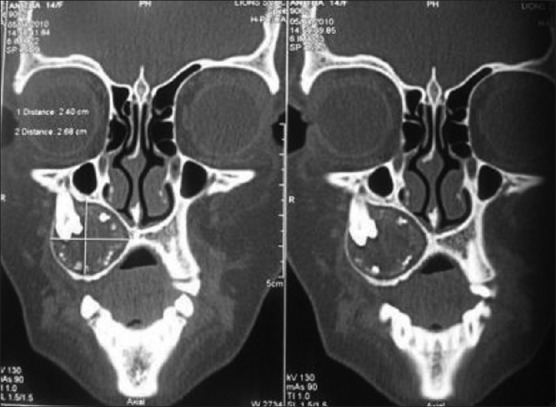
CT—coronal sections
Computed tomography findings
Well-defined cystic lesions present with impacted premolor and canine. There are flakes of radio-opaque areas inside the lesion
Differential diagnosis
Dentigerous cyst
Adenomatoid odontogenic tumor
Calcifying odontogenic cyst
Discussion
AOT usually occurs within the tooth bearing areas of jaws and often found in association with impacted teeth.
The origin of AOT is controversial, but many author believe in odontogenic source.
AOT has cytological features similar to various components of enamel organ, dental lamina, reduced enamel epithelium, and its remnants.[4]
Radiographically, AOT frequently looks like a dentigerious cyst. The lesion is usually unilocular and radiolucent. However, they contain fine calcifications (snowflake), a feature that may be helpful in differentiating an AOT from dentigerious cyst. The unilocular radiolucency is well demarcated with smooth cortical border. Most lesions are pericoronal, juxta coronal, and divergence of roots and displacement of teeth often occurs without root resorption.[2,3,10,11]
Radiographic differential diagnosis:[4]
Dentigerious cyst
Califying odontogenic cyst
Calcifying odontogenic tumor
Uni cystic ameloblastoma
Odontogenic kerato cyst
Microscopic features:[2]
AOT is usually surrounded by a well-developed connective tissue capsule. It may present as a solid mass, a single large cystic space, or as numerous small cystic spaces. The tumor is composed of spindle-shaped or polygonal cells forming sheets and whorled masses in a scant connective tissue stroma. Between the epithelial cells as well as in the center of rosette-like structures is amorphous eosinophilia material. The characteristic duct-like structures is lined by a single row of columnar epithelial cells, the nuclei of which are polarized away from the central lumen. The lumen may be empty or contain amorphous eosinophilic material. Dystrophic calcifications in varying amounts and in different forms are usually encountered in AOTs, within the lumen of duct-like structures, scattered among epithelial masses, or in the stroma.[4]
Summary and Conclusion
Even though enucleation and curettage for AOT is the most common treatment modality, accurate histological diagnosis is mandatory to avoid unnecessary mutilating surgery.
Still the search for accurate classification and ideal nomenclature for AOT continues.
The debate as to whether AOT is an anomalous hamartomatous growth or a true benign neoplasm has not been settled yet.[1] Immunohistochemical studies by certain authors reinforce the theory of hamartomatous character of this lesion indicating AOT is not a true neoplastic lesion.[12]
Some authors prefer to disagree with the term AOT.[13] According to Marx and Stern, the more appropriate term is adenomatoid odontogenic cyst (AOC).[13] The term adonomatoid odontogenic cyst as suggested by Marx and Stern is controversial. But in our case presented, the presence of unilocular cystic lesion, fluid on aspiration, and cystic cavity on transection has to some extent support the terminology adenomatoid odontogenic cyst (AOC) as termed by Marx and Stern.[13]
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Rick GM. Adenomatoid odontogenic tumor. Oral Maxillofac Surg Clin North Am. 2004;16:333–54. doi: 10.1016/j.coms.2004.04.001. [DOI] [PubMed] [Google Scholar]
- 2.Rajendran R. In: Shafer's Text book of Oral Pathology. 6th ed. Rajendran R, Sivapathasundharam B, editors. Noida(India): ELSEVIER; 2009. pp. 282–83. [Google Scholar]
- 3.Oral and Maxillofacial Pathology- Neville, Damm, Allen & Bouquot. 2nd ed. New Delhi(India): ELSEVIER; 2005. pp. 621–25. [Google Scholar]
- 4.Garg D, Palaskar S, Shetty VP, Bhushan A. Adenomatoid odontogenic tumor – harmartoma or true neloplasm: a case report. J Oral Sci. 2009;51:155–9. doi: 10.2334/josnusd.51.155. [DOI] [PubMed] [Google Scholar]
- 5.Sato D, Matsuzaka K, Yama M, Kakizawa T, Inoue T. Adenomatoid Odontogenic Tumor arising from the manidibular molar region: A case report of the literature. Bull Tokyo Dent Coll. 2004;45:223–7. doi: 10.2209/tdcpublication.45.223. [DOI] [PubMed] [Google Scholar]
- 6.Bernier JL, Tiecke RW. Adenoameloblastoma; report of nine cases. Oral Surg Oral Med Oral Pathol. 1956;9:1304–17. doi: 10.1016/0030-4220(56)90232-8. [DOI] [PubMed] [Google Scholar]
- 7.Philipsen HP, Birn H. The adenomatoid odontogenic tumor. Ameloblastic adenomatoid tumour or adeno-ameloblastoma. Acta Pathol Microbiol Scand. 1969;75:375–8. [PubMed] [Google Scholar]
- 8.Pindborg H, Kramar IR. (International Histological classification of tumors. (No.5)) Geneva, Switzerland: World Health Organization; 1971. Histological typing of odontogenic tumors, jaw cysts, and allied lesions. [Google Scholar]
- 9.Reichart PA, Philipsen HP. Odontogenic Tumor facts and figures. Oral Oncol. 1998;35:125–31. doi: 10.1016/s1368-8375(98)00111-0. [DOI] [PubMed] [Google Scholar]
- 10.Philipsen HP, Reichart PA, Zhang KH, Nikai H, Yu QX. Adenomatoid odontogenic tumor: biologic profile based on 499 cases. J Oral Pathol Med. 1991;20:149–58. doi: 10.1111/j.1600-0714.1991.tb00912.x. [DOI] [PubMed] [Google Scholar]
- 11.Reichart PA, Philipsen HP. Odontogenic Tumors and allied lesions. London: Quintessence Publishing Co, Ltd; 2004. pp. 105–15. [Google Scholar]
- 12.Vera Sempere FJ, Artes Martínez MJ, Vera Sirera B, Bonet Marco J. Follicular adenomatoid odontogenic tumor: immunihistochemical study. Med Oral Patol Oral Cir Bucal. 2006;11:E305–8. [PubMed] [Google Scholar]
- 13.Marx RE, Stern D. Oral and Maxillofacial Pathology. Illinois: Quintessence Publishing Co, Inc; 2003. p. 877. [Google Scholar]