

Abstract
Renal metastases from thyroid carcinoma are very rare, late recurrences of papillary thyroid carcinomas (PTC) are not reported in literature and there is no universal recommendation for optimum duration of follow-up of thyroid carcinoma. We present herein a case of late renal recurrence of follicular variant PTC (FV-PTC). This study is a case report of renal metastasis revealing a late recurrence of FV-PTC. An 81-year-old woman with previously treated FV-PTC 24 years ago by total thyroidectomy, lymph nodes dissection and radioiodine therapy presented with sudden gross-hematuria. Computerized tomography scan (CT-scan) revealed a 70-mm right renal mass and histological diagnosis after nephrectomy demonstrated recurrence of FV-PTC with a positive thyroglobulin immunostaining. Despite of 131I-radioiodine therapy postoperatively, the serum thyroglobulin (Tg) increased and positron emission tomography combined to CT-scan showed 4 years later, an abdominal lymph node and distant metastases. Now the patient is alive but her general condition is too poor for systemic adjuvant therapy. This case illustrates the need of prolonged follow-up after surgery of high-risk FV-PTC.
Keywords: Late recurrence, renal metastasis, thyroid carcinoma
Introduction
Papillary thyroid carcinoma (PTC) is the most common cause of thyroid cancers. Surgery, 131I radioiodine therapy and TSH suppression represent the three main treatments of high risk thyroid differentiated carcinomas. After achieving a complete remission, cost effectiveness of patient follow up decreases considerably with time since late recurrences are very rare. There is no universal recommendation for optimum duration of follow up of thyroid carcinoma. We report an original case of renal metastasis revealing a FV PTC recurrence 24 years after initial therapy.
Case Report
In 1982, a 59 year old female patient with left cervical lymph nodes from follicular variant papillary thyroid carcinoma (FV PTC) was treated by total thyroidectomy, lymph nodes dissection (pT1aN1b) and 131I radioiodine remnant ablation (3.7GBq). Post therapy whole body scan (RxWBS) revealed a thyroid bed uptake. At the first follow up control, hypothyroid serum thyroglobulin (hypo Tg) and diagnostic radioiodine whole body scan (DxWBS) were negative.
During the follow up, serum TSH was maintained suppressed. The DxWBS and measurements of hypo Tg were performed annually after thyroid hormone withdrawal from 1 to 5 years postablation, at 8 and at 12 years and remained normal. After 12 years, the patient was considered as cured and no additional work up was performed.
In 2006, 24 years after the resection of primary tumor, the patient presented with sudden gross hematuria and was referred to Urology department. Computerized tomography scan identified a 70mm mass of the superior polar region of right kidney. The patient then underwent radical nephrectomy. The tumor corresponded to renal metastasis from a FV PTC. After nephrectomy, hypo Tg was low (3.2 ng/ml, equivalent CRM 457), 18F FDG PET/CT and Rx WBS were normal. Four years later, the disease progressed with abdominal aorta cava lymph node recurrence diagnosed on 18F FDG PET/CT [Figure 1] and distant metastases despite additional adjuvant treatments with radioiodine. The patient is now alive but her general condition is considered to be too poor for systemic adjuvant therapy.
Figure 1.
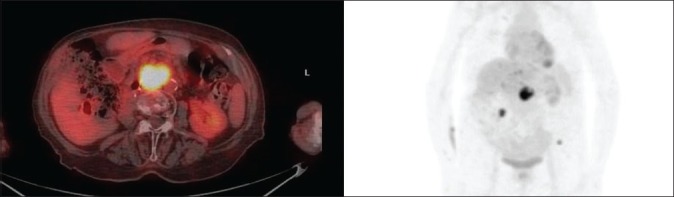
PET-CT scan performed 4 years after the renal recurrence. This figure demonstrated abdominal aorta-cava lymph node with a diameter of 30 mm which appeared 4 years after the renal recurrence despite additional adjuvant treatments with radioiodine.
Discussion
Renal metastases of thyroid carcinomas represent a rare clinical presentation of thyroid cancers recurrences. These metastases have been previously described in literature, usually occurring in presence of others tumor sites[1,2] and represent 2.5 2.7% of all metastases to the kidney.[3] Among the 19 cases of renal metastases from differentiated thyroid carcinomas described in literature, there are two cases of late recurrences revealed by renal metastases from follicular carcinomas.[4,5] In the reported cases, the remission duration ranged 0 37years (Mean±SD: 7.75±11.35). Patients were female in 83.3%. The renal metastases were revealed by hematuria in 16.7%, abdominal pain in 11.1%, palpable mass in 11.1% and incidentally discovered at imaging in 55.5% or autopsy in 5.6%.
In our case, PTC belongs to the family of FV PTCs which are known to carry a poorer prognosis than classic forms of PTC. In contrast to our case, previous renal metastases were associated with other tumor metastases. The pathogenesis of late metastases from thyroid carcinomas without local recurrence suggests an early metastatic spread from the primary tumor. Only very few of the many cells that migrate from the primary tumor are able to escape from apoptosis and survive in the host tissue.[6] It has been demonstrated that cells could establish long term residence in host tissue until development of macroscopic metastases.[7] It is probable that the kidney could provide a favorable microenvironment to cell survival. The low TSH value should have limited the proliferation and expansion of metastatic cells during follow up.
Conclusions
This case illustrates the need of prolonged follow up after surgery of high risk Follicular variant PTC. In these cases, when monitoring should be stopped?
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Lam KY, Ng WK. Follicular carcinoma of the thyroid appearing as a solitary renal mass. Nephron. 1996;73:323–4. doi: 10.1159/000189065. [DOI] [PubMed] [Google Scholar]
- 2.Moudouni S, En-Nia I, Rioux-Leclerc N, Patard JJ, Guille F, Lobel B. Renal metastasis of thyroid carcinoma. Prog Urol. 2001;11:670–2. [PubMed] [Google Scholar]
- 3.Davis RI, Corson JM. Renal metastases from well differentiated follicular thyroid carcinoma: a case report with light and electron microscopic findings. Cancer. 1979;43:265–8. doi: 10.1002/1097-0142(197901)43:1<265::aid-cncr2820430138>3.0.co;2-e. [DOI] [PubMed] [Google Scholar]
- 4.Johnson MW, Morettin LB, Sarles HE, Zaharopoulos P. Follicular carcinoma of the thyroid metastatic to the kidney 37 years after resection of the primary tumor. J Urol. 1982;127:114–6. doi: 10.1016/s0022-5347(17)53634-4. [DOI] [PubMed] [Google Scholar]
- 5.Marino G, Cocimano V, Taraglio S, Testori O. Metastasis of thyroid carcinoma: A rare case of secondary renal tumor. Minerva Urol Nefrol. 1991;43:85–8. [PubMed] [Google Scholar]
- 6.Mehlen P, Puisieux A. Metastasis: A question of life or death. Nat Rev Cancer. 2006;6:449–58. doi: 10.1038/nrc1886. [DOI] [PubMed] [Google Scholar]
- 7.Podsypanina K, Du YC, Jechlinger M, Beverly LJ, Hambardzumyan D, Varmus H. Seeding and propagation of untransformed mouse mammary cells in the lung. Science. 2008;321:1841–4. doi: 10.1126/science.1161621. [DOI] [PMC free article] [PubMed] [Google Scholar]