

Abstract
Background/aims
Chronic hepatitis B (CHB) infection is a serious public health problem due to its potential liver disease sequelae and highly expensive medical costs such as the need for liver transplantation. The aim of this study was to quantify the burden of active CHB in terms of mortality and morbidity, the eligibility of antiviral treatment and to assess various treatment scenarios and possible salvage combinations for cost-effectiveness.
Methods
A population cohort from a large data base of chronic hepatitis B patients was constructed and stratified according to 10-year age groups, the prevalence of HBsAg, HBV DNA level, ALT level, HBeAg status and the presence of cirrhosis. An age-specific Markov model for disease progression and cost-effectiveness analysis was constructed and calibrated for the specific population setting.
Results
Of about 3.2 million estimated HBsAg carriers, 25 % are eligible for treatment. If the active cohort remains untreated, 31 % will die due to liver related complications. Within a 20-year period, 11 % will have developed decompensated cirrhosis, 12 % liver cancer and 6 % will need liver transplantation. Quality adjusted life years (QALYs) for the no treatment scenario ranged from 9.3 to 14.0. For scenarios with antiviral treatment, QALYs ranged from 9.9 to 14.5 for lamivudine, 13.0–17.5 for salvage therapy, and 16.6–19.0 for the third generation drugs entecavir and tenofovir.
Conclusion
In a country with considerable amount of active CHB patients, monotherapy with a highly potent third generation drug has the most health-gain, and is cost-effective in both HBeAg-positive and negative in all stages of liver disease.
Electronic supplementary material
The online version of this article (doi:10.1007/s10198-012-0413-8) contains supplementary material, which is available to authorized users.
Keywords: Chronic hepatitis B, Cost-effectiveness analysis, Antiviral therapy, Turkey, Middle income
Introduction
Chronic hepatitis B (CHB) is a major global public health problem and an important cause of morbidity and mortality from sequelae related to CHB which includes cirrhosis development, decompensation and hepatocellular carcinoma [1].
Antiviral therapy is the only option to control and prevent progression of disease in chronic patients. The indications are generally the same for HBeAg-positive and negative patients. These are based mainly on the combination of three criteria: serum HBV DNA and ALT levels, and the stage of liver disease [2].
The course from infection exposure to the development of complications related to CHB infection may span multiple decades. Once diagnosed, treatment may modify the natural course for the better. The American and European guidelines on treatment of chronic hepatitis B recommend treatment with pegylated interferon or the nucleos(t)ide analogs (NA) entecavir or tenofovir [2, 3]. The latter two NAs are preferred over other NAs because of their antiviral potency and a high genetic barrier to resistance. However, treatment options need to be balanced in resource constraint settings. It should be of global concern that resource limitations are especially evident where hepatitis B is endemic or hyperendemic such as in the Far East or in Sub-Saharan Africa [4, 5]. The consequences and costs of treatment strategies may help in contributing to the buildup of health strategies. Based on its GNI (gross national income) per capita, every economy is classified as low income, middle income (subdivided into lower middle and upper middle), or high income, according to the World Bank. The GNI per capita for Turkey is $ 9,500, which classifies Turkey as an upper middle income country. To support national health authorities policy making in long-term chronic hepatitis B treatment, we assessed the impact of treatment in preventing adverse outcomes of CHB infection, and the cost-effectiveness of various treatment strategies. For these goals, Turkey was used and investigated as an example median endemic country.
Methods
Cohort definition
A population cohort of CHB patients was constructed from a recent meta-analysis of age- and region-specific hepatitis B surface antigen (HBsAg) prevalence in Turkey [6]. We projected these age-stratified HBsAg prevalence from the meta-analysis to the total age-specific Turkish population numbers, which was a total of 71.5 million in 2009 [7].
The HBsAg positive cohort was first divided into two groups, active and inactive CHB, based on hepatitis B e-antigen status, HBV DNA level, and serum alanine aminotransferase (ALT) level. The age-specific distributions of these factors were derived from a newly constructed patient database of the gastroenterology departments of the University of Ankara, and a state hospital in Ankara (Turkiye Yuksek Ihtisas Hastanesi) with 1,453 newly diagnosed CHB patients. Both of these hospital departments receive patients from around the country, which supposedly means that the constructed patient data is heterogeneous. In Turkey, almost all CHB cases are detected at the hospital, of which some patients are coincidentally detected during other medical procedures. The differentiation of active and inactive CHB is essential since progression of the disease is different in these two groups. Patients with high HBV DNA levels HBV DNA ≥104 copies/mL and elevated ALT (>2 × ULN) have potentially progressive liver disease and are candidates for HBV antiviral therapy [2], while those with low or undetectable HBV DNA and normal ALT levels usually are inactive HBsAg carriers with a low risk of disease progression. Lastly, we classified the active CHB patients into four categories, namely HBeAg (+) and HBeAg (−) CHB with or without cirrhosis, respectively, using age group-specific proportions from large HBeAg-positive and HBeAg-negative clinical trials [8, 9].
Model and clinical probability estimates
We evaluated the cohort of treatment-naïve active CHB patients for mortality, morbidity, impact of treatment and cost-effectiveness of various treatment strategies for a follow-up time of 20 years, thus the cycle length was 21, and the half cycle correction was applied with the TreeAge Pro 2009 software (TreeAge Software, Inc., MA, USA). The model uses annual probabilities of transition from CHB to virologic response, and of progression to cirrhosis, decompensated liver disease or hepatocellular carcinoma, liver transplantation, and finally death. The natural history and treatment related annual probabilities are obtained mostly from systematic reviews (Tables 1, 2) [10–36]. Other causes of death not related to liver disease are included in the model, as age-specific mortality rates derived from the Turkish statistics institute [7]. The probabilities of receiving a liver transplant were calculated based on personal communications with six major liver transplantation centres distributed throughout Turkey. We received reports that included annual numbers of liver transplants due to HBV related decompensated cirrhosis and HCC. From these figures, we calculated that there are annually around 500 liver transplantations performed in Turkey, of which about 150 are for HBV alone (no co-infections included). Out of these 150 liver transplantations, 120 are due to decompensated cirrhosis, and 30 to HCC. This corresponds to an annual probability of receiving a liver transplant for decompensated cirrhosis of 24 and 6 % for HCC.
Table 1.
Annual transition estimates of the natural history of chronic hepatitis B by initial state
| Initial state | Outcome | Estimate (%)* | Referencesa |
|---|---|---|---|
| Chronic hepatitis B e+ | Resolution | 6.9 (2.0–23) | [10] |
| Cirrhosis | 3.8 (1.6–5.9) | [11] | |
| Hepatocellular carcinoma | 0.3 (0.3–0.6) | [11] | |
| Chronic hepatitis B e− | 1.9 (1.0–3.8) | [11] | |
| Chronic hepatitis B e− | Resolution | 1.6 (0.0–11) | [10] |
| Cirrhosis | 9.7 (2.9–16.3) | [11] | |
| Hepatocellular carcinoma | 0.3 (0.3–0.6) | [11] | |
| Cirrhosis e+ | Decompensated cirrhosis | 3.9 (2.0–7.9) | [12–14] |
| Hepatocellular cancer | 1.8 (0.9–3.8) | [12–14] | |
| HBV related death | 3.1 (3.1–3.8) | [12–14] | |
| Cirrhosis e− | Decompensated cirrhosis | 2.7 (1.4–5.4) | [12–14] |
| Hepatocellular cancer | 2.9 (1.0–5.6) | [12–14] | |
| HBV related death | 3.1 (3.1–3.8) | [12–14] | |
| Decompensated Cirrhosis | Liver transplantation | 23 (15–25) | Personal communicationb |
| HBV related death | 26 (15–62) | [12–14] | |
| Hepatocellular carcinoma | Liver transplantation | 6 (3.0–7.0) | Personal communicationb |
| HBV related death | 35 (20–60) | [10] | |
| Liver transplant | HBV related death | 6.6 (2.0–12) | [10] |
HBV hepatitis B virus
* Ranges are shown in parentheses
aEstimates derived from European cohort studies
bThe probabilities of receiving a liver transplantation for decompensated cirrhosis and hepatocellular carcinoma were calculated on the basis of data from six major transplant centers in Turkey
Table 2.
Treatment-related annual transition estimates
| Initial state | Outcome | Estimate (%) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Lamivudine | Entecavirh | Adefovir salvage | Tenofoviri | Tenofovir salvagej | |||||||
| HBeAg status | + | − | + | − | + | − | + | − | + | − | |
| CHB initial therapya | Sustained virological response | 20 | 10 | 22b | 11b | 12 | 10 | 23 | 11 | 19 | 11 |
| Cirrhosisc | 0.5 | 1.2 | 0.2 | 0.6 | 0.5 | 1.2 | 0.2 | 0.6 | 0.5 | 1.2 | |
| Hepatocellular carcinomaf | 0.2 | 0.2 | 0.2 | 0.2 | 0.2 | 0.2 | 0.2 | 0.2 | 0.2 | 0.2 | |
| CHB long-term therapy | Sustained virological response | 24 | 10 | 27b | 11b | 12 | 10 | 27 | 11 | 19 | 11 |
| Cirrhosisc | 0.5 | 1.2 | 0.2 | 0.6 | 0.5 | 1.2 | 0.2 | 0.6 | 0.5 | 1.2 | |
| Resistance: year 1 | 23d | 23e | 0.1 | 0.1 | 6e | 6e | 0 | 0 | 0 | 0 | |
| Year 2 | 42d | 42d | 0.3 | 0.3 | 21e | 21e | 0 | 0 | 1 | 1 | |
| Year 3 | 53d | 53d | 0.4 | 0.4 | 21e | 21e | 0.4 | 0.4 | 1 | 1 | |
| Year 4 | 70d | 70d | 0.8 | 0.8 | 21e | 21e | 0.8 | 0.8 | 1 | 1 | |
| Year 5 | 74d | 74d | 1 | 1 | 21e | 21e | 1 | 1 | 1 | 1 | |
| Hepatocellular carcinomaf | 0.2 | 0.2 | 0.2 | 0.2 | 0.2 | 0.2 | 0.2 | 0.2 | 0.2 | 0.2 | |
| Resistant CHB long-term therapy | Sustained virological response | 4.5 | 0 | 5b | 0.5b | 4.5 | 0 | 5 | 0.5 | 5 | 0.5 |
| Cirrhosisc | 2.7 | 6.2 | 2.7 | 6.2 | 2.7 | 6.2 | 2.7 | 6.2 | 2.7 | 6.2 | |
| Hepatocellular carcinomaf | 0.4 | 0.4 | 0.4 | 0.4 | 0.4 | 0.4 | 0.4 | 0.4 | 0.4 | 0.4 | |
| Cirrhosis initial therapy | Sustained virological response | 20 | 10 | 22b | 11b | 12 | 10 | 23 | 12 | 19 | 11 |
| Hepatocellular carcinomaf | 0.9 | 1.5 | 0.9 | 1.5 | 0.9 | 1.5 | 0.9 | 1.5 | 0.9 | 1.5 | |
| Cirrhosis long-term therapy | Sustained virological response | 24 | 10 | 27b | 11b | 12 | 10 | 27 | 11 | 19 | 11 |
| Resistance: year 1 | 23d | 23d | 0.1 | 0.1 | 6′′ | 6′′ | 0 | 0 | 0 | 0 | |
| Year 2 | 42d | 42d | 0.3 | 0.3 | 21e | 21e | 0 | 0 | 1 | 1 | |
| Year 3 | 53d | 53d | 0.4 | 0.4 | 21e | 21e | 0.4 | 0.4 | 1 | 1 | |
| Year 4 | 70d | 70d | 0.8 | 0.8 | 21e | 21e | 0.8 | 0.8 | 1 | 1 | |
| Year 5 | 74d | 74d | 1 | 1 | 21e | 21e | 1 | 1 | 1 | 1 | |
| Decompensated cirrhosis | 1.9 | 1.9 | 1.9 | 1.9 | 1.9 | 1.9 | 1.9 | 1.9 | 1.9 | 1.9 | |
| Hepatocellular carcinoma | 1.6 | 1.6 | 1.6 | 1.6 | 1.6 | 1.6 | 1.6 | 1.6 | 1.6 | 1.6 | |
| Death HBV | 2.4 | 2.4 | 2.4 | 2.4 | 2.4 | 2.4 | 2.4 | 2.4 | 2.4 | 2.4 | |
| Resistant cirrhosis long-term therapy | Sustained virological response | 4.5 | 0 | 5b | 0.5b | 4.5 | 0 | 5 | 0.5 | 5 | 0.5 |
| Decompensated Cirrhosis | 7.9 | 7.9 | 7.9 | 7.9 | 7.9 | 7.9 | 7.9 | 7.9 | 7.9 | 7.9 | |
| Hepatocellular carcinoma | 1.8 | 2.9 | 1.8 | 2.9 | 1.8 | 2.9 | 1.8 | 2.9 | 1.8 | 2.9 | |
| Death HBV | 3.1 | 3.1 | 3.1 | 3.1 | 3.1 | 3.1 | 3.1 | 3.1 | 3.1 | 3.1 | |
| Decompensated Cirrhosis | Liver transplantationg | 3.3 | 3.3 | 3.3 | 3.3 | 3.3 | 3.3 | 3.3 | 3.3 | 3.3 | 3.3 |
| Death HBV | 26 | 26 | 26 | 26 | 26 | 26 | 26 | 26 | 26 | 26 | |
| Hepatocellular carcinoma | Liver transplantationg | 1.2 | 1.2 | 1.2 | 1.2 | 1.2 | 1.2 | 1.2 | 1.2 | 1.2 | 1.2 |
| Death HBV | 35 | 35 | 35 | 35 | 35 | 35 | 35 | 35 | 35 | 35 | |
| Liver transplantation | Death HBV | 6.6 | 6.6 | 6.6 | 6.6 | 6.6 | 6.6 | 6.6 | 6.6 | 6.6 | 6.6 |
Estimates from Kanwal et al. [10, 15]
aInitial therapy is 12 months (48 weeks) of therapy
bEstimates from recent clinical trials: Chang et al. [16], Lai et al. [17] and Colonno et al. [18]
cEstimates calculated by the author, based on the assumption that the natural progression rates of chronic hepatitis B are reduced by antiviral therapy. Estimates derived from natural history estimate similar to Kanwal’s assumption of no progression of disease in HBeAg seroconversion, we assume no progression of disease in case HBV DNA is undetectable by PCR. In the papers from Chang and Lai full suppression of HBV DNA was observed in 80 % with a high resistance profile drug, and 90 % with a low resistance profile drug. We took these percentages for our calculations. Refs. [16, 17]
dEstimates for Lamivudine resistance from Lai et al. [19] and Moskovitz et al. [20]
eAdefovir salvage resistance estimates from Lee et al. [21], Chen et al. [22] and Yeon et al. [23]
fEstimates based on reduction of progression rates by nucleoside analogue therapy of 50 % Ref. [24]
gThe probabilities of receiving a liver transplantation for decompensated cirrhosis and hepatocellular carcinoma were calculated on the basis of data from six major transplant centres in Turkey
hEstimates for entecavir resistance from Colonno et al. [18, 25] and Tenney et al. [26]
iTenofovir monotherapy estimates Ref. [27]
jTenofovir salvage scenario estimates from van Bommel et al. [28], Sarin et al. [29], van Bommel et al. [30] and Reijnders et al. [31]
Scenario analysis
The following treatment options used by clinicians in Turkey were analyzed:
Natural History (no antiviral treatment) scenario: In this scenario, which is the base case scenario, active CHB patients progress according to the natural history, following annual rates of progression derived from systematic reviews (Table 1). Since the disease progression rates differ among European and Asian cohort studies [11], we only implemented in the model the annual progression rates derived from European cohort studies. We assumed that patients were followed clinically but did not receive antiviral therapy for CHB. Patients followed the natural history according to their HBeAg and disease status (with or without cirrhosis). Resolution was defined as seroconversion to anti-HBe in HBeAg positive patients, and as persistent HBV DNA suppression and ALT normalization in HBeAg negative patients. We assumed that all patients received regular ongoing care once complications occur.
Lamivudine monotherapy scenario: In this scenario, patients received 100 mg orally once daily with the first licensed antiviral HBV drug that is associated with a high incidence of resistance [24]. Such monotherapy is still being practiced in many countries with limited resources [5, 37]. We defined sustained virological response (SVR) in HBeAg positive patients as HBe-antigen loss and development of antibodies against HBeAg (anti-HBe).
Entecavir monotherapy scenario: Patients in this strategy received 0.5 mg entacavir once daily [38, 39]. The treatment related probability estimates are shown in Table 2.
Tenofovir monotherapy scenario: In this scenario patients received 300 mg of tenofovir for a continuum of 20 years. The annual probability of resistance in this scenario was 0 % for the first and second years of treatment.
Adefovir salvage scenario: In this scenario, patients initially receive lamivudine. Once resistance occurs, patients are salvaged add-on by add-on adefovir. Patients without resistance continued to receive lamivudine.
Tenofovir salvage scenario: In this more up-to-date scenario, patients who have developed resistance during lamivudine therapy are switched to treatment with tenofovir [31].
Pegylated Interferon, followed by tenofovir scenario: In this scenario patients receive 180 mcg/mL of pegylated interferon once a week subcutaneously, for 48 weeks. If the patients do not respond or relapse, they start tenofovir in the following year. The annual transition rates for SVR after 72 weeks of Peg-IFN was 30 % for HBeAg-positive and 20 % for HBeAg-negative patients [32–34, 40]. The withdrawal rate was 2 and 5 % for HBeAg-positive and negative patients, respectively [35].
Roadmap concept scenario: In this scenario we applied the ‘roadmap concept’ [41] to the sub-group of CHB non-cirrhotic HBeAg-negative cases treated with lamivudine, due to its low price, which continues to be widely used in HBV endemic areas. Patients with HBV DNA levels <107 copies/mL start therapy with lamivudine; after 24 weeks virologic response on treatment is assessed. If HBV DNA is undetectable (50 UI/mL, 300 copies/mL), patients continue their treatment with lamivudine until resistance or virologic breakthrough occurs, after which patients are switched to tenofovir. However, if HBV DNA is above 300 copies/mL at 24 weeks, lamivudine is switched to tenefovir monotherapy already at week 24. 71 % of patients are expected to become HBV DNA negative at week 24 of treatment [42]. Annual resistance rate in these patients on lamivudine treatment is 2 % [43, 44]. Annual rate of HBV DNA relapse is 8.2 % (28 % at 4 years) [44].
Model assumptions
An assumption was that HBeAg-positive non-cirrhotic patients stop treatment after receiving one year consolidation treatment after HBeAg seroconversion and achieving undetectable HBV DNA levels [2], while HBeAg-negative patients continue treatment [38] for the follow-up period of 20 years. Also, our model assumes that the resistance for entecavir and tenofovir scenarios stays low as recent studies report. After the third year of treatment tenofovir resistance is assumed to be the same as entecavir. We took different time points to assess the outcomes for pegylated interferon and nucleos(t)ide analogues. For the Peg-IFN scenario we assumed that the non-responders continued with long-term tenofovir treatment both in HBeAg-positive and negative patients. For the road map concept the annual resistance of 2 % estimate was derived from the GLOBE telbivudine versus lamivudine trial [43].
Cost and utility estimates
Medical costs are obtained from a retrospective analysis of the medical records of a sample of 542 patients (3,000 hospital admissions), where a random sample of patients was selected from inactive carriers, CHB active, cirrhosis, HCC and liver transplantation cases. An average annual medical treatment cost (excluding antiviral treatment) per patient in each health state was calculated (unpublished work). Data extracted for outpatient visits included information of visits, diagnosis, type of examination, signs and symptoms, laboratory tests, and procedures. Outpatients costs were mainly costs of laboratory tests, examination and consult. Information for inpatients included the length of stay, bed costs, surgical procedures, radiation treatment and chemotherapy. Annual cost was calculated as: cost per visit × visit per year + costs per admission × admission per year. The costs of antiviral drugs are obtained from the Turkish Ministry of Health [45]. A wide range of age-specific health state utilities are obtained from a multinational study on chronic hepatitis B [46]. Table 3 contains the specific cost and utility estimates. All costs and utilities were discounted at a rate of 3 % per year [47].
Table 3.
Annual costs and health state utilities for chronic hepatitis B
| Parameter | Base-case estimate TL (€) | (range) | References |
|---|---|---|---|
| Drug costs (year 2010 values) | |||
| Lamivudine treatment (100 mg) | 1,176 (585) | 884–1,470 (439–731) | [45] |
| Adefovir salvage treatment (10 mg) | 12,012 (5,976) | 9,009–15,015 (4,482–7,470) | [45] |
| Entecavir treatment (0.5 mg) | 11,292 (5,618) | 8,469–14,115 (4,214–7,022) | [45] |
| Tenofovir (300 mg) | 8,028 (3,994) | 6,021–10,035 (2,996–4,992) | [45] |
| Peg-INF alfa 2a (INJVL 180MCG/ML) | 19,344 (9,624) | 14,508–24,180 (7,218–12,030) | [45] |
| Medical management costs | Personal communicationa | ||
| Monitoring of CHB | 720 (358) | 540–900 (269–627) | |
| Compensated Cirrhosis | 1,204 (602) | 903–1,505 (452–752) | |
| Decompensated Cirrhosis | 5,364 (2,668) | 4,023–6,705 (2,001–3,335) | |
| Hepatocellular carcinoma | 14,300 (7,114) | 10,725–17,875 (5,336–8,892) | |
| Liver transplantation | 174,050 (86,592) | 130,538–217,562 (64,944–108,240) | |
| Health state utilitiesb | |||
| Durable response to treatment | 1.00 | (0.95–1.00) | [46] |
| Chronic HBV | 0.68 | (0.66–0.70) | [46] |
| Compensated cirrhosis | 0.69 | (0.66–0.71) | [46] |
| Decompensated cirrhosis | 0.35 | (0.32–0.37) | [46] |
| Hepatocellulr carcinoma | 0.38 | (0.36–0.41) | [46] |
| Liver transplantation | 0.67 | (0.64–0.69) | [46] |
CHB chronic hepatitis B, HBV hepatitis B virus
aObtained from a retrospective analysis of medical records of a sample of 3,000 hospital admissions unpublished work
bSee Levy et al. (Ref. [46]) for the age-specific utilities
Outcomes
By applying the Markov cohort analysis, the cumulative mortality, and the cumulative probability of developing cirrhosis, decompensated cirrhosis, HCC, and getting a liver transplant were quantified for a 20-year time period. We measured costs (2010 Euro and Turkish Lira), quality adjusted life years (QALYs), and the incremental cost-effectiveness ratio (ICER), to determine the additional cost to obtain one QALY. The guidelines of economic submission to the BMJ was used for this cost-effectiveness analysis [48].
Sensitivity analysis
To study the effect of uncertainty of the robustness of our results, we performed a sensitivity analysis on the low and high ranges of the transition estimates in the natural history scenario (Table 1). First, a so called best case scenario was assessed by applying the high range of achieving spontaneous virological response, and the low ranges for the estimates of disease progression. Second, a worst case scenario was assessed by applying the low rates for spontaneous virological response, and the high ranges for the disease progression estimates.
We assume that after seroconversion occurs, patients are allowed a 6 month therapy, and NAs are discontinued. A recent publication suggests continuation of long-term nucleos(t)ide analogue treatment, irrespective of the occurrence of HBeAg seroconversion in HBeAg-positive patients. Following this recent finding, an alternative scenario was assessed where treatment was continued in HBeAg-positive patients.
In addition, we performed a Monte Carlo simulation assuming that all variables followed a triangular distribution, due to its continues distribution, with base case, low and high range of values. We simulated 10,000 trials and plotted the results on cost-effectiveness acceptability curve stratified by cost-effectiveness thresholds to determine which treatment to use under different budgetary restraints.
Results
Cohort
Table 4 shows the total population of Turkey in 2009 with the age-specific prevalence of HBsAg. Around 3.2 million people (4.6 % of the total population) were estimated to be HBsAg carriers, with 22.6 % of them having HBeAg-positive CHB and 77.4 % having HBeAg-negative CHB. The total number of patients with active CHB was about 828,000 or 25 % of the total HBsAg-positive cohort, of which 57 % had HBeAg-positive and the rest HBeAg-negative CHB. The proportion that had cirrhosis in the active CHB cohort was 13 %.
Table 4.
Age group specific distribution of chronic hepatitis B in Turkey by HBeAg and stage of liver disease
| Age group | Active CHB | Cirrhosis | Chronic hepatitis (no cirrhosis) |
|||||||
|---|---|---|---|---|---|---|---|---|---|---|
| (years) | Population | HBsAg+ (%) | HBeAg+ | HBeAg− | HBeAg+ | HBeAg− | HBeAg+ (%) | HBeAg− (%) | HBeAg+ | HBeAg− |
| 0–14 | 18,788,587 | 533,596 (2.84) | 283,828 | 249,768 | 90,621 | 47,586 | 1,818 (2) | 2,379 (5) | 88,808 | 45,207 |
| 15–24 | 12,441,662 | 490,201 (3.94) | 176,473 | 313,729 | 91,504 | 45,804 | 1,830 (2) | 2,290 (5) | 89,674 | 43,514 |
| 25–34 | 12,328,944 | 784,121 (6.36) | 159,961 | 624,160 | 113,892 | 132,322 | 6,834 (6) | 9,263 (7) | 107,058 | 123,059 |
| 35–44 | 10,070,734 | 624,386 (6.20) | 62,439 | 561,947 | 35,222 | 96,610 | 2,466 (7) | 14,491 (15) | 32,756 | 82,118 |
| 45–54 | 7,927,348 | 437,590 (5.52) | 22,655 | 414,935 | 11,923 | 74,353 | 2,981 (25) | 20,819 (28) | 8,943 | 53,534 |
| 55–64 | 5,066,402 | 184,924 (3.65) | 12,753 | 172,170 | 5,070 | 41,595 | 1,673 (33) | 21,214 (51) | 3,397 | 20,382 |
| 65+ | 4,893,423 | 197,205 (4.03) | 18,260 | 178,945 | 4,565 | 37,280 | 0 | 20,877 (56) | 4,565 | 16,403 |
| Total | 71,517,100 | 3,252,022 (4.57) | 736,367 | 2,515,655 | 352,797 | 475,550 | 17,595 (9) | 91,333 (19) | 335,202 | 384,217 |
CHB chronic hepatitis B, HBeAg hepatitis B e antigen, HBsAg hepatitis B surface antigen
Mortality and morbidity in the active CHB cohort
The estimated age-specific CHB burden in a 20-year follow up is shown in Table 5 for the natural history scenario. If the cohort of 828,347 individuals remains untreated, it is estimated that 256,788 (31 %) will die due to liver related complications. Within a 20-year period, 11 % will have developed decompensated cirrhosis, 12 % HCC and 6 % will need liver transplantation. At the entry into the cohort in the year 2009, 108,928 (13 %) cases were estimated to be already in the cirrhotic stage. By the year 2029, another 247,261 (30 %) cases will have developed cirrhosis if left untreated, and this will have led to a cumulative number of 356,189 (43 %) patients with cirrhosis in the eligible cohort.
Table 5.
Age-specific clinical outcome of active chronic hepatitis B by HBeAg status in the natural history scenario
| HBeAg status | n | Outcome | ||||
|---|---|---|---|---|---|---|
| Age-group (years) | Cirrhosis (%) | Decompensated Cirrhosis (%) | HCC (%) | Liver transplant (%) | Death (%) | |
| HBeAg+ | ||||||
| <15 | 90,621 | 819 (1) | 863 (1) | 1,234 (1) | 503 (0,5) | 2,574 (3) |
| 15–24 | 91,504 | 833 (1) | 877 (1) | 1,257 (1) | 512 (0,5) | 2,617 (3) |
| 25–34 | 113,892 | 35,401 (31) | 12,082 (11) | 8,461 (7) | 5,776 (5) | 27,276 (24) |
| 35–44 | 35,222 | 10,966 (31) | 3,694 (11) | 2,561 (7) | 1,769 (5) | 8,316 (24) |
| 45–54 | 11,923 | 3,783 (32) | 1,741 (15) | 1,050 (9) | 825 (7) | 3,842 (32) |
| 55–64 | 5,070 | 1,630 (32) | 779 (16) | 452 (9) | 359 (7) | 1,689 (33) |
| 65+ | 4,565 | 1,574 (34) | 241 (5) | 206 (5) | 109 (2) | 526 (12) |
| All HBeAg+ | 352,797 | 55,006 (16) | 20,277 (6) | 15,221 (4) | 9,853 (3) | 46,840 (13) |
| HBeAg− | ||||||
| <15 | 47,586 | 424 (1) | 680 (1) | 1,153 (2) | 412 (1) | 2,465 (5) |
| 15–24 | 45,804 | 406 (1) | 657 (1) | 1,110 (2) | 400 (1) | 2,389 (5) |
| 25–34 | 132,322 | 99,242 (75) | 22,392 (17) | 26,464 (20) | 11,770 (9) | 67,484 (51) |
| 35–44 | 96,610 | 73,924 (76) | 16,424 (17) | 19,322 (20) | 8,695 (9) | 50,237 (52) |
| 45–54 | 74,353 | 54,278 (73) | 12,640 (17) | 15,614 (21) | 6,692 (9) | 39,407 (53) |
| 55–64 | 41,595 | 28,285 (68) | 7,071 (17) | 8,319 (20) | 3,744 (9) | 22,045 (53) |
| 65+ | 37,280 | 25,723 (69) | 4,846 (13) | 5,592 (15) | 2,237 (6) | 13,794 (37) |
| All HBeAg− | 475,550 | 323,374 (68) | 76,088 (16) | 90,355 (19) | 38,044 (8) | 223,509 (47) |
| Total | 828,347 | 356,189 (43) | 91,118 (11) | 99,402 (12) | 49,701 (6) | 256,788 (31) |
Impact of antiviral treatment on burden of disease
Treating the cohort with lamivudine monotherapy will decrease the mortality from 256,787 (31 %) to 124,253 (15 %) of cases, and when salvage therapy without delay is applied once patients become resistant to lamivudine, mortality will further decrease to 49,700 (6 %) cases. With the Peg-IFN (followed by tenofovir) strategy mortality will be reduced to 82,834 (10 %) cases. Treating the same patients with entecavir or tenefovir monotherapy will decrease the mortality to 41,417 liver related deaths (5 %).
Cost-effectiveness
A plot of the outcomes of the various strategies on the cost-effectiveness plane according to HBeAg and disease status is shown in Fig. 1. The total costs, QALYs gained, incremental QALYs, incremental costs and ICERs for each scenario are presented in Table 6.
Fig. 1.
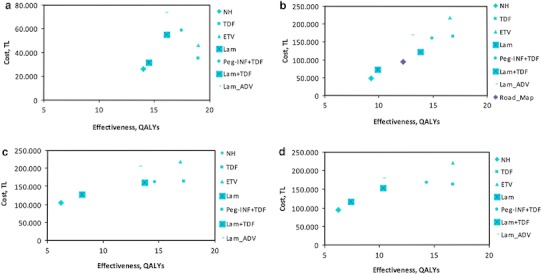
Results of cost-effectiveness analysis stratified by hepatitis B e antigen (HBeAg) and stage of liver disease: a HBeAg-positive (non-cirrhosis) b HBeAg-negative (non-cirrhosis) c HBeAg-positive (cirrhosis) d HBeAg-negative (cirrhosis). Results plotted on a cost-effectiveness plane. The x-axis represents the gain in QALYs with each strategy, and the y-axis the total healthcare costs (year 2010 values). NH natural history, Lam lamivudine, Lam + ADV adefovir salvage therapy, Peg_IFN + TDF pegylated interferon followed by tenofovir, ETV entecavir, TDF tenofovir
Table 6.
Base case results of various scenarios: costs, quality adjusted life years (QALYs) gained, incremental QALYs, incremental costs and incremental cost-effectiveness ratios (ICERs)
| Treatment | NH* | Lam | Lam + ADV | Lam + TDF | ||||
|---|---|---|---|---|---|---|---|---|
| HBeAg status | + | − | + | − | + | − | + | − |
| CHB (no cirrhosis) | ||||||||
| Cumulative costs (×1,000 TL (€)) | 25.7 (12.8) | 48.2 (23.9) | 31.6 (15.7) | 72.6 (36.1) | 73.4 (36.5) | 168.5 (83.8) | 54.7 (27.2) | 122.5 (60.9) |
| Cumulative QALYs | 14.0 | 9.3 | 14.5 | 9.9 | 17.0 | 13.0 | 17.5 | 13.8 |
| Incremental costs (×1,000 TL (€))a | – | – | 5.8 (2.9) | 24.4 (12.1) | 41.9 (20.8) | 120.3 (59.9) | 23.2 (11.5) | 74.4 (37.0) |
| Incremental QALYsb | – | – | 0.5 | 0.6 | 3.0 | 3.7 | 3.5 | 4.5 |
| ICER (×1,000 TL (€)/QALY) | – | – | 11.2 (5.5) | 38.3 (19.0) | 13.9 (6.9) | 32.1 (16.0) | 6.6 (3.2) | 16.3 (8.1) |
| Cirrhosis | ||||||||
| Cumulative costs (×1,000 TL (€)) | 104.9 (52.2) | 93.9 (46.7) | 128.1 (63.7) | 117.2 (20.1) | 205.5 (102.2) | 180.0 (89.6) | 160.6 (79.9) | 154.6 (76.9) |
| Cumulative QALYs | 6.2 | 6.2 | 8.1 | 7.4 | 13.2 | 12.9 | 13.7 | 13.5 |
| Incremental costs (×1,000 TL (€))a | – | – | 23.3 (11.6) | 23.2 (11.6) | 100.7 (50.0) | 86.1 (42.8) | 55.8 (27.5) | 60.6 (30.1) |
| Incremental QALYsb | – | – | 1.9 | 1.2 | 7 | 6.7 | 7.5 | 7.3 |
| ICER (×1,000 TL (€)/QALY) | – | – | 12.5 (6.2) | 20.1 (10.0) | 14.5 (7.2) | 12.9 (6.4) | 7.5 (3.7) | 8.3 (4.1) |
| Treatment | Peg INF + TDF | ETV | TDF | Roadmap | |||
|---|---|---|---|---|---|---|---|
| HBeAg status | + | − | + | − | + | − | − |
| CHB (no cirrhosis) | |||||||
| Cumulative costs (×1,000 TL (€)) | 58.7 (29.2) | 161.0 (80.1) | 46.0 (22.9) | 218.0 (108.5) | 34.8 (17.3) | 165.9 (82.5) | 94.8 (47.1) |
| Cumulative QALYs | 17.5 | 14.9 | 18.8 | 16.6 | 19.0 | 16.8 | 12.2 |
| Incremental costs (×1,000 TL (€))a | 27.1 (13.5) | 112.9 (56.2) | 14.4 (7.2) | 169.9 (84.5) | 3.2 (1.6) | 117.7 (58.5) | 46.6 (23.2) |
| Incremental QALYsb | 3.5 | 5.6 | 4.8 | 7.3 | 5.0 | 7.6 | 2.9 |
| ICER (×1,000 TL (€)/QALY) | 7.8 (3.9) | 20.0 (9.9) | 3.0 (1.5) | 23.2 (11.6) | 0.6 (0.3) | 15.6 (7.8) | 15.6 (7.9) |
| Cirrhosis | |||||||
| Cumulative costs (×1,000 TL (€)) | 162.9 (81.0) | 168.2 (83.7) | 218.5 (108.7) | 220.8 (109.8) | 163.5 (81.3) | 163.1 (81.2) | – |
| Cumulative QALYs | 14.6 | 14.3 | 16.9 | 16.5 | 17.2 | 16.7 | – |
| Incremental costs (×1,000 TL (€))a | 58.1 (28.9) | 74.2 (36.9) | 113.6 (56.5) | 126.8 (63.1) | 58.6 (29.2) | 69.1 (34.4) | – |
| Incremental QALYsb | 8.4 | 8.0 | 10.7 | 10.3 | 11.0 | 10.5 | – |
| ICER (×1,000 TL (€)/QALY) | 6.9 (3.4) | 9.2 (4.6) | 10.7 (5.3) | 12.3 (6.1) | 5.3 (2.6) | 6.6 (3.3) | – |
NH natural history, Lam lamivudine, Lam + ADV adefovir salvage therapy, Peg_IFN + TDF pegylated interferon followed by tenofovir, ETV entecavir, TDF tenofovir
* “NH (no treatment)” was the baseline strategy compared with other treatment strategies
aDifference in costs over NH
bDifference in healthy years over NH
Chronic hepatitis (non-cirrhosis)
The increasing health gain achieved over a period of 20 years for both HBeAg-positive and -negative patients has been assessed for lamivudine, the roadmap concept (for HBeAg-negative only), adefovir salvage, tenofovir salvage, pegylated interferon (followed by tenofovir), entecavir and tenofovir therapy strategies.
The natural history (no-treatment) strategy resulted in 14 and 9.3 QALYs and total discounted 20-year CHB related healthcare costs of 25,781 TL (€12,826) and 48,198 TL (€23,979) for the HBeAg-positive and negative cohort, respectively.
Both tenofovir and entecavir had equal incremental QALYs; however, entecavir compared to tenofovir, in a 20 year follow up period was 11,252 TL (€5,598) and 52,159 TL (€25,949) more expensive in HBeAg-positive and negative patients, respectively. The incremental cost-effectiveness ratio (ICER) of tenofovir versus no treatment was 638 TL (€318) and 15,573 TL (€7,747) for HBeAg-positive and negative patients, respectively.
CHB (cirrhosis)
The no-treatment strategy resulted in 6.2 QALYs and total healthcare costs of 104,859 TL (€52,168) and 93,954 TL (€46,743) for the cirrhotic HBeAg-positive and negative cohort, respectively. The lowest ICER was achieved with the tenofovir scenario versus no treatment which was 5,328 TL (€2,650) and 6,609 TL (€3,288) in the HBeAg-positive and negative cohort, respectively.
Sensitivity analysis
The sensitivity analysis for the natural history scenario shows that, in comparison with the base case, in which the mortality of the active CHB cohort is 31 %, the mortality ranges from 17 % in the best case scenario to 42 % in the worst case scenario. When assessed by subgroups, in the worst case scenario, mortality ranges from 4 to 28 % for HBeAg-positive chronic hepatitis, from 8 to 35 % for HBeAg-negative chronic hepatitis, and from 62 to 91 % for cirrhosis independent of HBeAg status.
The ICER outcomes analysed when antiviral therapy were continued irrespective of HBeAg-seroconversion, varied according to the therapy chosen. Tenofovir and entecavir monotherapy had an ICER of 22,100 TL (€11,000) and 36,800 TL (€18,000), respectively. The ICER for lamivudine monotherapy, lamivudine/adefovir salvage and lamivudine/tenofovir salvage were, 56,200 TL (€27,900), 51,200 TL (€25,400) and 26,200 TL (€13,000), respectively. Pegylated interferon (followed by tenofovir) had an ICER of 27,600 TL (€13,700).
The World Health Organization defines the threshold value for intervention cost-effectiveness as three times the gross national income (GNI) of a country. The threshold value for Turkey is 47,280 TL (€20,124) [49]. The probabilistic sensitivity analysis indicated that the no-treatment strategy was preferred at cost-effectiveness thresholds less than approximately 30,000 TL (€14,925) per QALY, and tenofovir had the highest probability of being optimal above this threshold (Fig. 2) for the HBeAg-positive (non-cirrhosis) patients. For the HBeAg-negative (non-cirrhosis) patients, tenofovir had the highest probability of being optimal above 30,000 TL (€14,925) per QALY.
Fig. 2.
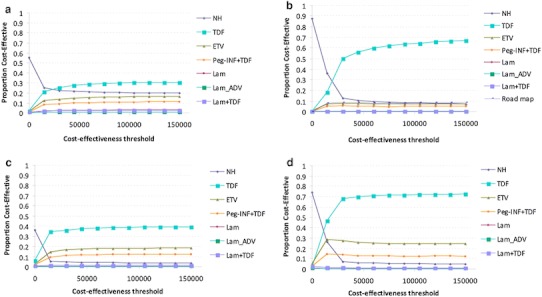
Cost-effectiveness acceptability curves showing the probabilities of net benefits achieved by each strategy for different willingness to pay thresholds (the maximum amount a person is willing to pay for a good) in HBeAg-positive (non-cirrhosis) (a), HBeAg-negative (non-cirrhosis) (b), HBeAg-positive (cirrhosis) (c), and HBeAg-negative (cirrhosis) (d). The vertical axes represent the probability of cost-effectiveness. The horizontal axes represent willingness-to-pay threshold to gain one additional quality adjusted life year (QALY). NH natural history, Lam lamivudine, Lam + ADV adefovir salvage therapy, Peg_IFN + TDF pegylated interferon followed by tenofovir, ETV entecavir, TDF tenofovir
For the HBeAg-positive cirrhotic patients, at a 15,000 TL (€7,462) per QALY threshold, tenofovir had the greatest net health benefit in 34 % of the simulations, and pegylated Interferon (followed by tenofovir) in 10 % of the simulations. In HBeAg-negative cirrhotic patients, tenofovir had a net health benefit of 46 % and pegylated interferon (followed by tenofovir) 14 % at a 15,000 TL (€7,462) per QALY threshold.
Program costs for treating eligible patients
In addition to the cost and QALY gained per patient, we calculated the total program costs if the active CHB patients are identified and treated with the most cost-effective strategy. Tenofovir monotherapy had the lowest ICER for all sub-groups (HBeAg-positive; 638 TL (€318), HBeAg-negative; 15,573 TL (€7,747), HBeAg-positive cirrhosis; 5,328 TL, (€2,650), HBeAg-negative cirrhosis; 6,609 TL, (€3,288)), with ICERs far below the 36,212 TL (€18,016) threshold value. If the total 828,347 active CHB patients (Table 5) are treated, it will cost about 4.6 billion TL (€2.3 billion) annually, if not treated the total costs are tripled due to progression to liver failure and the high costs of medical treatment (hospitalization) and the need for liver transplantation.
Discussion
In a country where the estimated number of HBsAg-positive cases is more than 3.2 million, the total amount of treatment eligible patients, which was quantified through population data and the large patient database constructed for this study, is 828,000, and of these, around 108,000 are patients with liver cirrhosis. If these eligible patients are not identified and treated, about 12,800 deaths are expected to occur each year due to liver related complications, leading to a cumulative number of 256,788 (31 %) in 20 years. The number of liver transplant patients in Turkey is 400–500 per year and this treatment is covered by the health insurance [50]. If we would modestly assume that 50 % of liver transplantations are due to HBV, there will be a total of about 4,000 liver transplantations that will take place in 20 years, while the demand will be around 49,000, according to our estimates. On top of all the life years lost, and more severe treatment options such as liver transplantation are needed, the 20-year cumulative medical management cost of an untreated active HBeAg-positive and HBeAg-negative CHB (no-cirrhosis) patient will be 25,781 TL (€12,800), and 48,198 TL (€23,900), respectively.
If the estimated active CHB cohort is identified and treated with the most cost-effective drug, liver related mortality and morbidity can be reduced by almost 80 %. Comparing treatment scenarios to the no antiviral treatment scenario in all the sub-cohorts, the tenofovir strategy was the most cost-effective. The ICER for HBeAg-positive and negative CHB (non-cirrhosis), and HBeAg-positive and negative cirrhosis was 638 TL (€306), 15,573 TL (€7,800), 5,300 TL (€2,600), and 6,609 TL (€3,300), respectively. Both entecavir and tenofovir, compared to the do nothing scenario, had the same amount of health gain. A recent systematic review and Bayesian meta-analysis concludes that in the first year of treatment for CHB, tenofovir and entecavir are the most potent oral antiviral agents for HBeAg-positive patients, while for HBeAg-negative patients tenofovir is most effective [51]. According to net sold medication counts per year in Turkey, it was calculated that no more than 10 % of active CHB patients receive antiviral treatment [52], indicating a massive shortcoming in providing eligible patients with life prolonged and even life saving treatments. At individual level the association of disease progression with increased cost of disease management suggests that measures to prevent or delay progression of CHB related liver diseases will be economically beneficial. At population level, however, the impact of therapy on the overall number of people with chronic infection will remain limited as long as the majority of infected patients will not receive treatment due to lack of recourse for optimal treatment.
The future public health burden of chronic hepatitis B could potentially be reduced by antiviral treatment [53]. The recommendations by the Turkish Association for the Study of the Liver (TASL) [52] to treat eligible patients are in line with the European Association for the Study of the Liver [2] criteria, except that liver biopsy evidence is always required to start treatment in patients with no established cirrhosis. Almost all patients are reimbursed for treatment of viral hepatitis through the national insurance system in Turkey. A new modification issued in 2009 by the department within Turkish Health Authorities responsible for reimbursement decisions, states that lamivudine should be the first line therapy in all patients with viral load lower than 107 copies/mL. This is largely due to the low costs of lamivudine and to the recent data about on-treatment monitoring approach, using serum HBV DNA level as a predictor for efficacy and drug resistance. We assessed whether this scenario (roadmap concept) was cost-effective in an HBeAg-negative non-cirrhotic patients group, since sufficient data were available for this sub-group. The ICERs of both scenarios, roadmap concept [15,829 TL (€7,875)] and tenofovir monotherapy [15,573 TL (€7,747)], were equal. Although eight healthy life years were gained by tenofovir monotherapy while this was only three healthy life years gained for the roadmap concept scenario.
According to our outcomes, the roadmap concept could be an alternative strategy to consider for a country with a large HBeAg-negative disease, where tenofovir is not available. This scenario could also be suggested in resource poor settings, since the cumulative costs to treat are less compared to tenofovir monotherapy. Various studies have examined the cost-effectiveness of antiviral therapy for CHB and have concluded that treatment is cost-effective versus no treatment [10, 15, 54–56]. Kanwal et al. [10] found that lamivudine monotherapy strategy was more expensive and less effective than treatment with interferon or salvaged by adefovir. According to our analysis, lamivudine monotherapy was less effective as well, but was not more expensive compared to other treatment strategies. This can be explained by the fact that more than 5 years have elapsed between both studies during which the price of lamivudine has decreased. Buti et al. [57] concludes that first-line treatment with tenofovir is cost-effective for both HBeAg-positive and negative patients, in comparison to other antivirals. They also conclude that tenofovir was more effective than entecavir, which is in contrast to our results for which the efficacy equality was equal for both drugs.
A country with similar patient characteristics and health care system may benefit from our scenario analysis and outcomes related to the burden of disease. Considering the economic affordability in different countries, the cost-effectiveness thresholds may be different. It may be that in a country where the threshold is high, a more expensive but effective drug is cost-effective, while this might not be the case for this same drug in a country with a lower cost-effectiveness threshold. A review study by Barbieri et al. [58] on the generalizability of cost-effectiveness studies concludes that the differences in cost-effectiveness results between countries are not systematic, which makes inferences from one country to another difficult.
A limitation of our study is that we used simplified assumptions (e.g., we did not consider coinfection with other viruses or toxins such as alcohol that will accelerate progression), and we assumed the cohort to be static, so there were no new cases added to the cohort. Also, the assumption that the development of resistance both with entecavir and tenofovir for the coming 20 years will stay at 0–1 % per year may underestimate what will happen as longer term data are collected. We took a rather conservative approach by only including high HBV DNA and ALT >2 × ULN. If, like in the guidelines, we had taken elevated ALT levels but starting at 1 × ULN, the number of eligible patients would have increased. Another factor that surely plays an important role in the estimation of eligible patients is the inclusion of data from tertiary centres. In Turkey, data on viral hepatitis are collected at the provincial health directorate, but only for acute (incident) cases. Thus, the data on CHB patients is derived from clinical settings, of which not all patients coming to the hospital have active disease. Some patients are detected during the diagnostic process for other diseases and referred to the hepatology department. We conclude that the cohort data from Turkey are, therefore, likely to be biased towards more active CHB cases, which could mean that the number of eligible patients might be an overestimation. One way to account for this bias would be to implement new information systems and registries to facilitate the notification, counseling, and medical management of persons with CHB infections in countries with intermediate or high endemicity. Any attempt to predict the future is likely to be biased. Therefore, our projections and estimates regarding future treatment rates and liver-related deaths are only intended to provide a crude overview of the public health impact of antiviral therapy.
Identification of chronic hepatitis B infected individuals is essential to ensure that infected persons receive necessary care to prevent or delay onset of significant liver disease and services to prevent transmission to others. Achieving identification could be done by monitoring inactive cases annually, as is recommended in the guidelines. Antenatal screening should be routinely performs, and new information systems and registries should be implemented to facilitate the notification, counselling, and medical management of persons with chronic HBV infection in countries with intermediate and high endemicity. Given the substantial mortality and morbidity attributable to HBV related chronic liver diseases, the control of progression to cirrhosis, decompensated cirrhosis and liver cancer will continue to be an important public health priority. Third generation drugs, such as entecavir and tenofovir, with high effectiveness and low resistance profiles, should be made more affordable to help people with active chronic hepatitis B lead healthier lives.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Acknowledgments
The authors would like to thank the following people from various liver transplantation centres for their contribution of information: Dr. Dinc Dincer of Antalya Medical Faculty, Dr. Murat Danyangac of Istanbul Florence Nightingale hospital, Meral Kose of Ibn-i Sina hospital, Ankara, Dr. Sebahattin Kaymakoglu of Istanbul Medical Faculty, Dr. Zeki Karasu of Ege University, Izmir, Dr. Yilmaz Cakaloglu of Istanbul Memorial hospital.
Conflict of interest
This study was supported by the European Association for the study of the liver (EASL). Dame Sheila Sherlock short-term fellowship awarded to Mehlika Toy.
Open Access
This article is distributed under the terms of the Creative Commons Attribution License which permits any use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
References
- 1.Lavanchy D. Hepatitis B virus epidemiology, disease burden, treatment, and current and emerging prevention and control measures. J. Viral Hepat. 2004;11(2):97–107. doi: 10.1046/j.1365-2893.2003.00487.x. [DOI] [PubMed] [Google Scholar]
- 2.European Association For The Study of The Liver EASL clinical practice guidelines: management of chronic hepatitis B. J. Hepatol. 2009;50(2):227–242. doi: 10.1016/j.jhep.2008.10.001. [DOI] [PubMed] [Google Scholar]
- 3.Lok AS, McMahon BJ. Chronic hepatitis B: update 2009. Hepatology. 2009;50:661–662. doi: 10.1002/hep.23190. [DOI] [PubMed] [Google Scholar]
- 4.Ferenci P, Fried M, Labrecque D, Bruix J, Sherman M, Omata M, Heathcote J, Piratsivuth T, Kew M, Otegbayo JA, Zheng SS, Sarin S, Hamid SS, Modawi SB, Fleig W, Fedail S, Thomson A, Khan A, Malfertheiner P, Lau G, Carillo FJ, Krabshuis J, Le Mair A. World Gastroenterology O: Hepatocellular carcinoma (HCC): a global perspective. J. Clin. Gastroenterol. 2010;44(4):239–245. doi: 10.1097/MCG.0b013e3181d46ef2. [DOI] [PubMed] [Google Scholar]
- 5.Yurdaydin, C., Akarca, U.: Treatment of chronic hepatitis B with telbuvidine: wise hepatologists needed in hepatitis B endemic countries where treatment options are limited. Liver Int. 31(5), 589–591 (2011) [DOI] [PubMed]
- 6.Toy, M., Onder, F.O., Wormann, T., Bozdayi, M., Schalm, S.W., Borsboom, G.J., Idilman, R., Richardus, J.H., Yurdaydin, C.: Age- and region-specific hepatitis B prevalence in Turkey estimated using generalized linear mixed models: a systematic review. BioMed Central Infect. Dis. 11, 337 (2011) [DOI] [PMC free article] [PubMed]
- 7.Turkish Statistics Institute: In., p. http://www.tuik.gov.tr/Start.do. (2010)
- 8.Hadziyannis SJ, Tassopoulos NC, Heathcote EJ, Chang TT, Kitis G, Rizzetto M, Marcellin P, Lim SG, Goodman Z, Wulfsohn MS, Xiong S, Fry J, Brosgart CL. Adefovir dipivoxil for the treatment of hepatitis B e antigen-negative chronic hepatitis B. N. Engl. J. Med. 2003;348(9):800–807. doi: 10.1056/NEJMoa021812. [DOI] [PubMed] [Google Scholar]
- 9.Janssen HL, van Zonneveld M, Senturk H, Zeuzem S, Akarca US, Cakaloglu Y, Simon C, So TM, Gerken G, de Man RA, Niesters HG, Zondervan P, Hansen B, Schalm SW. Pegylated interferon alfa-2b alone or in combination with lamivudine for HBeAg-positive chronic hepatitis B: a randomised trial. Lancet. 2005;365(9454):123–129. doi: 10.1016/S0140-6736(05)17701-0. [DOI] [PubMed] [Google Scholar]
- 10.Kanwal F, Gralnek IM, Martin P, Dulai GS, Farid M, Spiegel BM. Treatment alternatives for chronic hepatitis B virus infection: a cost-effectiveness analysis. Ann. Intern. Med. 2005;142(10):821–831. doi: 10.7326/0003-4819-142-10-200505170-00007. [DOI] [PubMed] [Google Scholar]
- 11.Fattovich G, Bortolotti F, Donato F. Natural history of chronic hepatitis B: special emphasis on disease progression and prognostic factors. J. Hepatol. 2008;48:335–352. doi: 10.1016/j.jhep.2007.11.011. [DOI] [PubMed] [Google Scholar]
- 12.Fattovich G, Pantalena M, Zagni I, Realdi G, Schalm SW, Christensen E. Effect of hepatitis B and C virus infections on the natural history of compensated cirrhosis: a cohort study of 297 patients. Am. J. Gastroenterol. 2002;97(11):2886–2895. doi: 10.1111/j.1572-0241.2002.07057.x. [DOI] [PubMed] [Google Scholar]
- 13.Fattovich G, Giustina G, Schalm SW, Hadziyannis S, Sanchez-Tapias J, Almasio P, Christensen E, Krogsgaard K, Degos F, Carneiro de Moura M, et al. Occurrence of hepatocellular carcinoma and decompensation in western European patients with cirrhosis type B. The EUROHEP Study Group on Hepatitis B Virus and Cirrhosis. Hepatology. 1995;21(1):77–82. doi: 10.1002/hep.1840210114. [DOI] [PubMed] [Google Scholar]
- 14.Realdi G, Fattovich G, Hadziyannis S, Schalm SW, Almasio P, Sanchez-Tapias J, Christensen E, Giustina G, Noventa F. Survival and prognostic factors in 366 patients with compensated cirrhosis type B: a multicenter study. The Investigators of the European Concerted Action on Viral Hepatitis (EUROHEP) J. Hepatol. 1994;21(4):656–666. doi: 10.1016/S0168-8278(94)80115-0. [DOI] [PubMed] [Google Scholar]
- 15.Kanwal F, Farid M, Martin P, Chen G, Gralnek IM, Dulai GS, Spiegel BM. Treatment alternatives for hepatitis B cirrhosis: a cost-effectiveness analysis. Am. J. Gastroenterol. 2006;101(9):2076–2089. doi: 10.1111/j.1572-0241.2006.00769.x. [DOI] [PubMed] [Google Scholar]
- 16.Chang TT, Gish RG, de Man R, Gadano A, Sollano J, Chao YC, Lok AS, Han KH, Goodman Z, Zhu J, Cross A, DeHertogh D, Wilber R, Colonno R, Apelian D. A comparison of entecavir and lamivudine for HBeAg-positive chronic hepatitis B. N. Engl. J. Med. 2006;354(10):1001–1010. doi: 10.1056/NEJMoa051285. [DOI] [PubMed] [Google Scholar]
- 17.Lai CL, Shouval D, Lok AS, Chang TT, Cheinquer H, Goodman Z, DeHertogh D, Wilber R, Zink RC, Cross A, Colonno R, Fernandes L. Entecavir versus lamivudine for patients with HBeAg-negative chronic hepatitis B. N. Engl. J. Med. 2006;354(10):1011–1020. doi: 10.1056/NEJMoa051287. [DOI] [PubMed] [Google Scholar]
- 18.Colonno RJ, Rose RE, Pokornowski K, Baldick CJ, Eggers B, Xu D, Cross A, Tenney DJ. Four year assessment of entecavir resistance in nucleoside naïve and lamivudine refractory patients. J. Hepatol. 2007;46(Suppl. 1):S294. doi: 10.1016/S0168-8278(07)62379-4. [DOI] [Google Scholar]
- 19.Lai CL, Dienstag J, Schiff E, Leung NW, Atkins M, Hunt C, Brown N, Woessner M, Boehme R, Condreay L. Prevalence and clinical correlates of YMDD variants during lamivudine therapy for patients with chronic hepatitis B. Clin. Infect. Dis. 2003;36(6):687–696. doi: 10.1086/368083. [DOI] [PubMed] [Google Scholar]
- 20.Moskovitz DN, Osiowy C, Giles E, Tomlinson G, Heathcote EJ. Response to long-term lamivudine treatment (up to 5 years) in patients with severe chronic hepatitis B, role of genotype and drug resistance. J. Viral Hepat. 2005;12(4):398–404. doi: 10.1111/j.1365-2893.2005.00613.x. [DOI] [PubMed] [Google Scholar]
- 21.Lee YS, Suh DJ, Lim YS, Jung SW, Kim KM, Lee HC, Chung YH, Lee YS, Yoo W, Kim SO. Increased risk of adefovir resistance in patients with lamivudine-resistant chronic hepatitis B after 48 weeks of adefovir dipivoxil monotherapy. Hepatology. 2006;43(6):1385–1391. doi: 10.1002/hep.21189. [DOI] [PubMed] [Google Scholar]
- 22.Chen CH, Wang JH, Lee CM, Hung CH, Hu TH, Wang JC, Lu SN, Changchien CS. Virological response and incidence of adefovir resistance in lamivudine-resistant patients treated with adefovir dipivoxil. Antivir. Ther. 2006;11(6):771–778. [PubMed] [Google Scholar]
- 23.Yeon JE, Yoo W, Hong SP, Chang YJ, Yu SK, Kim JH, Seo YS, Chung HJ, Moon MS, Kim SO, Byun KS, Lee CH. Resistance to adefovir dipivoxil in lamivudine resistant chronic hepatitis B patients treated with adefovir dipivoxil. Gut. 2006;55(10):1488–1495. doi: 10.1136/gut.2005.077099. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Liaw YF, Sung JJ, Chow WC, Farrell G, Lee CZ, Yuen H, Tanwandee T, Tao QM, Shue K, Keene ON, Dixon JS, Gray DF, Sabbat J. Lamivudine for patients with chronic hepatitis B and advanced liver disease. N. Engl. J. Med. 2004;351(15):1521–1531. doi: 10.1056/NEJMoa033364. [DOI] [PubMed] [Google Scholar]
- 25.Colonno RJ, Rose R, Baldick CJ, Levine S, Pokornowski K, Yu CF, Walsh A, Fang J, Hsu M, Mazzucco C, Eggers B, Zhang S, Plym M, Klesczewski K, Tenney DJ. Entecavir resistance is rare in nucleoside naive patients with hepatitis B. Hepatology. 2006;44(6):1656–1665. doi: 10.1002/hep.21422. [DOI] [PubMed] [Google Scholar]
- 26.Tenney DJ, Rose RE, Baldick CJ, Pokornowski KA, Eggers BJ, Fang J, Wichroski MJ, Xu D, Yang J, Wilber RB, Colonno RJ. Long-term monitoring shows hepatitis B virus resistance to entecavir in nucleoside-naive patients is rare through 5 years of therapy. Hepatology. 2009;49(5):1503–1514. doi: 10.1002/hep.22841. [DOI] [PubMed] [Google Scholar]
- 27.Heathcote EJ, Marcellin P, Buti M, Gane E, De Man RA, Krastev Z, Germanidis G, Lee SS, Flisiak R, Kaita K, Manns M, Kotzev I, Tchernev K, Buggisch P, Weilert F, Kurdas OO, Shiffman ML, Trinh H, Gurel S, Snow-Lampart A, Borroto-Esoda K, Mondou E, Anderson J, Sorbel J, Rousseau F. Three-year efficacy and safety of tenofovir disoproxil fumarate treatment for chronic hepatitis B. Gastroenterology. 2011;140(1):132–143. doi: 10.1053/j.gastro.2010.10.011. [DOI] [PubMed] [Google Scholar]
- 28.van Bommel F, Wunsche T, Mauss S, Reinke P, Bergk A, Schurmann D, Wiedenmann B, Berg T. Comparison of adefovir and tenofovir in the treatment of lamivudine-resistant hepatitis B virus infection. Hepatology. 2004;40(6):1421–1425. doi: 10.1002/hep.20464. [DOI] [PubMed] [Google Scholar]
- 29.Sarin, N., Yim, C., Feld, J.J., Heathcote, E.J., Wong, D.K.: Tenofovir is effective salvage therapy for nucleoside-resistant hepatitis B. abstract nr: 454, AASLD 2009 Boston (2009)
- 30.Van Bommel, F., De Man, R., Ferenci, P., Reijnders, J.G., Bronowicki, J.P., Fulop, B., Wedemeyer, H., Erhardt, A., Hueppe, D., Bourliere, M., Sarrazin, C., Trojan, J., Buggisch, P., Petersen, J., Spenger, U., Brost, S., Pariente, A., Schuchmann, M., Wasmuth, H.E., Deterding, K., Rutter, K., Feucht, H.H., Wiedenmann, B., Berg, T.: Long-term follow-up evaluation of the efficacy and safety of tenofovir disoproxil fumarate (TDF) in a european multicenter (nucleos(t)ide experienced) hepatitis B virus HBV infected cohort. abstract nr: 221, AASLD 2009 Boston (2009)
- 31.Reijnders JG, Janssen HL. Potency of tenofovir in chronic hepatitis B: mono or combination therapy? J. Hepatol. 2008;48(3):383–386. doi: 10.1016/j.jhep.2007.12.006. [DOI] [PubMed] [Google Scholar]
- 32.Lau GK, Piratvisuth T, Luo KX, Marcellin P, Thongsawat S, Cooksley G, Gane E, Fried MW, Chow WC, Paik SW, Chang WY, Berg T, Flisiak R, McCloud P, Pluck N. Peginterferon Alfa-2a, lamivudine, and the combination for HBeAg-positive chronic hepatitis B. N. Engl. J. Med. 2005;352(26):2682–2695. doi: 10.1056/NEJMoa043470. [DOI] [PubMed] [Google Scholar]
- 33.Marcellin, P., Bonino, F., Lau, G.K., Farci, P., Yurdaydin, C., Piratvisuth, T., Jin, R., Gurel, S., Lu, Z.M., Wu, J., Popescu, M., Hadziyannis, S.: Sustained response of hepatitis B e antigen-negative patients 3 years after treatment with peginterferon alpha-2a. Gastroenterology 136(7), 2169–2179 e2161–2164 (2009) [DOI] [PubMed]
- 34.Cooksley WG, Piratvisuth T, Lee SD, Mahachai V, Chao YC, Tanwandee T, Chutaputti A, Chang WY, Zahm FE, Pluck N. Peginterferon alpha-2a (40 kDa): an advance in the treatment of hepatitis B e antigen-positive chronic hepatitis B. J. Viral Hepat. 2003;10(4):298–305. doi: 10.1046/j.1365-2893.2003.00450.x. [DOI] [PubMed] [Google Scholar]
- 35.Piratvisuth T, Lau G, Chao YC, Jin R, Chutaputti A, Zhang QB, Tanwandee T, Button P, Popescu M. Sustained response to peginterferon alfa-2a (40 kD) with or without lamivudine in Asian patients with HBeAg-positive and HBeAg-negative chronic hepatitis B. Hepatol. Int. 2008;2(1):102–110. doi: 10.1007/s12072-007-9022-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Fleurence RL, Hollenbeak CS. Rates and probabilities in economic modelling: transformation, translation and appropriate application. Pharmacoeconomics. 2007;25(1):3–6. doi: 10.2165/00019053-200725010-00002. [DOI] [PubMed] [Google Scholar]
- 37.Kennedy PT, Phillips N, Chandrasekhar J, Jacobs R, Jacobs M, Dusheiko G. Potential and limitations of lamivudine monotherapy in chronic hepatitis B: evidence from genotyping. Liver Int. 2008;28(5):699–704. doi: 10.1111/j.1478-3231.2008.01717.x. [DOI] [PubMed] [Google Scholar]
- 38.Shouval D, Lai CL, Chang TT, Cheinquer H, Martin P, Carosi G, Han S, Kaymakoglu S, Tamez R, Yang J, Tenney D, Brett-Smith H. Relapse of hepatitis B in HBeAg-negative chronic hepatitis B patients who discontinued successful entecavir treatment: the case for continuous antiviral therapy. J. Hepatol. 2009;50(2):289–295. doi: 10.1016/j.jhep.2008.10.017. [DOI] [PubMed] [Google Scholar]
- 39.Reijnders JG, Perquin MJ, Zhang N, Hansen BE, Janssen HL. Nucleos(t)ide analogues only induce temporary hepatitis B e antigen seroconversion in most patients with chronic hepatitis B. Gastroenterology. 2010;139(2):491–498. doi: 10.1053/j.gastro.2010.03.059. [DOI] [PubMed] [Google Scholar]
- 40.Marcellin P, Lau GK, Bonino F, Farci P, Hadziyannis S, Jin R, Lu ZM, Piratvisuth T, Germanidis G, Yurdaydin C, Diago M, Gurel S, Lai MY, Button P, Pluck N. Peginterferon alfa-2a alone, lamivudine alone, and the two in combination in patients with HBeAg-negative chronic hepatitis B. N. Engl. J. Med. 2004;351(12):1206–1217. doi: 10.1056/NEJMoa040431. [DOI] [PubMed] [Google Scholar]
- 41.Keeffe EB, Zeuzem S, Koff RS, Dieterich DT, Esteban-Mur R, Gane EJ, Jacobson IM, Lim SG, Naoumov N, Marcellin P, Piratvisuth T, Zoulim F. Report of an international workshop: roadmap for management of patients receiving oral therapy for chronic hepatitis B. Clin. Gastroenterol. Hepatol. 2007;5(8):890–897. doi: 10.1016/j.cgh.2007.05.004. [DOI] [PubMed] [Google Scholar]
- 42.Chang TT. On-treatment monitoring of HBV DNA levels: predicting response and resistance to oral antiviral therapy at week 24 versus week 48. Hepatol. Int. 2009;3(Suppl 1):16–23. doi: 10.1007/s12072-009-9143-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Lai CL, Gane E, Liaw YF, Hsu CW, Thongsawat S, Wang Y, Chen Y, Heathcote EJ, Rasenack J, Bzowej N, Naoumov NV, Di Bisceglie AM, Zeuzem S, Moon YM, Goodman Z, Chao G, Constance BF, Brown NA. Telbivudine versus lamivudine in patients with chronic hepatitis B. N. Engl. J. Med. 2007;357(25):2576–2588. doi: 10.1056/NEJMoa066422. [DOI] [PubMed] [Google Scholar]
- 44.Hadziyannis AS, Mitsoula PV, Hadziyannis SJ. Prediction of long-term maintenance of virologic response during lamivudine treatment in HBeAg-negative chronic hepatitis B. Hepatology. 2007;46(Suppl. 1):667A. [Google Scholar]
- 45.Turkish Health Ministry: Turkish Health Ministry Drugs and pharmaceutical head quarters. vol. 2009, December http://www.iegm.gov.tr/Default.aspx?sayfa=fiyat_listesi (2010)
- 46.Levy AR, Kowdley KV, Iloeje U, Tafesse E, Mukherjee J, Gish R, Bzowej N, Briggs AH. The impact of chronic hepatitis B on quality of life: a multinational study of utilities from infected and uninfected persons. Value Health. 2008;11(3):527–538. doi: 10.1111/j.1524-4733.2007.00297.x. [DOI] [PubMed] [Google Scholar]
- 47.Gold MR, Siegel JE, Russel LB, Weinstein MG. Cost-Effectiveness in Health and Medicine. New York: Oxford University Press; 1996. [Google Scholar]
- 48.Drummond MF, Jefferson TO. Guidelines for authors and peer reviewers of economic submissions to the BMJ the BMJ economic evaluation working party. BMJ. 1996;313(7052):275–283. doi: 10.1136/bmj.313.7052.275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.World Health Organization: WHO guide to cost-effectiveness. In., p. http://www.who.int/choice/publications/p_2003_generalised_cea.pdf (2003)
- 50.Karasu Z, Akyildiz M, Kilic M, Zeytunlu M, Aydin U, Tekin F, Yilmaz F, Ozacar T, Akarca U, Ersoz G, Gunsar F, Ilter T, Lucey MR. Living donor liver transplantation for hepatitis B cirrhosis. J. Gastroenterol. Hepatol. 2007;22(12):2124–2129. doi: 10.1111/j.1440-1746.2006.04782.x. [DOI] [PubMed] [Google Scholar]
- 51.Woo, G., Tomlinson, G., Nishikawa, Y., Kowgier, M., Sherman, M., Wong, D.K., Pham, B., Ungar, W.J., Einarson, T.R., Heathcote, E.J., Krahn, M.: Tenofovir and entecavir are the most effective antiviral agents for chronic hepatitis B: a systematic review and bayesian meta-analyses. Gastroenterology 139(4), 1218–1229 e1215 (2010). doi:10.1053/j.gastro.2010.06.042 [DOI] [PubMed]
- 52.Akarca US. Chronic hepatitis B. A guideline to diagnosis, approach, management, and follow-up 2007. Turkish Association for the Study of Liver. Turk. J. Gastroenterol. 2008;19(4):207–230. [PubMed] [Google Scholar]
- 53.Toy M, Veldhuijzen IK, de Man RA, Richardus JH, Schalm SW. Potential impact of long-term nucleoside therapy on the mortality and morbidity of active chronic hepatitis B. Hepatology. 2009;50(3):743–751. doi: 10.1002/hep.23061. [DOI] [PubMed] [Google Scholar]
- 54.Wong JB, Koff RS, Tine F, Pauker SG. Cost-effectiveness of interferon-alpha 2b treatment for hepatitis B e antigen-positive chronic hepatitis B. Ann. Intern. Med. 1995;122(9):664–675. doi: 10.7326/0003-4819-122-9-199505010-00004. [DOI] [PubMed] [Google Scholar]
- 55.Spackman DE, Veenstra DL. A cost-effectiveness analysis of currently approved treatments for HBeAg-positive chronic hepatitis B. Pharmacoeconomics. 2008;26(11):937–949. doi: 10.2165/00019053-200826110-00006. [DOI] [PubMed] [Google Scholar]
- 56.Shepherd, J., Jones, J., Takeda, A., Davidson, P., Price, A.: Adefovir dipivoxil and pegylated interferon alfa-2a for the treatment of chronic hepatitis B: a systematic review and economic evaluation. Health Technol. Assess. 10(28), iii–iv, xi–xiv, 1–183 (2006) [DOI] [PubMed]
- 57.Buti M, Brosa M, Casado MA, Rueda M, Esteban R. Modeling the cost-effectiveness of different oral antiviral therapies in patients with chronic hepatitis B. J. Hepatol. 2009;51(4):640–646. doi: 10.1016/j.jhep.2009.04.013. [DOI] [PubMed] [Google Scholar]
- 58.Barbieri M, Drummond M, Willke R, Chancellor J, Jolain B, Towse A. Variability of cost-effectiveness estimates for pharmaceuticals in Western Europe: lessons for inferring generalizability. Value Health. 2005;8(1):10–23. doi: 10.1111/j.1524-4733.2005.03070.x. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.