

Abstract
Background
The co-occurrence of suicidal ideation, depression, and conduct disturbance is likely explained in part by correlated genetic and environmental risk factors. Little is known about the specific nature of these associations.
Method
Structured interviews on 2814 twins from the Virginia Twin Study of Adolescent Behavioral Development (VTSABD) and young adult follow-up (YAFU) yielded data on symptoms of depression, conduct disorder and adolescent and young adult suicidal ideation.
Results
Univariate analyses revealed that the familial aggregation for each trait was explained by a combination of additive genetic and shared environmental effects. Suicidal ideation in adolescence was explained in part by genetic influences, but predominantly accounted for by environmental factors. A mixture of genetic and shared environmental influences explained ideation occurring in young adulthood. Multivariate analyses revealed that there are genetic and shared environmental effects common to suicidal ideation, depression, and conduct disorder. The association between adolescent suicidal ideation and CD was attributable to the same genetic and environmental risk factors for depression.
Conclusions
These findings underscore that prevention and intervention strategies should reflect the different underlying mechanisms involving depression and conduct disorder to assist in identifying adolescents at suicidal risk.
INTRODUCTION
Suicide is the third leading cause of death in adolescents (Centers for Disease Control and Prevention, 2007) underscoring the urgent need for advancing knowledge and research regarding the causes and prevention of suicide in young people (Goldsmith, Pellmar, Kleinman, & Bunney, 2002). Increased understanding of the underlying processes leading to suicide attempts and death by suicide, including its familial nature and association with other disorders, is needed to inform prevention and intervention efforts.
Over eighty percent of youth referred for suicide attempts and 90% of those who complete suicide have an associated psychiatric disorder - the most common being depression. (Gould, Greenberg, Velting, & Shaffer, 2003) (Bridge, Goldstein, & Brent, 2006). Depressive disorder, particularly with co-occurring disruptive behavior or anxiety disorder, confers an increased risk to all forms of suicidal behaviors including thoughts, plans and attempts (Thompson, Kuruwita, & Foster, 2009; Foley, Goldston, Costello, & Angold, 2006; Spirito & Esposito-Smythers, 2006). The association between suicidality and externalizing disorders (Hills, Cox, McWilliams, & Sareen, 2005) is also well documented and combined with depression, increases the risk of suicidal behavior (Asarnow et al., 2008). Conduct disorders, co-occurring with mood, anxiety, and substance abuse disorders, are found in girls with a history of suicidal behavior (Glowinski, et al, 2001) and in one-third of adolescent male suicides (Gould, et al, 2003). Conduct disorder also appears to confer an independent effect on suicidal behavior controlling for depression (Brent et al., 1993; Foley et al., 2006).
Familial factors are influential in liability to suicidal behavior - twin, family, and adoption studies of adults (Brent & Mann, 2005; Bondy, Buettner, & Zill, 2006) all show significantly higher rates of suicidal behavior in the families of suicidal probands (Brent & Melham, 2008). The concordance rates for suicidal ideation, suicide attempts (Statham et al., 1998) and completed suicides (Roy & Segal, 2001; Roy, Segal, & Sarchiapone, 1995) are consistently higher in MZ than DZ twins with genetic factors accounting for nearly half of the variation in both suicidal attempts and ideation (Statham et al., 1998). In the Statham et al. twin study, the examination of epidemiological correlates in adult probands show that lifetime suicidal ideation, plans and attempts were associated with depression in men and women, and with childhood conduct problems in women. However, in the same study, genetic influences were only partially explained by Axis I disorders. Fu et al. (2002) showed that genetic effects were significant for suicidal attempts even controlling for psychopathology and sociodemographic variables, including marital and employment status, mood, anxiety, substance abuse, antisocial, and childhood conduct disorder, implicating. These studies suggest overlapping genetic risk factors to suicidal behavior and psychopathology, but also genetic effects specific to suicidal behavior.
Suicidal behavior in adolescents also has a strong heritable component (Cho, Guo, Iritani, & Hallifors, 2006; Glowinski et al., 2001) and is linked with other genetically mediated disorders including adolescent depression and conduct disorder (Silberg, Maes, & Eaves, 2010; Eaves et al., 1997; Rhee & Waldman, 2002). Despite consistent work demonstrating strong associations amongst these behaviors, little is known about the genetic and environmental mechanisms underlying them.
To address this, psychiatric data collected on a large population based sample of juvenile twins followed from middle childhood into young adulthood, was analyzed for estimating the extent to which the phenotypic associations between depression, conduct disorder, and suicidal ideation can be accounted for by a shared genetic and/or environmental diathesis. (Brent et al., 2003; Brent & Bridge, 2007; Brent & Mann, 2005).
We had three overarching goals: 1) investigate the degree of association between adolescent suicidal ideation, depression, conduct disorder, and young adult suicidiality; 2) estimate the influence of genetic, shared, and non-shared environmental factors on suicidal thoughts in adolescence and young adulthood; 3) determine to what extent the associations amongst the traits are accounted for by latent genetic and environmental risk factor(s).
METHODS
Ascertainment
Data for the present study was collected as part of the Virginia Twin Study of Adolescent Behavioral Development (VTSABD), a multi-wave, population-based, cohort–sequential study of twins between the ages of 8 and 17 and their follow-up into young adulthood. The sample was ascertained by statewide recruitment through Virginia schools. The twins were between the ages of 8 and 17 when they entered the study, and were followed up through three waves of data collection while the twins were younger than 18. Of the 1894 twin pairs initially eligible, 74.5% participated in the first wave of data collection (n=1412); 1047 of the 1302 families that continued to meet age and residence requirements completed the second wave of the study (80% participation rate); 628 of the 777 eligible twin families participated in the third wave (81% participation rate). The Young Adult Follow-Up (YAFU) is the outcome study of all the twins who participated in at least one wave of the VTSABD. At 18 years or older, these twins were re-contacted and evaluated as young adults. Of the 2,824 subjects who were considered eligible for participation in the YAFU, data was collected on 2,282 or 80% of the twins. Ages of the YAFU sample ranged from 18 to 27 with a mean age of 21.4.
Measurement
The twins were evaluated using an extensive psychiatric battery. The Child and Adolescent Psychiatric Assessment (CAPA) (Angold et al., 1995) was administered to both twins and at least one parent in a face-to-face interview format. The CAPA requires that a symptom be present in several activities and be at least somewhat uncontrollable.
Suicidal Thoughts and Behaviors
Suicidality represents a continuum, ranging from passive thoughts of death to completed attempts (O’Carroll et al., 1996; Asarnow et al., 2008). Given the low prevalence of suicide attempts in a population sample of adolescents, we chose to focus on suicidal ideation, which often precedes attempts, and is a strong predictor of completed suicide (Kessler, Berglund, Borges, Noch, & Wang, 2005; Brown, Beck, Steer, & Grisham, 2000; Lewinsohn, Seeley, Hibbard, Rohde, & Sack, 1996).
Suicidal ideation in the juvenile twins was assessed as thoughts about killing oneself in the previous three months. Suicidal ideation reflected thoughts about wanting to die, not being able to go on any longer, and life not being worth living that were at least somewhat intrusive, recurring, and uncontrollable. Those who endorsed suicidal ideation were assigned a score of ‘1’ and those who did not, a score of ‘0’. A depression score was child-report based and was scored as a dichotomous variable, with depression being present if two or more symptoms comprising a diagnosis of depression were endorsed in the previous three months. The presence of Conduct Disorder was based on three or more symptoms being endorsed by either the mother or the child. Those with 3 or more symptoms were considered to be Conduct Disordered. In the young adult study (YAFU) the twins were asked if they felt like harming themselves, as part of an assessment for diagnosing Major Depression. (Kendler et al., 1993).
Methodology
Data preparation
Data were prepared for raw ordinal data analysis in the software Mx (Neale, Boker, Xie, and Maes, 2006). This approach assumes that the observed ordinal categories within each item are an imprecise measure of a latent normal distribution of liability, and that this liability distribution has one or more threshold values which discriminate between the categories (Sullivan and Eaves, 2002). Thresholds can be conceived of as cut points along a standard normal distribution which classify individuals in terms of a probability or risk of endorsing one of two or more discrete (ordinal) categories. All thresholds were adjusted for the linear effects of age and sex.
Statistical analyses
Univariate & multivariate modeling
Standard biometrical genetic model fitting methods were used (Neale and Cardon, 1992) to decompose or explain the observed variation in depression, conduction disorder and suicide ideation in terms of additive genetic (A), shared environmental (C) and non-shared or unique environmental (E) risks. Additive gene action (A) reflects the additive or average effect of individual alleles at genetic loci influencing a trait or behavior. Common environmental effects (C) describe influences which make family members more alike compared to random pairs of individuals. Non-shared or unique environmental risks (E) capture aspects of the environment that are unique to each individual and are therefore uncorrelated between siblings. Since MZ twin pairs are genetically identical, the additive genetic correlation is fixed to 1.0. The additive genetic correlation for DZ twin pairs is fixed to 0.5 because on average DZ twin pairs share only half their genes in common. An important assumption of this biometrical model is that shared environmental effects correlate to an equal extent in MZ and DZ twin pairs. Non-shared environmental effects (E) are by definition uncorrelated and also include measurement error including short-term fluctuations of the environment.
With multivariate data it is possible to make use of the additional information in the cross-twin cross-trait correlations to determine the degree of genetic and environmental overlap between depression, CD and suicidal ideation (Martin and Eaves, 1977). The most commonly used multivariate method for this aim is the Cholesky Decomposition (Neale and Cardon, 1992) which we fitted using the Mx software package ((Neale, Boker, Xie, and Maes, 2006). The Cholesky is a method of triangular decomposition where the first variable (depression) is assumed to be caused by a latent factor (A1) that can explain the variance in the remaining variables (CD & suicidal ideation). The second variable (CD) is assumed to be caused by a second latent factor (A2) that can explain variation in the second as well as remaining variables. In this way, the second latent factor is restrained from explaining variance in the first observed variable. This pattern continues until the final observed variable, suicidal ideation, is explained by a latent variable (A3), which is constrained from explaining the variance in any of the previous observed variables. A Cholesky decomposition is specified for each latent source of variance of Additive Gene Effects (A), Shared Environment (C), and Individual Specific Environment (E).
RESULTS
Univariate & multivariate model fitting
Correlations shown in Table 1 between the four measures were moderate to high. Highest correlations were between depression and suicide within adolescence (.62). The lowest correlations were between juvenile depression and young adult suicidal ideation (.27) and between juvenile conduct disorder and suicidal ideation in young adulthood (.19). There was a moderate correlation between adolescent and young adult suicide ideation (.45). For each variable, the DZ twin pair correlation was greater than half the MZ counterpart suggesting that more shared environment and less additive genetic factors may explain the familial aggregation.
Table 1.
Sample size, endorsements1, monozygotic (MZ) & dizygotic (DZ) twin pair correlations, polychoric correlations & standard variances components2 based on univariate twin analyses3.
| Phenotype | N | % | 1. | 2. | 3. | 4. | MZ | 95%CI | DZ | 95%CI | A (95%CI) | C (95%CI) | E (95%CI) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Depression | 2697 | 0.07 | 1 | 0.43 | 0.25 – 0.59 | 0.40 | 0.20 – 0.58 | 0.05 (0.00–0.55) | 0.38 (0.00–0.54) | 0.57 (0.41–0.72) | |||
| 2. Conduct Disorder | 2801 | 0.09 | 0.41 | 1 | 0.55 | 0.37 – 0.71 | 0.42 | 0.18 – 0.63 | 0.18 (0.00–0.67) | 0.35 (0.00–0.62) | 0.47 (0.32–0.64) | ||
| 3. Juvenile Ideation | 2802 | 0.02 | 0.62 | 0.41 | 1 | 0.33 | −0.02 – 0.61 | 0.39 | 0.05 – 0.66 | 0.00 (0.00–0.60) | 0.36 (0.00–0.57) | 0.64 (0.39–0.88) | |
| 4. Adult Ideation | 2227 | 0.05 | 0.27 | 0.19 | 0.45 | 1 | 0.51 | 0.26 – 0.71 | 0.34 | 0.08 – 0.56 | 0.35 (0.00–0.71) | 0.17 (0.00–0.56) | 0.49 (0.29–0.73) |
These represent the standard normal cumulative distribution based on Maximum Likelihood threshold estimates.
A = additive genetic, C = common or shared environment, E = non-shared environment & measurement error.
All estimates adjusted for sex differences on item thresholds.
Standardized proportions of variance components attributable to additive genetic effects, A, shared environmental effects, C and individual specific environmental effects, E are also shown. Notwithstanding the wide 95% confidence intervals, nearly all of the familial aggregation in depression, conduct disorder, and childhood suicidal ideation can be explained by shared environmental risks ranging from 35% to 38% of the total variance. Additive genetic risk factors explained between 5% and 18% of the variance in depression and conduct disorder, respectively. From the univariate analysis, there was no apparent influence of genetic factors on suicidal ideation in adolescence – the variation could be attributable to aspects of the shared and non-shared environment. This pattern was reversed for young adult suicidal ideation; familial aggregation was explained by more additive genetic (35%) than shared environmental risk factors (17%).
In the multivariate analyses of all four variables in Tables 2, the E model that predicted no familial aggregation fitted the data poorly. The CE and the AE model provided comparably good fits to the data. Because there was insufficient power to choose between these models, the saturated ACE model was retained as the best fitting.
Table 2.
Multivariate comparison of the saturated ACE Cholesky, AE, CE and E submodels.
| Model | LL | df | ΔLL | Δdf | p | AIC |
|---|---|---|---|---|---|---|
| ACE | 4505.66 | 10493 | −16480.34 | |||
| AE | 4514.85 | 10503 | 9.20 | 10 | 0.51 | −16491.15 |
| CE | 4508.10 | 10503 | 2.45 | 10 | 0.99 | −16497.90 |
| E | 4634.46 | 10513 | 128.80 | 20 | *** | −16391.54 |
These represent the standard normal cumulative distribution based on Maximum Likelihood threshold estimates.
A = additive genetic, C = common or shared environment, E = non-shared environment & measurement error.
All estimates adjusted for sex differences on item thresholds.
Although larger proportions of familial aggregation for childhood suicidal ideation from the univariate results suggest a greater role of shared environmental risks compared to additive genetic factors, the confidence intervals are approximately equal and owing to lack of power are wide and span zero. The additional information from the cross-twin cross-trait correlations in the multivariate analyses increases the power to detect sources of genetic and environmental variance (e.g., genetic effects on childhood suicidal ideation) as well as covariance between the measures.
In Table 3, the first additive genetic risk factor loaded across all four variables. The polychoric correlations between all four additive genetic risk factors were high, ranging from 0.77 to 0.99. This suggests that a large proportion of the genetic variance is shared in common across measures. Although lower, the shared environmental correlations also account for the association amongst the four traits. Shared environmental risks in depression appear to be indexing liability to suicidal ideation, and to a lesser extent conduct disorder and young adult suicidal ideation shown by moderately high paths on the first common environmental factor. The loadings of CD and suicidal ideation on the single common factor and combined with a relatively small specific genetic and environmental paths for the two traits (.07 and −.08, respectively) reveals that any association between suicidal ideation and CD is explained primarily by the genetic and environmental risk factors influencing depression. The effect of the non-shared environment is mostly variable specific except for a modest association between depression and suicidal ideation, likely reflecting individual specific negative life events. The results from the modeling of the four variables are also presented in Figure 1.
Table 3.
Standardized pathway coefficients and correlations between the additive genetic, shared environmental & non-shared environment latent factors based on the saturated ACE Cholesky model1.
| Standardized pathway coefficients | Correlations between latent factors | |||||||
|---|---|---|---|---|---|---|---|---|
| Additive Genetic | 1. | 2. | 3. | 4. | 1. | 2. | 3. | 4. |
| 1. Depression | 0.29 | 1 | ||||||
| 2. Conduct Disorder | 0.46 | 0.16 | 0.94 | 1 | ||||
| 3. Suicide Ideation | 0.33 | 0.07 | −0.01 | 0.98 | 0.99 | 1 | ||
| 4. Adult Ideation | 0.40 | 0.13 | 0.20 | 0.22 | 0.77 | 0.81 | 0.80 | 1 |
| Shared Environment | ||||||||
| 1. Depression | 0.60 | 1 | ||||||
| 2. Conduct Disorder | 0.33 | 0.45 | 0.59 | 1 | ||||
| 3. Suicide Ideation | 0.56 | −0.08 | 0.21 | 0.93 | 0.45 | 1 | ||
| 4. Adult Suicide | 0.27 | −0.23 | 0.35 | −0.01 | 0.55 | −0.05 | 0.81 | 1 |
| Non-shared environment | ||||||||
| 1. Depression | 0.74 | 1 | ||||||
| 2. Conduct Disorder | 0.09 | 0.67 | 0.13 | 1 | ||||
| 3. Suicide Ideation | 0.25 | 0.12 | 0.66 | 0.35 | 0.21 | 1 | ||
| 4. Adult Ideation | 0.00 | 0.00 | 0.13 | 0.69 | 0.00 | 0.01 | 0.17 | 1 |
All estimates adjusted for sex differences on item thresholds.
Figure 1.
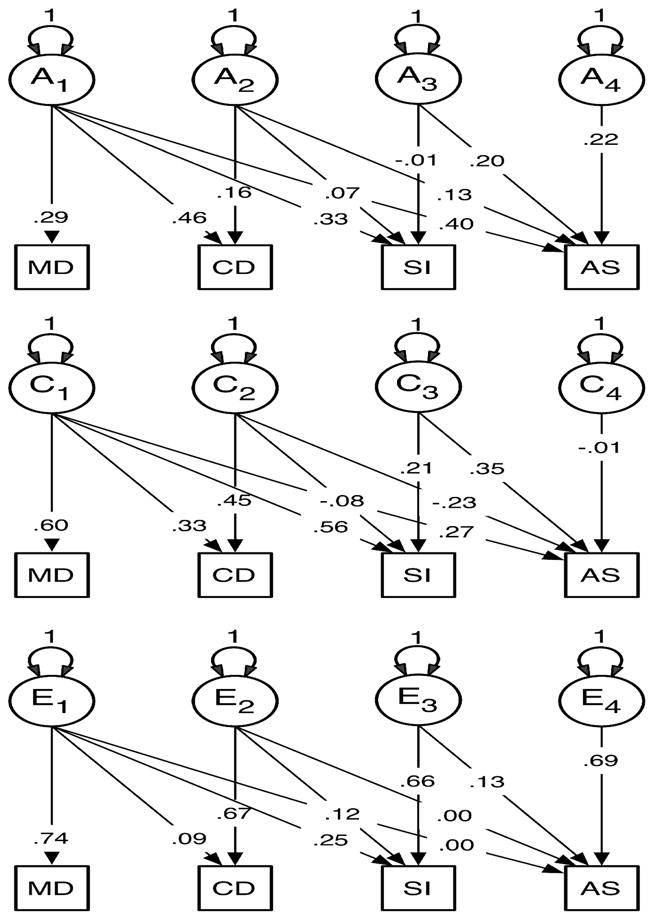
Paramater estimates for Additive Genetic (A), Shared Environmental (C), and Unique Environmental Components (E) under Full Cholesky Decomposition Model for Adolescent Depression (MD), Conduct Disorder (CD), Suicidal Ideation (SI), and Young Adult Ideation (AI).
DISCUSSION
Previous research has suggested that suicidal ideation and suicide attempts are on a continuum of risk with suicidal ideation representing an important precursor of more severe levels of suicidal behavior (Asarnow, 2008). While suicidal ideation is more common than suicide attempts, even the lower level of suicidality represented by ideation may be prognostic of suicidal behavior later in development (Thompson, Kuruwita, and Foster, 2009; Reuter, Holm, McGeorge, Conger, 2008). Within this sample of juvenile twins, 3% of the children endorsed significant suicidal ideation in the past three months. Our rate is higher than the prevalence rate of .69 percent found in other population studies (Foley, et al, 2006) but lower than that reported from the Youth Risk Behavior Surveillance Survey (Centers for Disease Control and Prevention, 2008). The latter reported a rate of 14.5 percent of youth had “seriously thought about suicide” in the previous 12 months. The discrepancies of prevalence rates across studies are likely a reflection of age range of the sample, methodology of data collection (interview versus survey), time span for reporting (past three months versus past year or lifetime), and threshold for inclusion (fleeting thoughts versus more intrusive, recurring, and uncontrollable thoughts of suicide).
Suicidal behavior does not occur in isolation, but frequently co-occurs with both internalizing and externalizing disorders. As reported in previous studies (Haavisto, Sourander, Ellila, Valimaki, and Santalahi, and Helenius, 2003; Kelly, Lynch, Donovan, and Clark, 2001) we find a significant association amongst these traits. Although numerous empirical and theoretical studies have demonstrated strong co-occurrences amongst these traits this is the first study to elucidate how they may be related.
The association between depression, conduct disturbance, and adolescent and young adult suicidal ideation can be explained by both common genetic and shared environmental risk factors. The genetic correlations among the latent factors comprising these traits are all high, consistent with a common genetic liability to adolescent suicidality that involves both a mood and behavioral component.
The predominance of shared environmental influences on adolescent suicidal ideation contrasts with its smaller effect in young adulthood. The finding that the effects of the family and shared environment are large in juveniles and smaller or absent in adults is not confined to suicidal behavior. Twin data show a sharp change in the role genes and the family environment at the time juveniles make the transition to independent adult living at which time the role of the shared environment declines rapidly to be replaced by long-term genetic influences (Eaves et al., 1997b, 2010). The importance of shared environmental influences on conduct disturbance in adolescence that diminishes in the transition to young adulthood is an example of a similar process of developmental change (Silberg, Maes, and Eaves 2010).
Our heritability estimate of approximately 30% for suicidal ideation is comparable with estimates reported from other large scale population studies of adult twins (Statham et al., 1998; Voracek and Loibl (2007). Evidence that there are specific genetic effects for suicidal ideation in adulthood apart from other psychiatric syndromes is also consistent with other findings (Fu et al., 1998).
The environmental structure also shows a strong association between all four traits. Despite the phenotypic association between CD and ideation and the large genetic and shared environmental correlation between them, there is little genetic or environmental overlap specific to these traits – rather any association appears to be driven by genetic and environmental effects shared in common with depression. These findings suggest that interventions with suicidal adolescents with (and without) conduct cisorder should focus primarily on the mood disturbance.
The effect of the shared environment on suicidal ideation and depression underscores the importance of identifying and evaluating putative environmental risk factors including peer effects, poor parent-child interactions, parental psychopathology, abuse and neglect (Hawton and Fortune, 2008) in suicidal youth. The association between mood and conduct disturbance and suicidal behavior and their genetic and to a less extent environmental relatedness has important implications for clinical conceptualization and treatment. Youth with conduct disorder may not be adequately assessed for mood disturbance or suicide risk, as these youth are often conceptualized as being behaviorally, rather than emotionally, disturbed. Given the small overlap between CD and suicidality apart from depression, interventions should focus on depression that conduct disordered youth present. In the face of the significant behavioral challenges that these youth present, feelings of depression may go unnoticed, and if left untreated, may progress toward suicide attempts. For youth that present as depressed, assessment of conduct symptoms, as additional indicators of genetic risk, should also be considered.
Limitations of this study and future directions
Because of the low endorsement of suicidal behavior, the most important limitation of this study is insufficient power to resolve the effects of genetic and shared environmental factors. We report parameter estimates based upon best fitting ACE models.
Further, given the way suicidal ideation is asked of the children, then as adults, it is possible that the differences in the pattern of genetic and environmental influence may be methodological rather than reflect genuine etiological differences. We do no assume that self-report measures are homogenous constructs. However, the additive genetic latent factor correlations are very high. Not withstanding the limitations of the modeling, these results suggest a great deal of biological overlap.
Previous work has shown important etiological differences in depression before and after puberty Harrington, 1993; Silberg et al., 1999). Because of the low prevalence rates for suicidal ideation our analyses we were limited to global age categories. Both age and gender differences are potentially important areas for ongoing research, given the possibility of differences in the effect of genes and environment. Moreover, the association between suicidality and anxiety, and suicide and drug use (Glowinski, et al, 2001), observed phenotypically, can be examined in future structural equation modeling analyses to identify more precisely their role in terms of the genetic and environmental pathways to suicide ideation.
We acknowledge that our model fitting was by no means exhaustive. Our analyses were intended as exploratory and in the absence of an explicit model or aim to test direction of causation we chose the agnostic Cholesky Decomposition as our starting point for future research. In the absence of theoretical or temporal ordering of the variables, the Cholesky decomposition is merely an arbitrary mathematical device to yield positive definite estimates of the genetic and environmental matrices of genetic and environmental components of variance and covariance (Fulker et al., 1983). In our application, we have partial temporal and causal ordering because we consider suicidality to be causally dependent on genetic and environmental components of adolescent psychopathology and adult suicidality as partially contingent of adolescent behavior. The causal ordering of depression and conduct disorder is arbitrary and cannot usually be resolved in the absence of repeated measures or covariates of known causal priority (such as genome-based indices of genetic liability). Although we can re-arrange the ordering of depression and CD in the Cholesky, this will not order the overall model fit, nor will re-ordering alter the proportion of genetic and environmental variance explained in juvenile and adult suicidal ideation by depression, conduct disorder, and adolescent suicidality. Different conceptions of the multivariate genetic and environmental covariance structure are possible but cannot be resolved with these small samples and restricted set of variables.
Acknowledgments
Supported by grants MH-55557, MH-62368 (JLS) and MH-068521 (LJE) from the National Institute of Mental Health, and UL1RR031990 from the National Center for Research Resources. We want to thank the Mid-Atlantic Twin Registry (MATR) for the recruitment of twin families.
References
- Angold A, Prendergast M, Cox A, Harrington R, Simonoff E, Rutter M. Psychological Medicine. 1995 Jul;25(4):739–754. doi: 10.1017/s003329170003498x. [DOI] [PubMed] [Google Scholar]
- Asarnow J, Baraff L, Berk M, Grob C, Devich-Navarro M, Suddath R, Piacentini J, Tang L. Pediatric emergency department suicidal patients: Two-site evaluation of suicide ideators, single attempters, and repeat attempters. Journal of the American Academy of Child and Adolescent Psychiatry. 2008;47:958–966. doi: 10.1097/CHI.0b013e3181799ee8. [DOI] [PubMed] [Google Scholar]
- Bondy B, Buettner A, Zill P. Genetics of suicide. Molecular Psychiatry. 2006;11(4):336–351. doi: 10.1038/sj.mp.4001803. [DOI] [PubMed] [Google Scholar]
- Brent DA, Bridge JA. Delinquent accounts: Does delinquency account for suicidal behavior? Journal of Adolescent Health. 2007;40(3):204–205. doi: 10.1016/j.jadohealth.2006.12.014. [DOI] [PubMed] [Google Scholar]
- Brent D, Mann J. Family genetic studies, suicide, and suicidal behavior. American Journal of Medical Genetics. 2005;133:13–24. doi: 10.1002/ajmg.c.30042. [DOI] [PubMed] [Google Scholar]
- Brent D, Melham N. Familial transmission of suicidal behavior. Psychiatriac Clinics of North America. 2008;31:157–177. doi: 10.1016/j.psc.2008.02.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brent DA, Oquendo M, Birmaher B, Greenhill L, Kolko D, Stanley B, Zelazny J, Brodsky B, Firincioqullari S, Ellis SP, Mann JJ. Peripubertal suicide attempts in offspring of suicide attempters with siblings concordant for suicidal behavior. American Journal of Psychiatry. 2003;160(8):1486–1493. doi: 10.1176/appi.ajp.160.8.1486. [DOI] [PubMed] [Google Scholar]
- Brent D, Perper J, Moritz G, Allman C, Friend A, Roth C, Schweers J, Balach L, Baugher M. Psychiatric risk factors for adolescent suicide: A case control study. Journal of the American Academy of Child and Adolescent Psychiatry. 1993;32:521–529. doi: 10.1097/00004583-199305000-00006. [DOI] [PubMed] [Google Scholar]
- Bridge JA, Goldstein TR, Brent DA. Adolescent suicide and suicidal behavior. Journal of Child Psychology and Psychiatry. 2006;47(3–4):372–394. doi: 10.1111/j.1469-7610.2006.01615.x. [DOI] [PubMed] [Google Scholar]
- Brown G, Beck A, Steer R, Grisham J. Risk factors for suicide in psychiatric outpatients: A 20-year prospective study. Journal of Consulting and Clinical Psychology. 2000;68:371–377. [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention (CDC) Web-based Injury Statistics Query and Reporting System (WISQARS) [Online] National Center for Injury Prevention and Control, CDC (producer); 2007. Available from URL: www.cdc.gov/injury/wisqars/index.html. [Google Scholar]
- Centers for Disease Control and Prevention. Youth Risk Behavior Surveillance -United States, 2007. Surveillance Summaries, [June 6, 2008] MMWR. 2008;57(SS-#) [PubMed] [Google Scholar]
- Cho H, Guo G, Iritani BJ, Hallifors DD. Genetic contribution to suicidal behaviors and associated risk factors among adolescents in the U.S Prevention. Science. 2006;7(3):303–311. doi: 10.1007/s11121-006-0042-5. [DOI] [PubMed] [Google Scholar]
- Eaves LJ, Martin NG, Heath AC, Schieken RM, Meyer JM, Silberg J, Neale MC, Corey LA. Age changes in the causes of individual differences in conservatism. Behavioral Genetics. 1997a;27(2):121–124. doi: 10.1023/a:1025633307992. [DOI] [PubMed] [Google Scholar]
- Eaves J, Silberg J, Meyer J, Maes H, Simonoff E, Pickles A, Rutter M, Neale M, Reynolds C, Erickson M, Heath A, Loeber A, Truett K, Hewitt K. Genetics and developmental psychopathology, II: The main effects of genes and environment on behavioral problems in the Virginia Twin Study of Adolescent Behavioral Development. Journal of Child Psychology and Psychiatry. 1997b;38:965–980. doi: 10.1111/j.1469-7610.1997.tb01614.x. [DOI] [PubMed] [Google Scholar]
- Eaves LJ, Hatemi PK, Heath AC, Martin NG. Modeling the biological and cultural inheritance of social and political behavior in twins and families. In: Hatemi PK, McDermott R, editors. Man is by Nature a Political Animal. Chicago, IL: University of Chicago Press; 2010. [Google Scholar]
- Foley D, Goldston D, Costello J, Angold A. Proximal psychiatric risk factors for suicidality in youth: The Great Smoky Mountains study. Archives of General Psychiatry. 2006;63:1017–1024. doi: 10.1001/archpsyc.63.9.1017. [DOI] [PubMed] [Google Scholar]
- Fu Q, Heath A, Bucholz K, Nelson E, Glowinski A, Goldberg J, Lyons M, Tsuang M, Jacob T, True M, Eisen S. A twin study of genetic and environmental influences on suicidality in men. Psychological Medicine. 2002;32:11–24. doi: 10.1017/s0033291701004846. [DOI] [PubMed] [Google Scholar]
- Fulker DW, Baker LA, Bock RD. Estimating components of covariance using LISREL. Data Analyst. 1983;1:5–8. [Google Scholar]
- Glowinski A, Bucholz K, Nelson E, Qiang F, Madden P, Reich W, Heath A. Suicide attempts in an adolescent female twin sample. Journal of the American Academy of Child and Adolescent Psychiatry. 2001;40:1300–1307. doi: 10.1097/00004583-200111000-00010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goldsmith SK, Pellmar TC, Kleinman AM, Bunney W, editors. Reducing suicide: a national imperative. Washington DC: National Academy Press; 2002. [PubMed] [Google Scholar]
- Gould MS, Greenberg T, Velting DM, Shaffer D. Youth suicide risk and preventive interventions: A review of the past 10 years. Journal of the American Academy of Child and Adolescent Psychiatry. 2003;42(4):386–405. doi: 10.1097/01.CHI.0000046821.95464.CF. [DOI] [PubMed] [Google Scholar]
- Harrington RC. Child and adult depression: A test of continuities with data from a family study. British Journal of Psychiatry 1993. 1993;162:627–633. doi: 10.1192/bjp.162.5.627. [DOI] [PubMed] [Google Scholar]
- Haavisto A, Sourander A, Ellila H, Valimaki M, Santalahti P, Helenius H. Suicidal ideation and suicide attempts among child and adolescent psychiatric inpatients in Finland. Journal of Affective Disorders. 2003;23(1–3):211–221. doi: 10.1016/s0165-0327(02)00093-9. [DOI] [PubMed] [Google Scholar]
- Hawton K, Fortune S. Suicidal behavior and deliberate self-harm. In: Rutter M, Bishop D, Pine D, Scott S, Stevenson J, Taylor E, Thapar A, editors. Rutter’s Child and Adolescent Psychiatry. Oxford, UK: Blackwell Publishing Limited; 2008. [Google Scholar]
- Hills A, Cox B, McWilliams L, Sareen J. Suicide attempts and externalizing psychopathology in a nationally representative sample. Comprehensive Psychiatry. 2005;46:334–339. doi: 10.1016/j.comppsych.2005.01.004. [DOI] [PubMed] [Google Scholar]
- Kelly TM, Lynch KG, Donovan JE, Clark DB. Alcohol use disorders and risk factor interactions for adolescent and suicidal ideation attempts. Suicide and Life-Threatening Behaviors. 2001;31(2):181–193. doi: 10.1521/suli.31.2.181.21512. [DOI] [PubMed] [Google Scholar]
- Kendler KS, Neale MC, Kessler RC, Heath AC, Eaves LJ. The lifetime history of major depression in women: The impact of varying definitions of illness. Archives of General Psychiatry. 1993;50:863–870. doi: 10.1001/archpsyc.1993.01820230054003. [DOI] [PubMed] [Google Scholar]
- Kessler R, Berglund P, Borges G, Nock M, Wang P. Trends in suicide ideation, plans, gestures, and attempts in the United States, 1990–1992 to 2001–2003. Journal of the American Medical Association. 2005;293:2487–2495. doi: 10.1001/jama.293.20.2487. [DOI] [PubMed] [Google Scholar]
- Lewinsohn PM, Seeley JR, Hibbard J, Rohde P, Sack WH. Cross-sectional and prospective relationships between physical morbidity and depression in older adolescents. Journal of the American Academy of Child and Adolescent Psychiatry. 1996;35(9):1120–1129. doi: 10.1097/00004583-199609000-00009. [DOI] [PubMed] [Google Scholar]
- Mann J. Neurobiology of suicidal behavior. Nature Reviews Neuroscience. 2003;4:819–828. doi: 10.1038/nrn1220. [DOI] [PubMed] [Google Scholar]
- Martin NG, Eaves LJ. The genetical analysis of covariance structure. Heredity. 1977;38(1):79–95. doi: 10.1038/hdy.1977.9. [DOI] [PubMed] [Google Scholar]
- Neale MC, Boker SM, Xie G, Maes HH. Mx: Statistical Modeling. 7 Box 126 Virginia Commonwealth University, Richmond, VA 23298: Department of Psychiatry; 2006. [Google Scholar]
- Neale MC, Cardon L. NATO ASI Series. Dordrecht: Kluwer Academic Publishers; 1992. Methodology for Genetic Studies of Twins and Families. [Google Scholar]
- O’Carroll PW, Berman AL, Maris RW, Moscicki EK, Tanney BL, Silverman MM. Beyond the Tower of Babel: A nomenclature for suicidology. Suicide and Life-Threatening Behaviors. 1996;26(3):237–252. [PubMed] [Google Scholar]
- Rhee SH, Waldman ID. Genetic and environmental influences on antisocial behavior: a meta-analysis of twin adoption studies. Psychological Bulletin. 2002;128(3):490–529. [PubMed] [Google Scholar]
- Roy A, Segal NL. Suicidal behavior in twins: A replication. Journal of Affective Disorders. 2001;66(1):71–74. doi: 10.1016/s0165-0327(00)00275-5. [DOI] [PubMed] [Google Scholar]
- Roy A, Segal NL, Sarchiapone M. Attempted suicide among living co-twins of twin suicide victims. American Journal of Psychiatry. 1995;152(7):1075–1076. doi: 10.1176/ajp.152.7.1075. [DOI] [PubMed] [Google Scholar]
- Rueter M, Holm K, McGeorge C, Conger R. Adolescent suicidal ideation subgroups and their association with suicidal plans and attempts in young adulthood. Suicide and Life-Threatening Behaviors. 2008;38:564–575. doi: 10.1521/suli.2008.38.5.564. [DOI] [PubMed] [Google Scholar]
- Silberg JL, Pickles A, Rutter M, Hewitt JK, Simonoff E, Maes H, Carbonneau R, Murrelle L, Foley DL, Eaves LJ. The influence of genetic factors and life stress on depression in adolescent girls. Archives of General Psychiatry. 1999;56:225–232. doi: 10.1001/archpsyc.56.3.225. [DOI] [PubMed] [Google Scholar]
- Silberg JL, Maes H, Eaves LJ. Genetic and environmental influences on the transmission of parental depression to children’s depression and conduct disturbance: An extended children of twins study. Journal of Child Psychology and Psychiatry. 2010;51(6):734–744. doi: 10.1111/j.1469-7610.2010.02205.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Silberg J, Rutter M, Maes HH, Eaves L. Etiological heterogeneity in the development of antisocial behavior: The Virginia twin study of adolescent behavioral development and the young adult follow-up. Psychological Medicine. 2007;37:1193–202. doi: 10.1017/S0033291707000293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sullivan PF, Eaves LJ. Evaluation of analyses of univariate discret twin data. Behavior Genetics. 2002;32 (3):221–227. doi: 10.1023/a:1016025229858. [DOI] [PubMed] [Google Scholar]
- Spirito A, Esposito-Smythers C. Attempted and completed suicide in adolescence. Annual Review of Clinical Psychology. 2006;2:237–266. doi: 10.1146/annurev.clinpsy.2.022305.095323. [DOI] [PubMed] [Google Scholar]
- Statham DJ, Heath AC, Madden PA, Bucholz KK, Bierut L, Dinwiddie SH, Slutske WS, Dunne MP, Martin NG. Suicidal behavior: An epidemiological and genetic study. Psychological Medicine. 1998;28(4):839–855. doi: 10.1017/s0033291798006916. [DOI] [PubMed] [Google Scholar]
- Thompson M, Kuruwita C, Foster M. Transitions in suicide risk in a nationally representative sample of adolescents. Journal of Adolescent Health. 2009;44:458–463. doi: 10.1016/j.jadohealth.2008.10.138. [DOI] [PubMed] [Google Scholar]
- Voracek M, Loibl LM. Genetics of suicide: a systematic review of twin studies. Wien Klin Wochenschr. 2007;119:463–475. doi: 10.1007/s00508-007-0823-2. [DOI] [PubMed] [Google Scholar]