

Abstract
BACKGROUND:
Anorexia nervosa (AN) is a difficult-to-treat psychosomatic disease. Very few cases of acute liver failure associated with AN have been described. We describe one patient who was affected by AN and presented high level increase of serum liver enzymes, along with sever thrombocytopenia. Then, we discuss the possible etiopathogenic factors.
METHODS:
A 14-year-old boy with AN was admitted in the pediatric psychiatric emergency department of Alzahra Hospital with impaired electrolyte levels, bradycardia, hypotension, liver dysfunction, and thrombocytopenia.
RESULTS:
A ten-time increase in liver enzymes and thrombocytopenia were observed on admission. After two months of treatment, the levels were within the normal range.
CONCLUSIONS:
Improvement of initial clinical symptoms and recovery of liver enzymes and thrombocytopenia after the treatment suggested that liver dysfunction and thrombocytopenia may be observed in AN patients and should be taken care of by physicians.
KEYWORDS: Anorexia Nervosa, Liver Dysfunction, Thrombocytopenia
Anorexia nervosa (AN) is a difficult-to-treat psychosomatic disease.1 Due to malnutrition, various physical problems have been reported to occur in patients with AN including diminished bone mineral density, increased QT interval, cardiomyopathy, and liver dysfunction. Thrombocytopenia is also known to occur in cases of low body weight accompanied by AN.2,3
Several studies have described an increase in serum liver enzyme in severely malnourished patients affected by AN,4–6 as well as during the refeeding phase of therapeutic intervention.7 In the case of anorectic patients, the slight to moderate increase in liver enzyme is expected to reflect a fatty liver that is typical of several protein-energy malnutrition states.8,9 Nevertheless, very few cases of acute liver failure associated with AN have been described.10,11 Aside from malnutrition, several pathogenetic factors have been considered to justify the shift from normal to slightly increased serum liver enzymes. These factors include acute complications such as hepatotropic viruses (hepatitis A and B, cytomegalovirus, Epstein-barr virus), acute liver hypoperfusion, hypothermia, alcohol, cannabis, and cocaine abuse, and hepatotoxic drugs (paroxetine, amphetamines, benzodiazepines, methadone, opiates, etc.).12 In this study, we describe a patient who was affected by AN and presented high level increase in serum liver enzymes and sever thrombocytopenia. Then we discuss the possible etiopathogenic factors and describe our medical intervention.
Case presentation
A 14-year-old boy with an 8-month history of AN referred to our outpatient clinic (Department of Pediatrics, Alzahra Hospital). Because of his physical condition (weight loss, bradycardia, imbalanced electrolytes, hypothermia, hypotension, and lung and liver dysfunction) we decided to hospitalize him (Figure 1).
Figure 1.

A male patient with anorexia nervosa.
On admission to the psychiatric unit, his body weight and body mass index (BMI) were 31 kg and 13.2, respectively. In addition, his liver enzymes were high, and his platelet decreased as shown in Table 1. Other causes of acute liver dysfunction such as hepatotoxic drugs, alcohol, cocaine and viral hepatotoxic diseases were evaluated and then ruled out.
Table 1.
Changes in liver enzymes and platelet numbers during the hospitalization period.
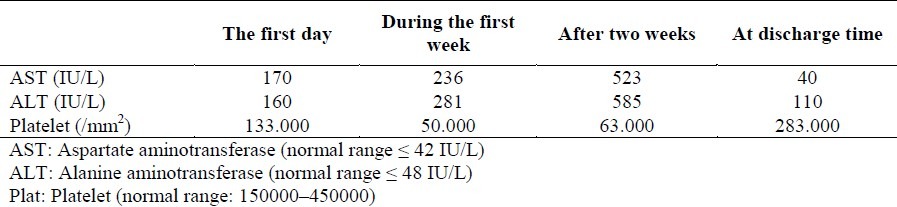
We started to treat the patient with conservative management including stabilizing electrolytes by serum therapy and nourishment using a high calorie diet. A marked decrease in serum transaminase and an increase in platelet count were observed with a gradual normalization of all the biochemical parameters within one months of hospitalization. He started eating and his electrolytes got balanced and his family became happy about his recovery. Therefore, he was discharged after one months of hospitalization and successfully continued his rehabilitation program on an outpatient basis.
Discussion
This was one of the uncommon cases of AN with a high level increase (10 times more) of liver enzymes and sever thrombocytopenia. Minor degrees of liver injury have been reported in up to 40% of patients with AN.13 Although the mechanism of liver injury in AN has thought to be due to protein-calorie malnutrition of the kwashiorkor type accompanied with fatty changes, this has not been rigorously demonstrated and the mechanism is still unknown.13,14 In AN, malnutrition has been reported to cause thrombocytopenia along with liver dysfunction.2
One report has described temporal changes in liver enzyme levels, platelet count, and thyroid peroxidase (TPO) levels in a patient with AN.3 Acute liver failure with a massive increase of serum liver enzyme may be a sever, though relatively uncommon, complication caused by severe malnutrition such as that secondary to AN.4–6 As reported in the literature, serum transaminases do not reach such high values during the refeeding syndrome.7 To avoid complications of refeeding syndromes,7 nutritional rehabilitation is started with a low-energy oral and parental nutrition (25 kcal/kg body weight).
Therefore, follow up of serum liver enzymes should be part of our evaluation to prevent the uncommon but serious risk of acute liver failure. We should also examine the patient for thrombocytopenia.
Conclusion
Our case report showed an AN patient with increased level of liver enzymes about 10 times more than normal range, as well as severe thrombocytopenia, which is uncommon. Therefore, it is concluded that physicians should be aware of high level increase of liver enzymes and severe thrombocytopenia which may occur in AN.
Authors’ Contributions
MK introduced the case and managed the process. SL found pediatric references and provided information on anorexia nervosa. MK provided up-to-date data regarding the case.
Footnotes
Conflict of Interests Authors have no conflict of interests.
References
- 1.Sakada M, Tanaka A, Ohta D, Takayanagi M, Kodama T, Suzuki K, et al. Severe steatosis resulted from anorexia nervosa leading to fatal hepatic failure. J Gastroenterol. 2006;41(7):714–5. doi: 10.1007/s00535-006-1845-7. [DOI] [PubMed] [Google Scholar]
- 2.Becker AE, Grinspoon SK, Klibanski A, Herzog DB. Eating disorders. N Engl J Med. 1999;340(14):1092–8. doi: 10.1056/NEJM199904083401407. [DOI] [PubMed] [Google Scholar]
- 3.Yoshiuchi K, Takimoto Y, Moriya J, Inada S, Akabayashi A. Thrombopoietin and thrombocytopenia in anorexia nervosa with severe liver dysfunction. Int J Eat Disord. 2010;43(7):675–7. doi: 10.1002/eat.20762. [DOI] [PubMed] [Google Scholar]
- 4.Umeki S. Biochemical abnormalities of the serum in anorexia nervosa. J Nerv Ment Dis. 1988;176(8):503–6. doi: 10.1097/00005053-198808000-00009. [DOI] [PubMed] [Google Scholar]
- 5.Milner MR, McAnarney ER, Klish WJ. Metabolic abnormalities in adolescent patients with anorexia nervosa. J Adolesc Health Care. 1985;6(3):191–5. doi: 10.1016/s0197-0070(85)80016-4. [DOI] [PubMed] [Google Scholar]
- 6.Mickley D, Greenfeld D, Quinlan DM, Roloff P, Zwas F. Abnormal liver enzymes in outpatients with eating disorders. Int J Eat Disord. 1996;20(3):325–9. doi: 10.1002/(SICI)1098-108X(199611)20:3<325::AID-EAT13>3.0.CO;2-Z. [DOI] [PubMed] [Google Scholar]
- 7.Ozawa Y, Shimizu T, Shishiba Y. Elevation of serum aminotransferase as a sign of multiorgan-disorders in severely emaciated anorexia nervosa. Intern Med. 1998;37(1):32–9. doi: 10.2169/internalmedicine.37.32. [DOI] [PubMed] [Google Scholar]
- 8.Waterlow SC, Tomkins AM, Grantham SM. Causes of oedema and its relation to kwashiorkor. In: Waterlow SC, editor. Protein Energy Malnutrition. London: Edward Arnold; 1992. pp. 146–63. [Google Scholar]
- 9.Fuhrman MP, Charney P, Mueller CM. Hepatic proteins and nutrition assessment. J Am Diet Assoc. 2004;104(8):1258–64. doi: 10.1016/j.jada.2004.05.213. [DOI] [PubMed] [Google Scholar]
- 10.Rivera-Nieves J, Kozaiwa K, Parrish CR, Iezzoni J, Berg CL. Marked transaminase elevation in anorexia nervosa. Dig Dis Sci. 2000;45(10):1959–63. doi: 10.1023/a:1005642601144. [DOI] [PubMed] [Google Scholar]
- 11.Harada N, Imanish H, Iwasaki M, Ohno T, Tukada K, Kimura H. A patient with anorexia nervosa and severe hepatic dysfunction. Nippon Naika Gakkai Zasshi. 1981;70:1458–62. [Google Scholar]
- 12.Di PL, Lion A, Milazzo D, Caregaro L. Acute liver damage in anorexia nervosa. Int J Eat Disord. 2004;36(1):114–7. doi: 10.1002/eat.20002. [DOI] [PubMed] [Google Scholar]
- 13.Mine T, Ogata E, Kumano H, Kuboki T, Suematsu H. Liver dysfunction in anorexia nervosa. 1991 [Google Scholar]
- 14.Sharp CW, Freeman CP. The medical complications of anorexia nervosa. Br J Psychiatry. 1993;162:452–62. doi: 10.1192/bjp.162.4.452. [DOI] [PubMed] [Google Scholar]