

Abstract
BACKGROUND:
Pain after knee surgery, if not relieved, it would lead to a more severe and prolonged pain that can delay the patients recovery and rehabilitation. The effect of pain relief by some drugs after intra-articular injection has been shown. This study compared the effect of intra-articular injection of opioids (morphine, pethidine, methadone, and tramadol) on postoperative relieving pain after arthroscopic anterior cruciate ligament (ACL) reconstruction.
METHODS:
150 candidate patients for knee arthroscopic ACL reconstruction were randomly enrolled into five groups. At the end of the procedure, all patients in each group received a joint injection solution including 9.5 millimeters bupivacaine with 1:200,000 epinephrine. The remaining 0.5 milliliters of syringe capacity was filled with one of the five solutions listed below: methadone group I: 5 mg methadone, morphine group II: 5 mg morphine, pethidine group III: 37.5 mg pethidine, tramadol group IV: 100 mg Tramadol, and control group V: 0.5 ml normal saline. Afterwards, any drug further administered to the patients based on need was recorded, and the morphine equivalent for all drugs was calculated. Patients need to narcotic drugs during the first twelve hours of hospitalization and pain scores were recorded. After data gathering, they were analyzed by SPSS 16 software with chi-Square, Kruskal-Wallis and ANOVA statistical tests.
RESULTS:
The highest and the lowest significant pain intensity were seen in placebo and morphine groups, respectively, in the first, second and third 4 hours after surgery. There were significant differences among the groups for need to analgesics. In other words, placebo group needed the highest dosage of analgesics and morphine and methadone groups needed the lowest dosage of analgesics. Morphine and methadone groups had maximum and minimum response to pain, respectively, in the first, second and third 4 hours after surgery.
CONCLUSIONS:
Administering 5 mg intra-articular morphine after arthroscopic ACL reconstruction is a valuable choice and is recommended to be added to other local anesthetics administrated drugs after this procedure.
KEYWORDS: Knee Arthroscopic, Morphine, Pethidine, Methadone, Tramadol, Intra-Articular Injection
Pain related problems are one of the important issues in medicine and pain after surgery is an unfavorable experience in human being. One goal is to relieve the patients’ pain. Acute pain after surgery is one of the most common, but important kinds of pain1 and arthroscopic anterior cruciate ligament (ACL) reconstruction is one of the most common surgical procedures that is done daily in all over the world and is accompanied by pain which can be the most important cause in preventing patients’ rehabilitation.2 Thus, finding the most effective treatment is very important. Some common examples of complications from pain stimulation after surgery are thromboembolism, myocardial ischemia, atelectasis, etc.3 There are several different methods for treating patient's pain after surgery and opioids is one of the most common used drugs for reduction of pain.4–6
Morphine and other Opioids are the most effective forms of medicine that are used in relieving pain, but over dosage of these drugs can lead to symptoms such as addiction, respiratory arrest particularly in children and increased drug tolerance.7 Today, one of the best recommended methods of relieving pain is the administration of a combination of drugs (multimodal analgesia) that includes synergism effects of multiple drugs with a minimum administration dose.8 Numerous studies showed analgesic effects of only opioids or combination with other local anesthetic drugs in arthroscopic ACL reconstruction.9,10 Morphine, methadone and pethidine were used as intra-articular injections.8,10–12 Intra-articular morphine dosage was reported in different ranges.5,6,11,12 Morphine is the most common used analgesic agents after major surgery and its half life is about 2 hours. If it used intra-articularly, its analgesic effects would last for 24 hours. Methadone is a synthetic long acting anesthetic agent with high activity on opioid receptors and its half-life is about 35 hours and highly linked to plasma protein. After intra-articular injection of methadone, its analgesic effects last for 24 hours.5 Pethidine is an anesthetic opioid drug, its half-life is about 4 hours, has lower affinity to protein linkage and higher cause of convulsion than morphine. After intra-articular injection of pethidine, the duration of anesthetic effect lasts about 12 hours and the patient's need is diminished.6 Tramadol is an analgesic drug which is weaker than morphine and has higher side effects than morphine. Its half-life is about 6-7.5 hours. Its analgesic effect lasts about 6 hours9 and it has not been used as an intra-articular injection in any previous research. Bupivacaine is an anesthetic agent that can be used sometimes with epinephrine and its effects last for 4-6 hours.6
There is not any research about comparison of the effects of intra-articular injection of morphine, pethidine, methadone and tramadol. The aim of this study was to compare the effects of intra-articular injection of morphine, pethidine, methadone and tramadol with bupivacaine in pain relief after ACL reconstruction and control group (normal saline).
Methods
This study was a controlled double blind randomized clinical trial based on random number table. All patients that needed arthroscopic ACL reconstruction from 2006 to 2009 and referred to the university hospital were enrolled in this study. All patients signed an informed consent form after approval of ethical committee (NO: 3-2-58, 3-2-2006) and registered in IRCT (NO: IRCT201106102341N4). Of 178 patients 28 were excluded since they did not take part in follow-up because came from another town or used intra-operation tourniquet that intervened with the intensity of pain due to ischemic muscles during operation. The remaining 150 patients were entered the study and classified into one of the 5 groups, randomly. The groups were named morphine group, methadone group, pethidine group, tramadol group, and control group (normal saline group). 30 patients were included in each group.
Inclusion criteria were as follows:
-
1-
ASAI or ASAII class of American Society of Anesthesiologist
-
2-
Age of 18-55years
-
3-
Tolerance to general anesthesia and signed the informed consent
Exclusion criteria were as follows:
-
1-
History of allergic reaction to administered drugs
-
2-
History of drug abuse
-
3-
History of chronic pain
-
4-
History of pregnancy or breastfeeding
-
5-
Need for drainage tube after surgery
-
6-
Consumption of MAOI agent that can lead to meperidine syndrome5.
-
7-
Use of preoperative opioids or other analgesic drugs
All of the patients had a standard anesthesia in four hour intervals after surgery by administration of thiopental sodium 5 mg/kg for induction of anesthesia followed by 60% air/oxygen (O2) with isoflurane 1% to 2% end-tidal volume. For maintenance anesthesia they received fentanyl 3 mcg/kg IV. After induction and based on Visual Analogue Scale (VAS),13 pain intensity and level of need and response to analgesics were measured and recorded. Need and response to analgesics were evaluated by VAS.14
When required analgesics each group received 0.5% bupivacaine with 1:200,000 epinephrine and analgesics as below: morphine group 5 mg morphine, methadone group 5 mg methadone, pethidine group 37.5 mg pethidine, and tramadol group 100 mg tramadol.
Control group received 0.5 ml normal saline.6
The contents of syringe were unknown for surgeon, anesthesiologist and patients. They were prepared by a pharmacist and each syringe had a unique number that only after data collection and analysis, it was distinguished. After surgery, administered pain killers were intravenous morphine and codeine tablet based on need of patients and when VAS was more than 3. 10 mg morphine sulfate is equivalent to 10 mg methadone hydrochloride, 100 mg pethidine hydrochloride, 100 mg tramadol and 200 mg codeine.5,6 Patients’ needs to analgesics were recorded every 4 hours using VAS by another surgeon. All of the patients were discharged the day after arthroscopic surgery with administration of codeine tablet. The amount of pain killers given to each patient was recorded for 7 days. All patients had undergone a similar physical therapy. After data was collected, they were analyzed by SPSS 16 software with chi-square, Kruskal – Wallis and ANOVA statistical tests. When ANOVA test showed significant differences among the groups, Tukey test was used for showing the differences. 7 milligram difference in morphine equivalent and 8 milligram difference in standard deviation among the groups assumed significant and meaningful difference. p - value < 0.05 was considered significant.
Results
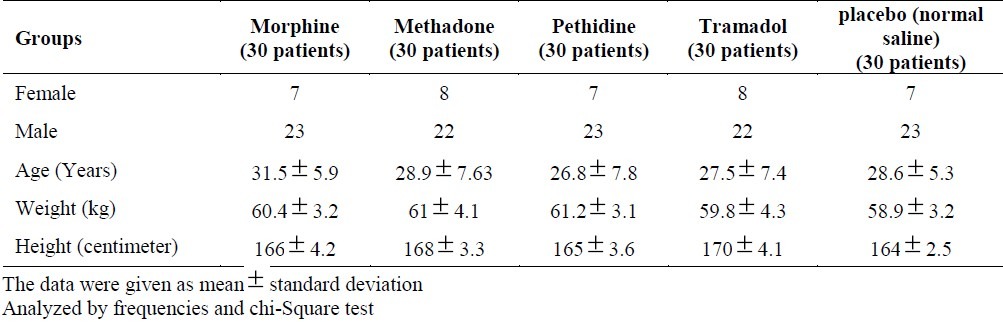
The age range was 18 to 55 years old with average of 28.7±7 years old. Morphine group had greater average age than other groups (p > 0.67). 37 (24.6 Percent) patients were female. There was no difference between sex ratios among the groups (p > 0.71). Demographic data results are presented in Table 1.
Table 1.
Demographic data
The needs to analgesics were measured after arthroscopic ACL reconstruction surgery in five groups and the results are presented in Table 2.
Table 2.
Comparison of average need to analgesics after arthroscopic ACL reconstruction in the study groups
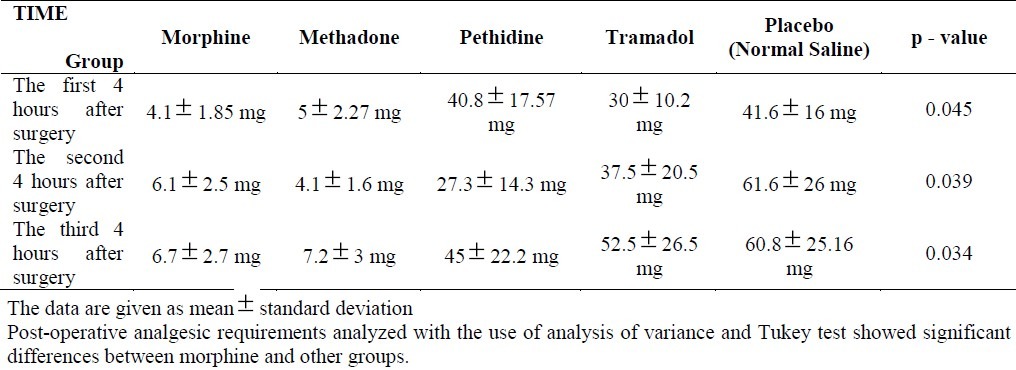
In comparison of the mean and standard deviation of the need to analgesics after arthroscopic surgery in 5 groups, Kruskal–Wallis, ANOVA and Tukey statistical tests were used and there were significant differences among the groups for need to analgesics. In other words, placebo group needed the highest dosage of analgesics and morphine and methadone groups needed the lowest dosage of analgesics. Postoperative pain scores based on the VAS (visual analogue scale) in three different times after operation (the first, the second and the third 4 hours after surgery) in five groups were measured and shown in Table 3.
Table 3.
Comparison of pain after arthroscopic ACL reconstruction surgery in the study groups based on the VAS scale
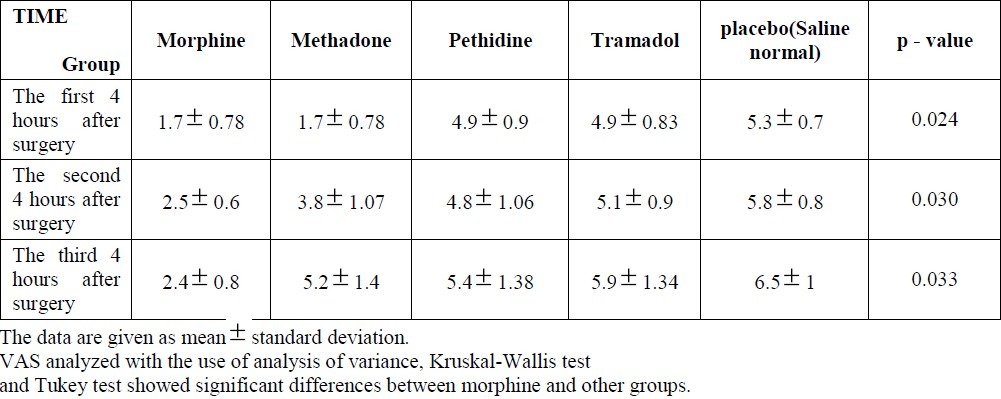
ANOVA and Kruskal-Wallis test showed significant difference in intensity of pain among 5 groups. Tukey test showed the highest and the lowest significant pain intensity in placebo and morphine groups, respectively, in the first, second and third 4 hours after surgery. Responses of pain to analgesics in three different times in 5 groups were measured and are presented in Table 4.
Table 4.
Comparison of the different opioids consumption In 5 groups after arthroscopic ACL reconstruction surgery
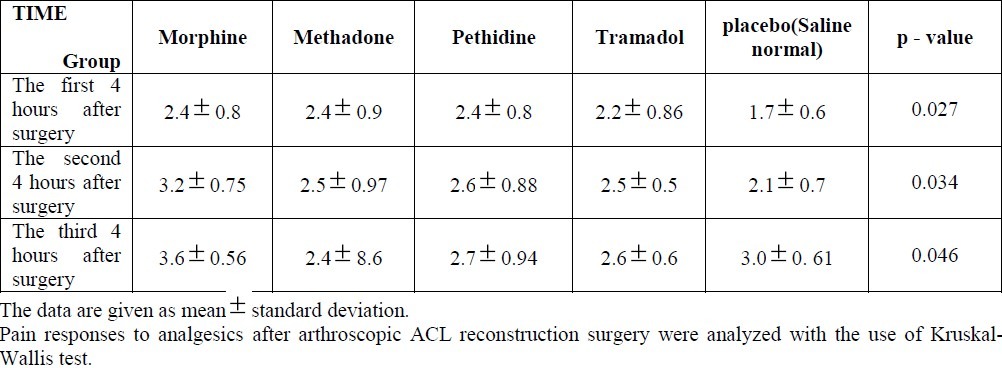
Kruskal-Wallis test showed significant differences in pain response to analgesics among five groups. Tukey test showed that morphine and methadone groups had maximum and minimum response to pain, respectively, in the first, second and third 4 hours after surgery.
Discussion
This study was a clinical trial performed to compare the effects of intra-articular injection of morphine, methadone, pethidine and tramadol with normal saline (placebo) after arthroscopic ACL reconstruction surgery. Many studies that have been done in the past showed their analgesics effects in reducing pain after surgery. For example, David J. Stewart in 2005 showed that analgesic effect on intra-articular injection reduced pain after primary arthroscopic ACL reconstruction ligament. In his study, 25 patients received 5 mg methadone, 25 patients received 5 mg morphine and 15 patients received 5 mg saline solution (control group) and the results showed that morphine group had a less pain scale and needed less administration of analgesics in the first 24 hours after surgery, but there was not a significance difference between the methadone and the control groups.15 Results of our study were similar to that of a recent study occurred in 2011 by Lykoudi on patients after knee arthroscopic surgery, which compared intra-articular morphine and control group. The results showed that pain was less severe in the group that received morphine compared with the control group, 24 hours after surgery.16 In another study by Kligman in 2004 that was conducted on 50 patients, the effect of intra-articular morphine injection was compared with intrasynovial injection after knee arthroscopy meniscectomy. In that study, 25 patients received 1 mg intrasynovial morphine injection and the other 25 patients received 1 mg intra-articular morphine injection after arthroscopy. The results showed significant differences in pain scale in the first 12-24 hours after arthroscopy in both groups, but there was less pain in 12-24 hours after arthroscopy in the group that received intrasynovial morphine.17 Intrasynovial injection, despite its more effectiveness than intra-articular morphine in meniscectomy is not effective in ACL reconstruction. Another study on the effect of intra-articular morphine injection after knee surgery to relieve the pain was conducted and evaluated by Kalso E. in 2002 on 1,500 patients. In that study, 900 patients after knee surgery, received 5 mg intra-articular morphine and 600 patients as control group received 5 mg saline solution. The results showed that morphine group had less pain than the control group in the first 24 hours after surgery.18 The results of this study are similar to that of a recent study. In most studies, to review of the effects of analgesics for reduction of postoperative pain, especially knee surgery, only the effect of morphine were evaluated, and other analgesics were not evaluated. Other analgesics than morphine may have more or less similar effectiveness and were more accessible than morphine. Intra-articular injection of opioids had long term pain relieving effects and this period of pain relieve is different and is variable between 8 to 24 hours for different opioids.16 Opioid receptors have been proved to be in central and peripheral nerves. Two responsible mechanisms for local administration of analgesic opioids are removal of the neural sheath in the ends of nerves that allow easy access to opioids in the neural receptors and inflammation that causes activation of the inactive opioids receptor.19 Both of these mechanisms after knee surgery are responsible for the analgesic opioids function. In addition, studies have shown that intra-articular opioid drugs compared to intravenous injection, lead to better pain relief and the patient's need to analgesics would be reduced in this method.19–22. Another factor that can influence the efficacy is dosage. High-dose opioids affect the central nervous system. In a recent study, 5 mg dosage of morphine and morphine equivalent for other analgesics were considered because the effects of this dosage of analgesics on CNS were negligible. The significant and far from expected results of the recent study showed lack of significant pain relief of methadone and pethidine. Although the two mentioned drugs have function similar to morphine and their pain relief effect is like morphine in stimulating opioids receptors. One of the possible reasons for differences between morphine and other opioids in this study is the differences between pharmacokinetics properties of them. Morphine molecules can probably reach to its peripheral receptor in a low concentration and easy way than two other drugs.23 Tramadol is more effective for mild to moderate pain. Also, 5 mg equivalent dosage of morphine is high and thus, a lower dosage of this drug is tolerated by the patient. However, it is less efficient than morphine. However, 5 mg methadone did not show any complication in this study in respect to morphine and equivalent dosage of other analgesics but was less effective than morphine, and as it appears from the result, this dosage of intra-articular injection opioids in human would be safe. This study showed that 5 mg dosage of morphine for reducing the need to analgesics was very useful, but this effect was significant only in the first 12-24 hours after surgery, and perhaps was due to its significant improvement of inflammatory reactions after this period. Results of this study about methadone were less than predications. While it was expected to have at least a morphine equivalent or more effect, this effect was probably due to relationship between maximum dosages of methadone with pain relieving effect of morphine.
Equivalent dosage of sedative effects of pethidine for pain relief was not sufficient after knee arthroscopic surgery and it needs more evaluation in future studies. The effect of equivalent dosage of tramadol was not significant in pain relief compared with other analgesics.
Conclusion
Considering the results, unlike methadone, pethidine and tramadol did not have significant long-term efficacy on pain relief after knee surgery. 5 mg intra-articular morphine was preferable, safe and useful and its use with bupivacaine is recommended for pain relief after knee surgery.
Authors’ Contributions
HRA has planned the study and finalized it, and also did the statistical analysis and prepared the first and final version of manuscript for publication; SAM provided assistance in the design of the study. All authors read and approved the final manuscript.
Acknowledgement
The authors would like gratefully to thank Imam Khomeini Trauma Research Center of Ahvaz Jundishapur University of Medical Sciences.
Footnotes
Conflict of Interests Authors have no conflict of interests.
References
- 1.Inturrisi CE, Lipman AG. Opioid Analgesics. In: Fishman S, Ballantyne J, Ballantyne JC, Rathmell JP, Rathmell JJ, editors. Bonica's Management of Pain. 4th ed. Philadelphia: Lippincott Williams & Wilkins; 2009. pp. 1173–85. [Google Scholar]
- 2.Miller RD, Eriksson LI, Fleisher LA, Wiener-Kronish JP, Young WL. London: Churchill Livingstone/Elsevier; 2010. Miller's anesthesia; pp. 769–83. [Google Scholar]
- 3.Kehlet H, Holte K. Effect of postoperative analgesia on surgical outcome. Br J Anaesth. 2001;87(1):62–72. doi: 10.1093/bja/87.1.62. [DOI] [PubMed] [Google Scholar]
- 4.McQuay H. Opioids in pain management. Lancet. 1999;353(9171):2229–32. doi: 10.1016/S0140-6736(99)03528-X. [DOI] [PubMed] [Google Scholar]
- 5.Brunton LL, Blumenthal D, Buxton L. 1st ed. Philadelphia: McGraw-Hill; 2007. Goodman and Gilman's manual of pharmacology and therapeutics; pp. 349–371. [Google Scholar]
- 6.Schumacher MA, Basbaum AI, Way WL. Opioid Analgesics and Antagonists. In: Katzung BG, editor. Basic & Clinical Pharmacology. 9th ed. New York: McGraw-Hill Medical McGraw-Hill Medical; 2005. pp. 497–9. [Google Scholar]
- 7.Benyamin R, Trescot AM, Datta S, Buenaventura R, Adlaka R, Sehgal N, et al. Opioid complications and side effects. Pain Physician. 2008;11(2 Suppl):S105–S120. [PubMed] [Google Scholar]
- 8.Rosaeg OP, Krepski B, Cicutti N, Dennehy KC, Lui AC, Johnson DH. Effect of preemptive multimodal analgesia for arthroscopic knee ligament repair. Reg Anesth Pain Med. 2001;26(2):125–30. doi: 10.1053/rapm.2001.20982. [DOI] [PubMed] [Google Scholar]
- 9.Ayoglu H, Altunkaya H, Bayar A, Turan IO, Ozer Y, Ege A. The effect of intra-articular combinations of tramadol and ropivacaine with ketamine on postoperative pain after arthroscopic meniscectomy. Arch Orthop Trauma Surg. 2010;130(3):307–12. doi: 10.1007/s00402-008-0770-z. [DOI] [PubMed] [Google Scholar]
- 10.Akinci SB, Saricaoglu F, Atay A, Doral MN, Kanbak M. Analgesic effect of intra-articular tramadol compared to morphine after arthroscopic knee surgery. Can J Anaesth. 2003;50(4):423–4. doi: 10.1007/BF03021046. [DOI] [PubMed] [Google Scholar]
- 11.Drosos GI, Vlachonikolis IG, Papoutsidakis AN, Gavalas NS, Anthopoulos G. Intra-articular morphine and postoperative analgesia after knee arthroscopy. Knee. 2002;9(4):335–40. doi: 10.1016/s0968-0160(02)00074-1. [DOI] [PubMed] [Google Scholar]
- 12.Musil D, Sadovsky P, Stehlik J. [Intra-articular analgesia after anterior cruciate ligament reconstruction] Acta Chir Orthop Traumatol Cech. 2007;74(3):182–8. [PubMed] [Google Scholar]
- 13.Turk DC, Melzack R. 2nd ed. New York: Guilford Press; 2001. Handbook of pain assessment; pp. 295–315. [Google Scholar]
- 14.Apfelbaum JL, Chen C, Mehta SS, Gan TJ. Postoperative pain experience: results from a national survey suggest postoperative pain continues to be undermanaged. Anesth Analg. 2003;97(2):534–40. doi: 10.1213/01.ANE.0000068822.10113.9E. table. [DOI] [PubMed] [Google Scholar]
- 15.Stewart DJ, Lambert EW, Stack KM, Pellegrini J, Unger DV, Hood RJ. The effect of intra-articular methadone on postoperative pain following anterior cruciate ligament reconstruction. J Bone Joint Surg Am. 2005;87(1):140–4. doi: 10.2106/JBJS.D.01912. [DOI] [PubMed] [Google Scholar]
- 16.Lykoudi I, Kottis G, Nikolaou VS, Setaki P, Fassoulaki A, Efstathopoulos N. Intra-articular morphine enhances analgesic efficacy of ropivacaine for knee arthroscopy in ambulatory patients. Orthopedics. 2011;34(2):91. doi: 10.3928/01477447-20101221-12. [DOI] [PubMed] [Google Scholar]
- 17.Kligman M, Bruskin A, Sckliamser J, Vered R, Roffman M. Intra-synovial, compared to intra-articular morphine provides better pain relief following knee arthroscopy menisectomy. Can J Anaesth. 2002;49(4):380–3. doi: 10.1007/BF03017326. [DOI] [PubMed] [Google Scholar]
- 18.Kalso E, Smith L, McQuay HJ, Andrew MR. No pain, no gain: clinical excellence and scientific rigour--lessons learned from IA morphine. Pain. 2002;98(3):269–75. doi: 10.1016/S0304-3959(02)00019-2. [DOI] [PubMed] [Google Scholar]
- 19.Gupta A, Bodin L, Holmstrom B, Berggren L. A systematic review of the peripheral analgesic effects of intraarticular morphine. Anesth Analg. 2001;93(3):761–70. doi: 10.1097/00000539-200109000-00042. [DOI] [PubMed] [Google Scholar]
- 20.Brandsson S, Karlsson J, Morberg P, Rydgren B, Eriksson BI, Hedner T. Intra-articular morphine after arthroscopic ACL reconstruction: a double-blind placebo-controlled study of 40 patients. Acta Orthop Scand. 2000;71(3):280–5. doi: 10.1080/000164700317411889. [DOI] [PubMed] [Google Scholar]
- 21.Shang AB, Gan TJ. Optimising postoperative pain management in the ambulatory patient. Drugs. 2003;63(9):855–67. doi: 10.2165/00003495-200363090-00002. [DOI] [PubMed] [Google Scholar]
- 22.Vintar N, Rawal N, Veselko M. Intra-articular patient-controlled regional anesthesia after arthroscopically assisted anterior cruciate ligament reconstruction: ropivacaine/morphine/ketorolac versus ropivacaine/morphine. Anesth Analg. 2005;101(2):573–8. doi: 10.1213/01.ANE.0000158608.27411.A9. [DOI] [PubMed] [Google Scholar]
- 23.Arti HR, Abrishamkar S, Rafeian M. Comparative study on intra-articular narcotics in pain relieve of knee after arthroscopic meniscectomy. Hormozgan Medical Journal. 2005;4(9):241–5. [Google Scholar]