

Abstract
BACKGROUND:
Attention deficit hyperactivity disorder (ADHD) is the most common childhood behavioral disorder causing hyperactivity, attention deficit and education decline among students. The teachers may not have enough knowledge about this disorder and are in a real need in this field. Teachers’ education is one of the ways to get knowledge about this disorder. Nowadays, finding a way like a short term nonattendance education method is highly in demand. Therefore, the aim of the study was to compare effectiveness of nonattendance and workshop education of primary school teachers on their knowledge, attitude, and function towards ADHD students.
METHODS:
Sixty seven primary school teachers from the First Districts of Education Department of Isfahan were randomly selected and put into two groups of workshop education (33 participants) and nonattendance education (34 participants). At first, both groups filled demographic date questionnaires and then, were given a pretest. Post tests were given after a two day education in workshop group and after ten days in nonattendance group who had studied the related booklet. Finally, the mean post test scores of knowledge, attitude and knowledge of function were compared between the two groups using ANCOVA analysis.
RESULTS:
After intervention, the mean scores of knowledge between the two groups was not significantly different whereas the mean scores of attitude and the mean scores of knowledge of function showed a significant difference between the two groups.
CONCLUSIONS:
Nonattendance education was as effective as workshop education in promotion of teachers’ knowledge, but workshop education was more effective in attitude change and promotion of teachers’ knowledge of function about dealing with ADHD students.
KEYWORDS: Attention Deficit Hyperactivity Disorder, Teacher Education, Primary School Teachers, Knowledge, Attitude, Knowledge of Function
ADHD is the most prevalent behavioral disorder diagnosed among children in outpatient clinics.1–3 About 5-12% of children are worldwide involved in ADHD.2
These children, based on definition, face more problems concerning attention, impulse control_and hyperactivity compared to their peers at the same age and sex.3 These signs are accompanied with some deficits in their social function and education as well as their occupation stability.1–4
ADHD related behaviors may be firstly observed in the classroom as causing most of the problems.5
On the other hand, since these children spend most of their times in classrooms or educational environments, the teachers are the first ones who refer the children for ADHD evaluation.6 Teachers report that they are not prepared enough to work with this group of students. Just those teachers who have experience in working with these students or already have been educated prefer to make educational changes that fit these students’ needs.7 Teachers’ enough knowledge and positive attitude towards this disorder is important and crucial to prevent labeling these students.8,9 So, teachers’ education and their on time detection of this disorder can reduce the time these students undergo the appropriate treatment.10,11
There are various methods for continuing education. Two current ones are workshop and nonattendance education. In a study comparing continuing education of ADHD, a change was seen in teachers’ attitude toward students with ADHD as well as their self-confidence to teach them and their ability in making necessary changes in classrooms after three months.12 A study, conducted in Shiraz, showed low knowledge and negative attitude of teachers toward ADHD.13
Another study in Isfahan showed that holding educational workshops was an effective way to increase the mean scores in teachers’ knowledge, attitude and knowledge of function.14 In a more recent study in Isfahan, there was no difference between the therapeutic effect of semi-attendance and attendance education in cognitive behavioral therapy (CBT) of the teenagers suffering from anxiety disorders so that both methods decreased anxiety signs with the same level. With regard to the fact that treatment lasted for 4 sessions in semi-attendance method versus 8 sessions in attendance method in the latter study, this method was possibly more time cost effective, compared to attendance method.15 Therefore, the aim of the study was to compare effectiveness of nonattendance and workshop education of primary school teachers on their knowledge, attitude, and function toward ADHD students. With regard to these issues, in fact due to the short number of conducted studies in Iran, this study was approved of being conducted.
Methods
This study was a randomized controlled trial. Since it was impossible to get samples from all Districts of Education Department of Isfahan, 70 primary school teachers, just from the District one were randomly selected. This study was conducted in Education Department Counseling Center in Isfahan. All subjects read and signed a written consent form before entering the study. They were randomly allocated into two groups of 35 participants. One group underwent a two-day workshop education and the other one (the study group) was educated by booklets in non-attendance method. Firstly, the subjects were explained about the methodology and the goal of work in an orientation session. Then, an educational workshop was held by an assistant professor, a subspecialist of a child and adolescent psychiatry and her fellowship assistant for two days. After filling demographic data forms including age, sex, teaching experience and working experience with ADHD students by both groups, a pretest on teachers’ knowledge, attitude and knowledge of function toward ADHD was done. The questionnaire, used in this study, has already been used in a similar study14 . In this study, validity of data collection tool was confirmed by face validity whereas the reliability was obtained by a Pilot study conducted on primary school teachers and calculation of Cronbach's alpha.14 Face validity of data collection method was done through consulting with experts of child and adolescent psychiatry and content validity was approved after some changes. To measure the reliability of questionnaire, 11 teachers with sufficient standards completed them and by using SPSS Cronbach's alpha was assigned which was 0.75 for knowledge questionnaires, 0.79 for attitude questionnaires and 0.71 for function questionnaires. The only inclusion criterion in this study was having working experience of over 5 years. Exclusion criterion for workshop education group was missing both days of the workshop and for the nonattendance group, was not studying the booklet. The workshop was hold in two days in a row in the consulting center of education department each day 5 for hours. At the ends of workshops, the subjects answered the post-tests of knowledge, attitude and knowledge of function questionnaires. The educational content, on the first day of the workshop, included recognition and definition of ADHD, epidemiology, etiology, differential diagnosis, accompanied disorders, prognosis and the treatment.
On the second day, it was about unreal beliefs about the disorder, ADHD impulse and hyperactivity control, strategies for attention increase in classrooms and schools, the manner of teacher-parents and teacher–psychiatrist relationship as well as the way of students’ referrals. The second groups were educated by educational booklets in nonattendance method with the precise educational content similar to that of the workshop.
The booklet had been prepared through consultation with a child and adolescents subspecialist of psychiatry and had been approved by Isfahan Behavioral Sciences Research Center. The subjects in this group took part in a post test of knowledge, attitude and knowledge of function ten days after they had studied the booklet.
This questionnaire included a questionnaire of demographic data including age, sex, teaching experience, teaching experience with ADHD children; the knowledge questionnaire, a 33-item questionnaire with 3 responses of “Right”, “Wrong” and “No Idea” concerning DSM-IV-TR criteria, epidemiological disorder, etiology, accompanied disorders, differential diagnosis and ADHD prognosis. Each “Right” answer scored +1, “Wrong” answer scored -1 and “No idea” scored 0. The questionnaire of attitude included nine 5-response questions as “Totally agreed”, “Agreed”, “No idea”, “ Disagreed” and “Totality disagreed”. Scoring scale was +5 for the correct answer and +1 for the wrong one. Functional knowledge questionnaire included thirty three 3-response questions as “Always”, “On average ”and “Never” for which each correct answer of “Always” scored +2, “On average” +1 and each answer of “Never” was coded as zero. This questionnaire was on teachers’ function and their strategies to control ADHD students. In group of workshop, 33 subjects remained in the study and two were left out of the study due to attending just one day to the workshop.
In nonattendance group, 34 subjects took part in the study; one did not take post-test due to being sick. The data were analyzed using SPSS version 18 and the mean score (SD) of variables calculated. Then, mean scores of teachers’ knowledge, attitude and knowledge of function between the two groups were compared using ANCOVA test.
Results
Among 67 teachers attending the study, the mean age was 41.67±7.61 years ranging between 25-55 years. All subjects were accidentally married and had experience of teaching ADHD students.
In order to perform co-variance analysis, the normal response variable and the variance between the two groups must be the same. The normal distribution of the variables (knowledge, attitude, and teacher function) were approved and the Levene's test showed similar variances of the scores in knowledge, attitude and knowledge of function (p > 0.05).
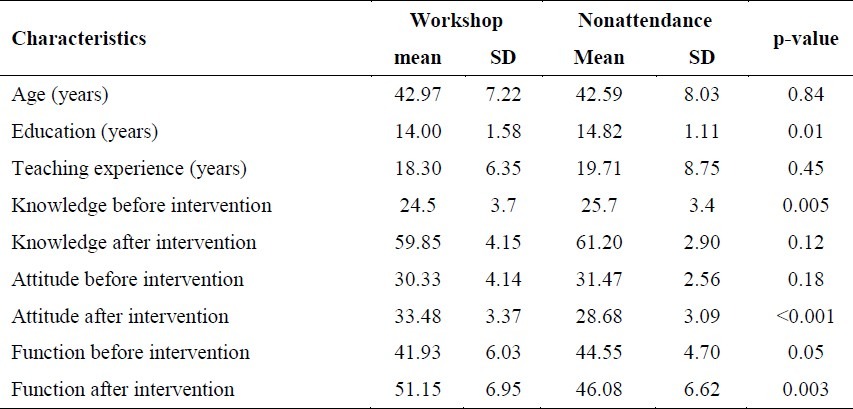
Based on the above table, mean year of education, with regard to calculation of 12 years for a high school diploma, 14 years for an associate degree and 16 years for a bachelor's degree, was 14±10.5 in workshop group and 14.82±2.5 in nonattendance group. Mean year of experience in workshop group was 18.3±6.5 and in nonattendance group was 19.71±9.75.
As presented in table 2, the mean scores of knowledge between the two groups of workshop and nonattendance (after checking the controlling variable) was not significantly different after intervention (p = 0.8) which means that the increase in teachers’ knowledge was nearly the same in workshop and non-attendance group.
Table 2.
Summarized results of teacher knowledge, attitude and knowledge of function.
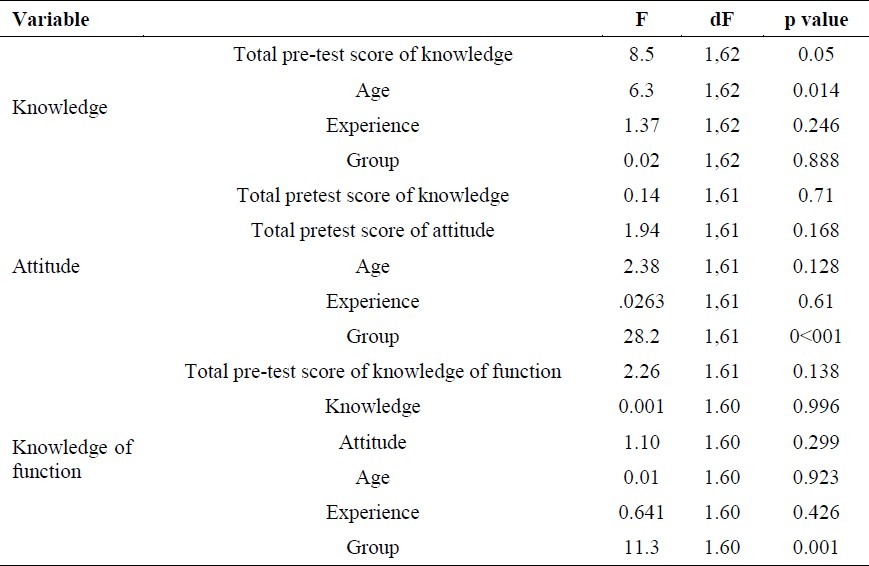
Table 1.
The mean (SD) of demographic characteristics in teachers based on two groups of workshop and nonattendance education.
Based on the table 2, the mean scores of attitude showed a significant difference between the two groups (p < 001) which means that in workshop group, the change in teachers’ attitude after education was more positive compared to that of nonattendance group.
Finally, as presented in table 2, mean scores of knowledge of function between the two groups showed a significant difference (after checking the controlling variable) (p = 0.001) which means that knowledge of function in workshop group was more promoted after intervention compared to that of non-attendance group.
Discussion
There was no significant association between mean scores of knowledge between the two groups of workshop and nonattendance education. Both groups answered to the post-tests appropriately. It seems that nonattendance education has increased teachers’ knowledge as much as workshop education. The less knowledge teachers have about ADHD, the more destructive behaviors the children may have in the classrooms.15 Former studies have shown workshop education to be more effective in increasing teachers’ knowledge.16 Nowadays, E-learning through internet and computers has yielded positive results.
In a study (2006), conducted on 7-14 year old adolescents, on E-education of anxiety management strategies,_it was revealed that this method of education was effective to decrease anxiety.17
In another comparative study on the effect of cognitive behavioral therapy to decrease adolescents’ anxiety by two methods of attendance and non-attendance education, no significant difference was seen. But, non-attendance method took less time (4 sessions) compared to attendance method (12 sessions). In regards to the attitude, there was a significant difference between the two groups (p < 0.05) which means that workshop group showed more attitude change than nonattendance group. Since, workshop education is counted as an active face to face method18 and with regards to the fact that a change in attitude needs different steps, of which, one is having active education and relationship with learners,19, this method seems to be a more effective method to change attitude19 compared to nonattendance method. There was a significant difference between knowledge of function mean scores of the two groups (p < 0.05). It was so that the knowledge of function had been more promoted in the workshop education compared to nonattendance group.
Although enough knowledge about behavioral strategies is essential to have appropriate knowledge of function, it cannot guarantee appropriate practice in real situations. Although such tests are not valid enough to measure individuals’ field function20, with regard to the measurement of knowledge of function, it seems in workshop group, compared to nonattendance group, the problems are better solved due to discussing teachers’ problems in details and getting an answer of face to face.18
Conclusion
Nonattendance education has been effective to increase teachers’ knowledge in dealing with ADHD as much as workshop education, but workshop education seems better for an attitude change and increase of knowledge of function compared to nonattendance education.
Limitations
This short term study was conducted on primary school teachers in District one Education Department in Isfahan, which can be counted as a limitation. Further long term studies are suggested to be conducted with a higher number of samples and in all Districts of Education Department in the city with post-tests taken in the 3rd and 6th month post-intervention in order to check the retention of teachers’ knowledge and its application in the classrooms. The quality of the workshop affects the results, and it could be considered as a limitation of study. Another limitation for this study was preparation of a primary booklet with an applicable content for primary school teachers who had lots of experience in facing with this sort of students in classrooms.
Authors’ Contributions
NS and MK carried out the design and coordinated the sessions of teachers, collected data and prepared the manuscript. NS wrote the booklet for teachers and it was approved by MK and SMA. MRM statistically analyzed the data and participated in writing manuscripts. SMA suggested the title. All authors have read and approved the content of the manuscript.
Acknowledgement
This research was conducted based on RCT number 201105212417N7 and project number 390033 by the Vice–chancellor Office for Research Affairs, Isfahan University of Medical Science with cooperation of Isfahan Behavioral Research Center and District one of Education Department of Isfahan.
Footnotes
Conflict of Interests Authors have no conflict of interests.
References
- 1.Sadock BJ, Kaplan HI, Sadock VA, Ruiz p. 9th ed. Philadelphia: Lippincott Williams & Wilkins; 2009. Kaplan & Sadock's Comprehensive Textbook of Psychiatry. [Google Scholar]
- 2.L acrimiora S, Eugen Arnold L. Attention deficit hyperactivity disorders. In: Martin A, Wolkmar FR, editors. Lewis's Child and Adolescent Psychiatry: A Comprehensive Textbook. 4th ed. philadelphia: Lippincott Williams & Wilkins; 2007. [Google Scholar]
- 3.Mash EJ, Barkley RA. 3th ed. New York: Guilt Ford Press; 2001. Assessment of Childhood Disorders. [Google Scholar]
- 4.Barkley RA. New York: Guilt Ford Press; 1990. Attention-Deficit Hyperactivity Disorder: A Handbook for Diagnosis and Treatment. [Google Scholar]
- 5.Steven R, Pliszka SR. Attention deficit hyperactivity disorder. In: Dulcan MK, editor. Dulcan's Textbook of Child and Adolescent Psychiatry. Arlington: American Psychiatric Publishing, Inc; 2009. p. 205. [Google Scholar]
- 6.Perlod M, Louw C, Kleymhans S. Primary school teachers’ knowledge and misperceptions of attention deficit hyperactivity disorder (ADHD) South African Journal of Education. 2010;30(3):457–73. [Google Scholar]
- 7.Reid R, Vasa SF, Maag JW, Wright G. An analysis of teacher's perception of Attention Defecit Hyperactity disorders. Journal of Research and Development in Education. 1994;27(3):195–202. [Google Scholar]
- 8.Sciutto MJ, Terjesen MD, Bender Frank As. Teachers’ knowledge and misperceptions of Attention-Deficit/Hyperactivity Disorde. Psychology in the Schools. 2000;37(2):115–22. [Google Scholar]
- 9.Ohan JL, Visser TA, Strain MC, Allen L. Teachers’ and education students’ perceptions of and reactions to children with and without the diagnostic label “ADHD”. J Sch Psychol. 2011;49(1):81–105. doi: 10.1016/j.jsp.2010.10.001. [DOI] [PubMed] [Google Scholar]
- 10.Runnheim VA, Frankenberger WR, Hazelkorn MN. Medicating students with emotional and behavioral disorders and ADHD: A state survey. Behavioral Disorders. 1996;21(4):306–14. [Google Scholar]
- 11.Schumm JS, Vaughn S. Meaningful professional development in accommodating students with disabilities. Remedial and special Education. 1995;16(6):344–53. [Google Scholar]
- 12.Zentall SS, Javosky J. Professional develop for teachers of student with ADHD and characteristic of ADHD. Behavioral Disorders. 2007;32(2):78–98. [Google Scholar]
- 13.Ghanizadeh A, Bahredar MJ, Moeini SR. Knowledge and attitudes towards attention deficit hyperactivity disorder among elementary school teachers. Patient Educ Couns. 2006;63(1-2):84–8. doi: 10.1016/j.pec.2005.09.002. [DOI] [PubMed] [Google Scholar]
- 14.Azhar S, Safari P. Development, Implementation and Evaluation of the Efficacy of ADHD Workshop on Knowledge, Attitude and Practice of Primary School Teachers.Isfahan: Isfahan University of Medical Science; 2010. [Research Number in Isfahan University of Medical Science 3387347] 2010 [Google Scholar]
- 15.Karbasi A, Arman S, Maracy MR. The efficacy of attendance and semi-attendance group cognitive-behavioral therapy (CBT) on the anxiety disorders of adolescent girls. J Res Med Sci. 2010;15(5):256–63. [PMC free article] [PubMed] [Google Scholar]
- 16.Jeneva L, Shellane L, Troy A, Strain W. Does knowledge about attention – deficit – hyperactivity disordes impact teachers repoted behavior and perceptions? School Psychology Quarterly. 2008;23(3):436–49. [Google Scholar]
- 17.Spence SH, Holmes JM, March S, Lipp OV. The feasibility and outcome of clinic plus internet delivery of cognitive-behavior therapy for childhood anxiety. J Consult Clin Psychol. 2006;74(3):614–21. doi: 10.1037/0022-006X.74.3.614. [DOI] [PubMed] [Google Scholar]
- 18.Lucas RW. Designing, Developing, and Delivering and Learning Events that Get Results. Richfield: Pfeiffer; 2009. Training Workshop Essentials. [Google Scholar]
- 19.Aronson E, Timothy DW, Rohin M, Wilson T, Akret R. 4th ed. New Jersey: Prentice Hall; 2001. Social Psychology. [Google Scholar]
- 20.Zolfaghari B, Adibi N, Darakhshanfar S, Tansaz M, Karbasi A, Niroomand A. Isfahan: Neshat; 1998. Academic Developing Scales. [Google Scholar]