

Abstract
A systematic review and meta-analysis of memory training research was conducted to characterize the effect of memory strategies on memory performance among cognitively intact, community-dwelling older adults, and to identify characteristics of individuals and of programs associated with improved memory. The review identified 402 publications, of which 35 studies met criteria for inclusion. The overall effect size estimate, representing the mean standardized difference in pre-post change between memory-trained and control groups, was 0.31 standard deviations (SD; 95% confidence interval (CI): 0.22, 0.39). The pre-post training effect for memory-trained interventions was 0.43 SD (95% CI: 0.29, 0.57) and the practice effect for control groups was 0.06 SD (95% CI: -0.05, 0.16). Among 10 distinct memory strategies identified in studies, meta-analytic methods revealed that training multiple strategies was associated with larger training gains (p=0.04), although this association did not reach statistical significance after adjusting for multiple comparisons. Treatment gains among memory-trained individuals were not better after training in any particular strategy, or by the average age of participants, session length, or type of control condition. These findings can inform the design of future memory training programs for older adults.
Keywords: memory training, memory, strategy use, meta-analysis, mnemonics
Introduction
Training programs designed to enhance memory among older adults have proliferated in recent years. Memory training programs exist within the larger context of cognitive training, which is based on the notion that cognition is plastic in older age (Acevedo & Lowenstein, 2007; Rebok, Carlson, & Langbaum, 2007). Through cognitive plasticity and reserve (Stern, 2002), mentally stimulating activities like memory training help maintain and improve cognitive and functional abilities in daily life (Hertzog et al., 2008). Memory training interventions facilitate plasticity by teaching various strategies that help encode and retrieve information (Gross & Rebok, 2011; McDaniel, Einstein, & Jacoby, 2008; Rebok et al., 2007; Verhaeghen, Marcoen, & Goossens, 1992). In addition to improving objective memory performance, research shows interventions can improve self-rated subjective memory (Floyd & Scogin, 1997).
Memory training interventions among older adults with no cognitive impairment seek to improve memory skills by teaching mnemonic techniques. Common mnemonic strategies include rehearsal (Gordon & Berger, 2003; Heun, Burkart, & Benkert, 1997; Howe et al., 1985; Kennedy & Miller, 1976), association (Bjorklund & Douglas, 1997; West, 1985), categorization (Bjorklund, Schneider, Cassel, & Ashley, 1994; Gobet, Lane, Croker, Cheng, Jones, et al., 2001; Ornstein & Naus, 1978; Schneider & Sodian, 1988), imagery (Bower, 1970; Poon et al., 1980; Rankin, Karol, & Tuten, 1984; Rasmusson et al., 1999; Richardson, 1998; Sharps & Price-Sharps, 1996), and concentration (Stigsdotter & Bäckman, 1989). Combinations of these strategies are often taught in memory training programs and include face-name recognition and name-face learning, number mnemonics, story mnemonics, and the method of loci. Additionally, training programs often entail instruction in how to take advantage of environmental supports, called external memory aids.
Evidence from several studies suggests training may help maintain, or potentially enhance, memory performance in later adulthood. Specifically, the Advanced Cognitive Training for Independent and Vital Elderly (ACTIVE) study, the largest randomized trial of cognitive training among older adults to date, reported a retest-adjusted effect size of 0.26 standard deviations (SD) comparing memory gains immediately after memory training with change in the no-contact control group, and an effect size of 0.23 SD five years after training (Willis et al., 2006). The potential for improvement in memory is mirrored by findings from systematic reviews and meta-analyses of memory training. Verhaeghen and colleagues (1992) reported an average standardized pre-post training gain of 0.73 SD in memory performance from training, indicating memory training can improve memory in cognitively normal older adults. Additionally, Verhaeghen et al. (1992) reported that mnemonic strategies that capitalized on imagery were most effective for increasing memory performance. Many studies have been conducted in the decades since the review by Verhaeghen and colleagues was published, and the topic of effective memory training strategies is worth revisiting. Further, their estimate did not adjust for practice, or retest, effects, which were 0.37 SD for placebo or active control groups and 0.36 SD for no-contact control groups (Verhaeghen et al., 1992). Retest effects are artifacts of prior test experience rather than of processes of interest to a research question (Salthouse & Tucker-Drob, 2008; Salthouse, 2010). They are attributable to changes in attention and increased expectancy that arise with repeated test administrations, and are important to account for in studies with repeated measures because prior exposure to test materials provides knowledge and test-taking experience that confound true training-related performance gains (Crawford et al., 1989; Mitrushina et al., 2005). More recently, a meta-analysis by Zehnder and colleagues (2009; Martin, Clare, Altgassen, Cameron, & Zehnder, 2011) studied the effect of memory training on particular memory abilities, and reported training effects for paired associate learning, immediate recall, and delayed recall.
Memory training for older adults has proliferated in recent years, often without rigorous empirical testing. Researchers and commercial businesses (e.g., Burden, 1988) have developed memory training programs that target particular populations of older adults, including those with no cognitive impairment (e.g., Willis et al., 2006), mild cognitive impairment or memory complaints (e.g., Craik et al., 2007), and dementia (Cherry & Simmons-D’Gerolamo, 2005; Zanetti et al., 1997). Programs for cognitively normal older adults, the focus of the present article, typically entail interactive group sessions over several days or weeks with a trainer (e.g., Zarit, Cole, & Guider, 1981), but also include self-guided training with take-home packets (e.g., Burden, 1988; Scogin et al., 1985).
Research on the impact of participant and program characteristics on memory training effectiveness is widespread but has produced conflicting results. Existing evidence suggests older age is associated with less training benefit (Verhaeghen et al., 1992; Yesavage, Sheikh, Friedman, & Tanke, 1990), though not all studies replicate this finding (e.g., Rasmusson et al., 1999; Schmidt et al., 2001; Singer, Lindenberger, & Baltes, 2003; Wolters, Theunissen, Bemelmans, van der Does, & Spinhoven, 1996). Effects of adherence and training length are understudied in memory training research. Although prior studies have demonstrated memory gain following mnemonic instruction over only one or two sessions (e.g., Rebok & Balcerak, 1989), group-based memory training programs typically last between five and fifteen hour-long sessions (Mahncke et al., 2006; Rebok et al., 2007).
Altogether, prior studies of memory training in later life have reported training interventions benefit older adults’ memory. Existing studies, however, seldom have evaluated training effects by the type of mnemonic strategy employed. The present systematic review and meta-analysis summarizes nearly 50 years of memory training research to address the following questions: (1) What is the average overall pre-to-post difference in effect between memory-trained and control groups? (2) Are particular mnemonic or other strategies taught during training more effective than others in improving memory? and (3) Are participant or program characteristics, such as participant age or intervention duration, associated with greater intervention effectiveness among community-dwelling older adults?
Methods
A comprehensive review was conducted of research on memory training interventions for cognitively normal older adults published or in press prior to January, 2010. To identify relevant studies, computerized databases (PsychInfo, PsychLit, PubMed) were searched using combinations of the following key words: memory, mnemonic, cognitive, cognition, intervention, training, rehabilitation, stimulation, learning, improvement, enhancement, older adult, aging, elderly, and impairment. We searched published reviews and meta-analyses (e.g., De Vreese et al., 2001; Floyd & Scogin, 1997; Grandmaison & Simard, 2003; Sitzer et al., 2006; Storandt, 1991; Verhaeghen et al., 1992); and performed hand searches of journals (e.g., Applied Cognitive Psychology; Educational Gerontology; Cognitive Technology; Psychology and Aging), and book chapters (e.g., Hill, Bäckman, & Stigsdotter-Neely, 2000). Authors of memory training studies were contacted for recently published or in press studies. Additional studies were identified from reference lists in retrieved articles.
Inclusion criteria for this meta-analysis were based on criteria for identification of evidence-based treatments developed for the Committee on Science and Practice, Society for Clinical Psychology, and Division 12 of the American Psychological Association. Detailed procedures for identifying, reviewing, and coding studies of psychological interventions are described in detail by Weisz and Hawley (2001). To be included in the present review, publications were required to report original data on memory training. All participants had to be at least 60 years of age at the time of training. This criterion was necessary because a treatment in a different age group is considered a new application of the treatment and may have different effects (Chambless & Hollon, 1998). Studies must have used a non-pharmacological approach targeted at memory or memory problems (Weisz & Hawley, 2011), and had to be published in English.
Theoretical articles, review articles, and book chapters that did not include original data were excluded. Studies were also excluded if the study design tested effects of a combination of memory training and pharmacotherapy or exercise therapy because we did not want to confound effects of memory training with pharmacologic effects. If the treatment program only involved practice with memory tasks or instruction manipulation but no training (e.g., psychological experiments on memory), we excluded the study. If there was no comparable control group (block randomization or comparable control groups were accepted in lieu of full randomization), we were unable to disambiguate treatment effects from baseline differences. Further, only outcome measures of objective memory performance were collected from eligible studies; outcome measures of other cognitive domains (e.g., executive functioning, attention), global cognitive status, and everyday function were excluded.
Strategy ascertainment
Initially, 402 articles published between 1967 and 2010 were deemed relevant to the present review. Not all these studies were appropriate for our review. Two independent reviewers reviewed each study and extracted information about the study design, sample age, memory outcomes, and means and standard deviations of memory tests before and after training in trained and control groups. Percent agreement among reviewers was high (95%), suggesting excellent inter-rater reliability. All differences were resolved by consensus. Raters also coded specific memory strategies taught as part of the training program. Mnemonic strategies were classified into rehearsal, associations, categorization, imagery, concentration, face–name recognition, number mnemonics, story mnemonics, method of loci, and external memory aids. In several cases, authors were contacted for their training manuals (e.g., Dunlosky et al., 2003; Scogin et al., 1985). These categories were determined post hoc after a thorough review of each eligible study. Mnemonic strategy classifications are described below.
Rehearsal entails repetition of information to facilitate encoding (Gordon & Berger, 2003; Heun, Burkart, & Benkert, 1997; Howe et al., 1985; Kennedy & Miller, 1976). Associations are links or connections formed between items with respect to time, environment, or specific item characteristics, and made using images, senses, words, and sentences (Bjorklund & Douglas, 1997; West, 1985). Categorization involves recognizing and grouping items by conceptual relations to facilitate remembering (Bjorklund et al., 1994; Gobet et al., 2001; Ornstein & Naus, 1978; Schneider & Sodian, 1988). Imagery entails binding together concepts or items into an integrated, often visual, representation (Bower, 1970; Poon et al., 1980; Rankin, Karol, & Tuten, 1984; Rasmusson et al., 1999; Richardson, 1998; Sharps & Price-Sharps, 1996). Visual imagery is useful for list-learning, prospective memory, and other types of memory. Training in concentration involves enhancing listening and information processing skills using divided attention and selective processing tasks (Stigsdotter & Bäckman, 1989).
Combinations of rehearsal, association, categorization, imagery, and concentration are often taught in memory training programs as stand-alone strategies helpful in particular contexts. These strategies include face–name recognition and name–learning techniques, number mnemonics, and story mnemonics. Face–name recognition is used to remember names and faces together by integrating mnemonic devices like visual imagery, categorization, and association to link a person’s name with his or her facial characteristics (Andrewes et al., 1996; Becker, McDougall, Douglas, & Arheart, 2008; Best et al., 1992; Calero & Navarro, 2007; Calero–Garcia & Navarro–Gonzalez, 2007; Craik et al., 2007; Dunlosky et al., 2003; Fabre et al., 2002; Lachman et al., 1992; Lustig, 2008; Mohs et al., 1998; Stigsdotter et al., 1989; Woolverton et al., 2001). Number mnemonics, also referred to as the phonetic system, digit–consonant method, and the major system (Worthen & Hunt, 2011), are used to remember strings of numbers like dates, phone numbers, and addresses (Calero & Navarro, 2007; Calero–Garcia & Navarro–Gonzalez, 2007; Derwinger et al., 2005; Hill et al., 1997). Use of this strategy entails creating a codebook to substitute letters for numbers by associating all numbers with characters or phonemes, generation of words and phrases using letters that correspond with to-be-remembered numbers, and finally, translating the word or phrase back into the original numbers using the codebook. Story and sentence mnemonics involve creating a story or sentence with to–be–remembered items to facilitate recall (e.g., Hill et al., 1991). This type of strategy relies on the distillation of thoughts or items into representative words or phrases (Small, 2002).
The method of loci is a formal visuo-spatial mnemonic device that takes advantage of known places, such as body parts or landmarks on the way to work, and pairs each location with a to-be-remembered item (Bower, 1970; Yates, 1966). This structured sequence of images provides memory cues to facilitate recall (Hill et al., 1991; Kliegl, Smith, & Baltes, 1989, 1990; Rebok & Balcerak, 1989; Verhaeghen & Marcoen, 1996; Yesavage & Rose, 1984).
External memory aids are environmental cues that enhance memory and everyday functioning (Andrewes et al., 1996; Best et al., 1992; Caprio-Prevette et al., 1996; Craik et al., 2007; Flynn et al., 1990; Hanley & Lusty, 1984; McPherson et al., 2001; Nolan et al., 2001; Scogin et al., 1985; Scogin et al., 1992; Scogin et al., 1998; Woods et al., 2006; Woolverton et al., 2001; Worthen & Hunt, 2011). External memory aids include lists, reminder notes, calendars, and messages to one’s self.
Effect size calculation
To characterize the immediate effect of memory training on memory among older adults, effect sizes were calculated in two ways. First, average pre-post effect sizes were calculated for memory-trained and control groups separately. Most studies reported multiple measures of memory ability, and we took an arithmetic mean of the effect sizes for these measures. Common memory tasks used to measure memory included verbal word list-learning tasks (Auditory Verbal Learning Test (Rey, 1964), California Verbal Learning Test (Delis et al., 1987), Hopkins Verbal Learning Test (Brandt & Benedict, 2001)), paragraph recall (e.g., Rivermead Behavioral Memory test (Wilson, Cockburn, & Baddeley, 1985)), and assorted tests of recall for numbers, images, and shopping lists. For each memory outcome provided by a study, the mean difference between the post-training and pre-training scores for the trained group was divided by the pooled standard deviation to place all effect sizes on the same scale. The same was done for the control group. These effect sizes are within-study averages of all reported memory measures that represent a study-specific training effect and a control retest effect. We used these study-specific composites of memory performance because the present study’s goal was to make statements about the construct of memory and not to distinguish types of memory. An advantage of using composites is they are likely less similar to tasks on which participants were trained than some specific memory tests used by a study to measure training effects. We did not distinguish memory measures by primary or secondary outcomes as identified by each individual study. Pre-training and post-training means and standard deviations were available from almost all studies; standard deviations were determined from inferential statistics (e.g., F statistics, t statistics, confidence intervals on barcharts) in five cases (Andrewes et al., 1994; Best et al., 1992; Caprio-Prevette & Fry, 1996; Yesavage, 1983, 1984). In these five cases, pre-post effect sizes were calculated using inflated standard deviation estimates to account for correlation between the two measures (Dunlap, Cortina, Vaslow, & Burke, 1996).
Retest-adjusted effect sizes were also calculated by taking a difference in pre-post change between memory and control groups for each memory measure in a study, and standardized using a pooled standard deviation. Unlike the first set of effect sizes, which were standardized differences in memory change between baseline and immediate post-training assessments and provided largely for descriptive purposes, retest-adjusted effect sizes represent memory change attributable to training by adjusting for a retest effect in control groups. The latter set of effect sizes was used for the meta-analysis in the present study. This analysis assumed that retest effects are comparable between trained and control participants.
Statistical analysis
Meta-analytic procedures were used to analyze retest-adjusted effect sizes from the systematic review. Study-specific effect size estimates were weighted by the study sample size and combined to form an overall effect size. Forest plots were constructed to display study-specific effect sizes. Funnel plots were used to visually inspect evidence of publication bias. Between-study heterogeneity was quantified using χ2 and I2 statistics, the latter of which is interpreted as the chance-adjusted percent of total variation attributable to between-study heterogeneity. Sources of heterogeneity were explored using separate random effects meta-regressions of effect size estimates on covariates. Because of the small sample size, separate meta-regressions were performed for each of the 15 predictors. A two-sided α-level <0.05 was used as a cutoff for statistical significance, although results from meta-regressions were adjusted for multiple comparisons using a Bonferroni adjustment (Bonferroni, 1935). All analyses were performed using the Stata version 11.0 software package (StataCorp, 2010).
Results
Based on the stated inclusion and exclusion criteria, 33 of the 402 publications were memory training studies involving randomization to memory training for older adults and therefore eligible for inclusion in the present review. Common reasons for exclusion involved designs that mixed memory training with a pharmacological, physical, or social engagement intervention (e.g., Rozzini et al., 2007; Tárraga et al., 2006); samples with individuals under 60 years of age (e.g., Bherer et al., 2006; Erickson et al., 2007; Hildebrandt et al., 2006; McKitrick, Camp, & Black, 1992; Troyer et al., 2008); studies without comparable control groups (e.g., Morrell, 2006); or theoretical or review articles (e.g., Acevedo & Loewenstein, 2007; Belleville, 2008; Clare & Woods, 2004; Dunlosky et al., 2007; McDougall, 2004).
The 33 publications provided 35 separate treatment-control studies because two studies included multiple treatment conditions alongside a control condition (Derwinger et al., 2005; Woolverton et al., 2001). From these, nine different mnemonic strategies and external memory aids used in memory training were identified with a total participant sample of 3,797 (Table 1). The mean sample age among included studies was 72.7 years (SD = 4.3; range of actual ages = 60 to 98 years). Most participants assigned to training completed the training according to study criteria (e.g., attended a certain number of sessions) or at least provided data at post-training. Training programs lasted anywhere in total duration from 30 minutes to 24 hours; most were administered in between one and 20 sessions. The majority of memory interventions were conducted in a group format. All studies followed an established, consistent protocol (Table 1).
Table 1.
Descriptive Statistics of 35 Studies Included in the Meta-Analysis
| Variable | Range | |
|---|---|---|
| Sample age, mean (SD) | 72.7 (4.4) | 65, 81.9 |
| Number of sessions, mean (SD) | 10.5 (8.0) | 1, 40 |
| Number of hours, mean (SD) | 12.8 (9.2) | 0.5, 42 |
| Completed training, % (SD) | 90.0 (10.0) | 56, 100 |
| Randomization, number of studies (%) | 26 (72.2) | |
| Placebo versus no-contact control, n (%) | 13 (36.1) | |
| Internal mnemonic strategies, n (%) | ||
| Method of Loci | 15 (42.9) | |
| Association | 14 (40.0) | |
| Categorization | 15 (42.9) | |
| Visual imagery | 23 (65.7) | |
| Face-name / Name-learning | 20 (57.1) | |
| Rehearsal | 3 (8.6) | |
| Attention | 10 (28.6) | |
| Number mnemonics | 6 (17.1) | |
| Story mnemonics | 2 (5.7) | |
| External memory aids | 10 (28.6) | |
| Number of strategies trained, n (%) | ||
| 1 | 10 (28.6) | |
| 2-3 | 11 (31.4) | |
| 4-5 | 7 (20.0) | |
| 6-7 | 7 (20.0) |
Note. Marginal counts of strategies used in particular studies add up to more than the 35 studies included in the present review because most studies taught multiple strategies. Nonrandomized controlled studies were included that used block randomization or matching procedures to identify a comparable control group.
n: number of studies; SD: standard deviation.
Among strategies taught for improving memory, visual imagery was the most prevalent, followed by face-name and name-learning techniques (Table 1). Only 29% of programs trained on a single strategy. The majority of memory training programs taught between two and seven different strategies. The most common combination of strategies was at least three of the following: method of loci, association, categorization, and visual imagery (Ball et al., 2002; Becker et al., 2008; Best, Hamlett, & Davis, 1992; Calero & Navarro, 2007; Calero-Garcia & Navarro-Gonzalez, 2007; McDougall et al., 2010; Scogin & Prohaska, 1992).
Effect sizes with 95% confidence intervals for each study in the present review are shown with a Forest plot (Figure 1). The overall pre-post training gain was 0.43 SD (95% CI: 0.29, 0.57) and the mean retest effect among control groups was 0.06 SD (95% CI: -0.06, 0.16; Table 2). Figure 2 reveals bell-shaped distributions of training and control effect sizes and a broader range of training effects than retest effects. The latter observation is consistent with tests of heterogeneity in Table 2. The mean standardized difference in pre-post change between memory and control groups was 0.31 SD (95% CI: 0.22, 0.39), indicating that, on average, memory-trained participants demonstrated a 0.31 SD greater improvement in memory performance than participants in the control condition. This difference was statistically significant (p < 0.001). A funnel plot of these effect sizes shows minimal asymmetry and thus no evidence of publication bias, although two studies (Best et al., 1992; Hill et al., 1990) provided very large effect sizes (Figure 3).
Figure 1. Forest Plot of Effect Sizes.
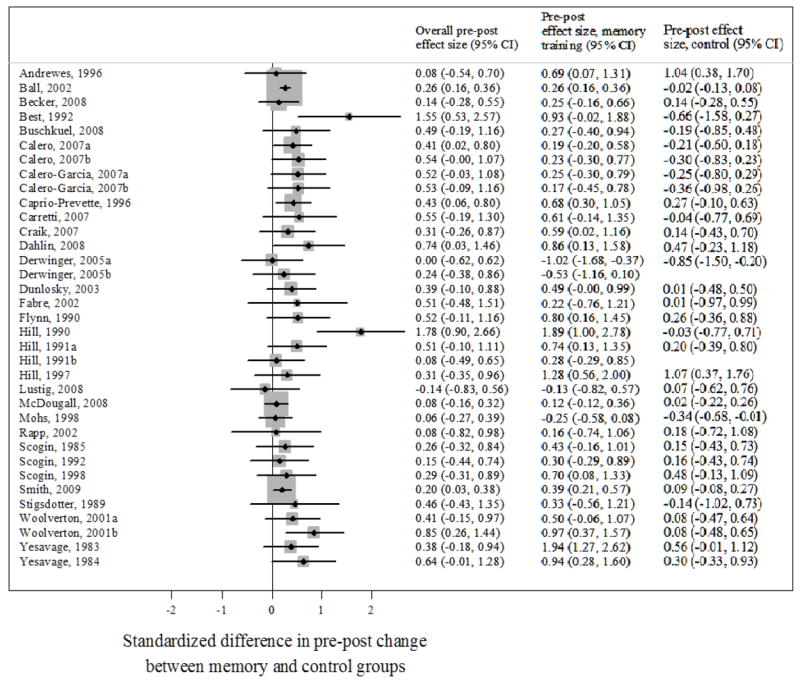
Legend. Effect sizes representing retest-adjusted standardized differences (in standard deviation units) in pre-post memory change between memory-trained and control groups are graphed. Training and control group-specific effect sizes are also provided in columns at right. Control effect sizes are not shown for two studies because the same control group was used to compare against more than one memory training intervention.
95% CI: 95% confidence interval.
Table 2.
Overall and Treatment-Specific Group Effect Size Estimates
| Effect size | 95% CI | Number of participants at post-training | Number of studies | Q statistic
|
Iˆ2 | ||||
|---|---|---|---|---|---|---|---|---|---|
| χ2 | Degrees of freedom | p-value | |||||||
| Overall | 0.31 | (0.22, 0.39) | 3797 | 35 | 38.41 | 34 | 0.24 | 12.40% | |
| Training | 0.43 | (0.29, 0.57) | 1930 | 35 | 107.03 | 34 | <0.001 | 68.20% | |
| Control | 0.06 | (-0.05, 0.16) | 1867 | 33 | 50.22 | 32 | 0.02 | 36.30% | |
Legend. The overall effect size represents the difference in standard deviation units in pre-post memory change between memory-trained and control groups. Effect sizes specific to training groups represent standardized pre-post changes (in standard deviation units) in memory for the group of studies.
95% CI: 95% confidence interval.
Figure 2. Distribution of Study Effect Sizes by Training Status.
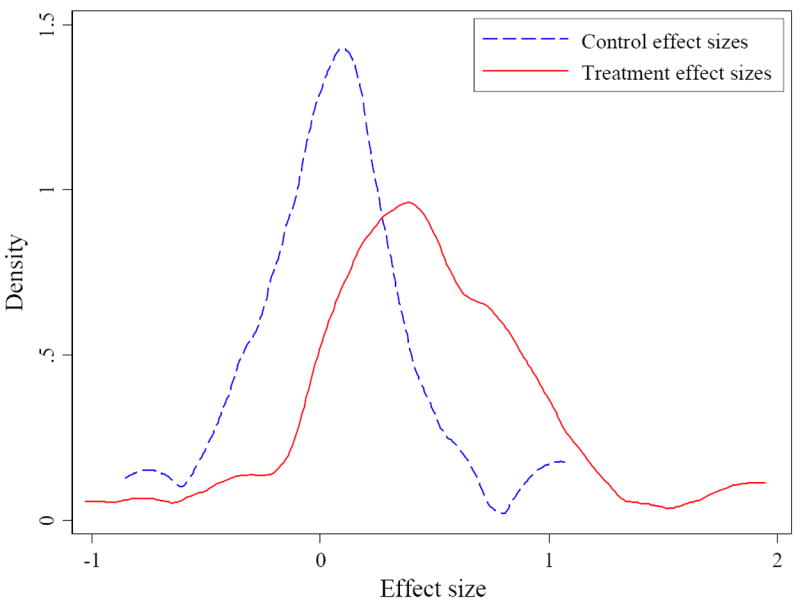
Legend. Effect sizes represent standardized pre-post changes (in standard deviation units) in memory for memory-trained and control groups.
Figure 3. Funnel Plot of Effect Sizes with Pseudo 95% Confidence Intervals.
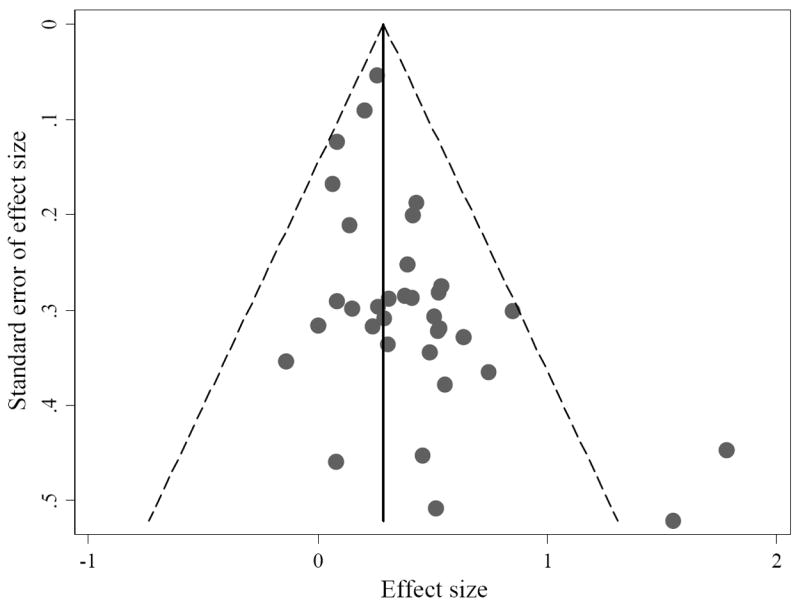
Legend. Effect sizes represent retest-adjusted standardized differences (in standard deviation units) in pre-post memory change between memory-trained and control groups. Diagonal dotted lines represent 95% confidence intervals of the expected distribution of studies around the mean memory effect size estimate for each standard error on the ordinate, assuming no between-study heterogeneity. They are referred to as pseudo because the lines are not strict confidence limits.
Statistical tests for heterogeneity in Table 3 (χ2 and I2) suggested negligible between-study heterogeneity in pre-post differences between training and control groups (Table 2), but for theoretical reasons and because pre-post changes in memory among memory-trained groups were heterogeneous, we further regressed effect sizes on several predictors in separate meta-regressions (Table 3). No individual or study characteristics (age, hours trained, percentage of completers, placebo versus no-contact control group) were associated with greater pre-post gains in memory-trained groups (Table 3). Although categorization and repetition mnemonic strategies were statistically significant at the α=0.05 level, they were not significant at the Bonferroni-adjusted α=0.003 level. We regressed effect sizes on the number of strategies. Similar to findings for individual strategies, the total number of strategies was also positively associated with an increased standardized pre-post difference between memory and control groups but was no longer significant after the Bonferroni correction (Table 3).
Table 3.
Meta-regressions of Effect Sizes on Selected Predictors
| Predictor | Pre-post effect size | |
|---|---|---|
| β | 95% CI | |
| Sample age | -0.01 | (-0.03, 0.01) |
| Number of hours | 0.00 | (-0.01, 0.00) |
| Percent who completed training | -0.34 | (-1.19, 0.51) |
| Placebo versus no-contact control | -0.10 | (-0.25, 0.06) |
| Internal mnemonic strategies | ||
| Method of Loci | 0.10 | (-0.06, 0.26) |
| Association | 0.07 | (-0.10, 0.23) |
| Categorization | 0.17 * | (0.00, 0.33) |
| Visual imagery | 0.06 | (-0.12, 0.24) |
| Face-name / Name-learning | 0.00 | (-0.17, 0.17) |
| Rehearsal | 0.38 * | (0.02, 0.75) |
| Attention | 0.09 | (-0.08, 0.27) |
| Number mnemonics | 0.16 | (-0.08, 0.41) |
| Story mnemonics | 0.12 | (-0.35, 0.58) |
| External memory aids | 0.15 | (-0.05, 0.35) |
| Number of strategies trained | 0.04 * | (0.00, 0.07) |
Legend. Effect sizes represent retest-adjusted standardized differences (in standard deviation units) in pre-post memory change between memory-trained and control groups from random effects regressions of effect sizes on covariates. Because of the small sample size (35 studies), separate regressions were performed for each of the 15 predictors.
p ≤ 0.05. No coefficients were significantly associated with effect sizes after applying a Bonferroni adjustment for multiple tests (adjusted α=0.003).
95% CI: 95% confidence interval.
Discussion
The present study reports results from a meta-analysis of nearly 50 years of memory training studies. Consistent with the view that memory can be improved in older adulthood, memory gains in training groups were larger than retest effects in control groups. The standardized difference in pre-post gain between memory and control groups was 0.31 SD, which is comparable to the difference between effect of training and the retest effect for control groups in the review by Verhaeghen and colleagues (1992) and is larger than in ACTIVE. Meta-regressions further revealed that providing training on more strategies was moderately associated with larger memory improvement. No other mnemonic strategies or study characteristics were significantly associated with memory improvement.
A challenge of memory training studies, like most cognitive training interventions, is that they often do not train abilities that generalize to everyday functioning (Hertzog et al., 2008). This is why an intervention’s scope, or the breadth of strategies trained, is important to characterize in any study. Individual strategies and the total number of strategies taught served as indicators of intervention scope in this study. Interventions that train more or broader techniques have a better chance than interventions that target fewer abilities of teaching something that resonates with an older adult, which they then might use to ameliorate their everyday lives (Hertzog et al., 2008). The trend for more improvement after training with more strategies trained, though not significant after adjustment for multiple comparisons, is consistent with the notion that studies with more variety of strategies have a larger scope and more chance of teaching strategies that older adults may internalize. This reasoning leads to the hypothesis that memory training interventions that train more strategies should yield more robust effects in everyday life; however, future research is needed to explore this possibility.
Suggestive but nonsignificant trends for larger effect sizes for rehearsal and categorization are worth mention. Because rehearsal was trained in only three of the 35 studies and never the only strategy trained, this finding is consistent with the notion that rehearsal in combination with other strategies can explain between-study variability. Although Ebbinghaus’ (1895/1964) seminal work on memory entailed memorizing nonsense syllables using only rote repetition, contemporary research indicates that rehearsal alone does not improve memory, but that it does provide an opportunity to form associations to facilitate other strategies used for recall (Worthen & Hunt, 2011). In contrast, nonsignificant trends for larger effect sizes with respect to categorization strategies are consistent with prior research (Verhaeghen et al., 1992; Zehnder et al., 2010). Grouping items into a smaller number of chunks or semantic units based on shared attributes makes encoding and subsequent information retrieval easier (Bousfield, 1953; Craik, 1981; Hunt & Love, 1972). Older adults who use more categorical clustering on memory tasks remember more than those who use less categorization (Bower, 1970; Craik et al., 2007; Mandler, 1967). Previous research also indicates older adults benefit from strategies that involve visual imagery (Verhaeghen et al., 1992) because the occipital region of the brain, responsible for visual information processing, does not deteriorate with age as much as the frontal lobes (Hazlett et al., 1998; Nyberg et al., 2003). That the present review did not find a significant association for imagery is likely because of its wide-spread use and considerable between-study heterogeneity in how imagery training is applied.
The average retest effect in control groups reported in the present study (0.06 SD) is much smaller than that reported by Verhaeghen et al. (1992) (0.37 SD). There are two potential reasons for this discrepancy. First, Verhaeghen et al. (1992) selected only target memory measures that were most likely to show a training effect given the specific training provided. For example, training in number mnemonics would have precluded a word list-learning test from being included in effect size calculations. Because the present study’s effect sizes incorporate a broader range of memory measures, some of which are less susceptible to practice effects than others, our effect size estimates are probably less affected by practice. Relatedly, the present study’s estimates are also more conservative because aggregate effect sizes are likely to include some memory outcomes that are more invariant to training interventions. Further, research suggests retest effects for some memory tests decline with age (e.g., word list-learning tests; Shapiro & Harrison, 1990). Studies included in the present review tended to include older samples (mean ages ranged from 65 to 81.9 years) compared with studies in the review by Verhaeghen and colleagues (mean ages ranged from 61 to 78 years).
In addition to research implications, identification of specific memory strategies for memory improvement has consequences for clinical practice (Rebok, Parisi, Gross, et al., in press). In memory clinics where clinicians receive memory complaints and diagnose memory problems, evidence-based memory training practices and programs can provide guidelines for decision-making about appropriate treatment protocols. This review’s findings present several options for patients who present with memory problems at such clinics and other health care settings. Importantly, identification of specific memory strategies may overlook self-generated, idiosyncratic, or hybrid techniques that are effective for some older adults, and so the present study’s findings should not substitute for experienced clinical judgment or ignore a given patient’s unique strengths and weaknesses.
Although the present study contributes to memory training research and practice, several caveats deserve comment. First, the review only includes published research studies. It does not include programs conducted in clinical or other settings or unpublished research trials, although efforts were made to contact potential authors of unpublished studies which led to inclusion of one eligible study (McDougall et al., 2010). Funnel plots revealed minimal evidence of publication bias. Further, a large intervention study among adults younger than 60 years using strategies common in commercially available cognitive training programs found similar training effect sizes (Owen et al., 2010), suggesting our results are valid.
Second, our inclusion criteria were stricter than previous studies of memory training. We felt justified in this because our criteria conform to published criteria for assessing psychological interventions (Weisz & Hawley, 2001), and because there is enough of a critical mass of memory training studies today we can afford to be selective. Another potential limitation is that, although the present analysis was limited to measures of memory exclusively, the measures are heterogeneous and reflect many types of memory (e.g., memory for numbers, lists, paragraph recall, visual memory). Despite this potential limitation, tests of heterogeneity suggested standardized differences in pre-post memory change between memory-trained and control groups were homogeneous across studies and meta-regressions were used to statistically account for unexplained between-study variance. Fourth, although the number of studies included in the present review is less than those in Verhaeghen et al. (1992) and thus might limit generalizability, the exclusion criteria relating to study design were more stringent to get as pure a sample of memory training studies as possible. Finally, the present review only considered studies among cognitively normal older adults. Other reviews have studied cognitive training in more cognitively impaired populations such as persons with dementia (Woods, Spector, Prendergast, & Orrell, 2006; Yu et al., 2009) and mild cognitive impairment (Belleville, 2008). Training among persons with dementia entails different training techniques than mnemonic training, including cognitive rehabilitation, spaced retrieval (Camp, 1989), or reality orientation therapy (Taulbee 1966; Woods et al., 2006).
Several areas of future research are indicated by the present meta-analysis. This study did not consider approaches that combined memory training with forms of pharmacotherapy (Yesavage et al., 2007), exercise (Colcombe & Kramer, 2003), or nutrition (Gonzalez-Gross, Marcos, & Pietrzik, 2001). Such combinations of approaches may be more effective than any single training program for promoting memory performance among older adults, a topic on which future investigation is merited (Hertzog et al., 2008; Studenski et al., 2006). Second, future studies should consider long-term memory benefits that may result from memory training. The ACTIVE study of healthy, community-dwelling older adults has provided evidence of long-term effects of memory training on memory outcomes as far as five years after training (Ball et al., 2002; Willis et al., 2006). However, few studies provide follow-up information beyond one year, and further research is needed to characterize the maintenance of memory training effects over time. Finally, future meta-analytic studies should investigate training effects on more distal measures of everyday functioning or other cognitive domains (e.g., everyday problem-solving, executive functioning, processing speed, language).
Concluding remarks
Public health is confronted with the confluence of three major challenges that will worsen in coming years: a greater number of older adults, rising prevalence of cognitive impairment in older adults, and increasing needs for health and long-term care services to accommodate this growing population segment who will experience cognitive decline. Against the backdrop of this looming predicament, researchers in public health and other fields study interventions that prevent or delay cognitive decline in late life. Memory training offers potential solutions to these public health challenges by helping individuals improve their everyday functioning through memory improvement (Hertzog et al., 2008). Maintenance of memory abilities is essential for the preservation of independence in older adulthood and also an influential factor in determining future care needs. Continued investigation of memory programs and interventions is needed to evaluate the effectiveness and generalizability of memory training interventions across different locations, populations, and age groups (Rebok et al., 2007).
There are several previous influential meta-analyses of memory training (Verhaeghen et al., 1992; Zehnder et al., 2009). Only four studies were in both our review and the one by Verhaeghen and colleagues (Flynn et al., 1990; Scogin et al., 1985; Yesavage et al., 1983, 1984). Two reasons for this lack of overlap are that many of our studies were published after 1992, and that the present review had different, and more stringent, inclusion criteria, per APA guidelines (Weisz & Hawley, 2001). The present review confirms and updates these other reviews and prior research that memory training is effective, and that although no particular strategy may be better than others, there is a trend towards larger improvement after training with more strategies. Consultations with clinicians and caregivers in the use of these training programs are vital to equip aging individuals with beneficial techniques that fit their lifestyles.
Acknowledgments
Dr. Gross was supported by the Johns Hopkins Sommer Scholars Fellowship. Dr. Parisi was supported by the National Institute of Mental Health Prevention Research Training Grant (T32 MH018834). Dr. Ko was supported by the National Institute on Aging Research Training in Age-Related Cognitive Disorders Training Grant (T32 AG027668). Dr. Saczynski was supported by the National Institute on Aging Career Development Award Medical Illness & Cognitive Impairment in Older Adults: Heart Failure as a Model (K01 AG033643). Authors would like to acknowledge Steven Koh, MD, MPH, MBA and Ronald E. Holtzman, Ph.D. for their help reviewing studies. The opinions expressed here are those of the authors and do not necessarily reflect those of the funding, academic, research, or governmental institutions involved.
Footnotes
No authors have any conflicts of interest.
References
References marked with an asterisk indicate studies included in the meta-analysis
- Acevedo A, Loewenstein DA. Nonpharmacological cognitive interventions in aging and dementia. Journal of Geriatric Psychiatry and Neurology. 2007;20:239–249. doi: 10.1177/0891988707308808. [DOI] [PubMed] [Google Scholar]
- *.Andrewes DG, Kinsella G, Murphy M. Using a memory handbook to improve everyday memory in community-dwelling older adults with memory complaints. Experimental Aging Research. 1996;22:305–322. doi: 10.1080/03610739608254013. [DOI] [PubMed] [Google Scholar]
- *.Ball K, Berch DB, Helmers KF, Jobe JB, Leveck MD, Marsiske M, Morris JN, Rebok GW, Smith DM, Tennstedt SL, Unverzagt FW, Willis SL. Effects of cognitive training interventions with older adults: a randomized controlled trial. Journal of the American Medical Association. 2002;288:2271–2281. doi: 10.1001/jama.288.18.2271. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Becker H, McDougall GJ, Douglas NE, Arheart KL. Comparing the efficiency of eight-session versus four-session memory intervention for older adults. Archives of Psychiatric Nursing. 2008;22:87–94. doi: 10.1016/j.apnu.2007.05.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Belleville S. Cognitive training for persons with mild cognitive impairment. International Psychogeriatrics. 2008;20:57–66. doi: 10.1017/S104161020700631X. [DOI] [PubMed] [Google Scholar]
- *.Best DL, Hamlett KW, Davis SW. Memory complaints and memory performance in the elderly: The effects of memory-skills training and expectancy change. Applied Cognitive Psychology. 1992;6:405–416. [Google Scholar]
- Bherer L, Kramer AF, Peterson MS, Colcombe S, Erickson K, Becic E. Testing the limits of cognitive plasticity in older adults: Application to attentional control. Acta Psychologica. 2006;123:261–278. doi: 10.1016/j.actpsy.2006.01.005. [DOI] [PubMed] [Google Scholar]
- Bjorklund DF, Douglas RN. The development of memory strategies. In: Cowan N, editor. The development of memory in childhood. Hove East Sussex: Psychology Press; 1997. pp. 201–246. [Google Scholar]
- Bjorklund DF, Schneider W, Cassel WS, Ashley E. Training and extension of a memory strategy: Evidence for utilization deficiencies in the acquisition of an organizational strategy in high- and low-IQ children. Child Development. 1994;65:951–965. [PubMed] [Google Scholar]
- Bonferroni CE. Studi in Onore del Professore Salvatore Ortu Carboni. Rome: Italy: 1935. Il calcolo delle assicurazioni su gruppi di teste; pp. 13–60. [Google Scholar]
- Bousfield WA. The occurrence of clustering in recall of randomly arranged associates. The Journal of General Psychology. 1953;49:229–240. [Google Scholar]
- Bower GH. Analysis of a mnemonic device. American Scientist. 1970;58:496–510. [Google Scholar]
- Brandt J, Benedict RHB. Hopkins Verbal Learning Test—Revised: Professional manual. Odessa, FL: Psychological Assessment Resources; 2001. [Google Scholar]
- Burden B. The Memory Master method. Dallas, TX: Billy Burden School of Memory & Attitude; 1988. [Google Scholar]
- *.Buschkuehl M, Jaeggi SM, Hutchison S, Perrig-Chiello P, Däpp C, Müller M, Breil F, Hoppeler H, Perrig WJ. Impact of working memory training on memory performance in old-old adults. Psychology and Aging. 2008;23:743–753. doi: 10.1037/a0014342. [DOI] [PubMed] [Google Scholar]
- Cahn-Weiner DA, Malloy PF, Rebok GW, Ott BR. Results of a randomized placebo-controlled study of memory training for mildly impaired Alzheimer’s disease patients. Applied Neuropsychology. 2003;10:215–223. doi: 10.1207/s15324826an1004_3. [DOI] [PubMed] [Google Scholar]
- *.Calero MD, Navarro E. Cognitive plasticity as a modulating variable on the effects of memory training in elderly persons. Archives of Clinical Neuropsychology. 2007;22:63–72. doi: 10.1016/j.acn.2006.06.020. [DOI] [PubMed] [Google Scholar]
- *.Calero-Garcia MD, Navarro-Gonzalez E. Effectiveness of a memory training programme in the maintenance of status in elderly people with and without cognitive decline. Psychology in Spain. 2007;11:106–112. [Google Scholar]
- Camp CJ. Facilitation of new learning in Alzheimer’s disease. In: Gilmore G, Whitehouse P, Wykle M, editors. Memory and aging: Theory, research, and practice. New York: Springer; 1989. pp. 212–225. [Google Scholar]
- *.Caprio–Prevette MD, Fry PS. Memory enhancement program for community–based older adults: Development and evaluation. Experimental Aging Research. 1996;22:281–303. doi: 10.1080/03610739608254012. [DOI] [PubMed] [Google Scholar]
- *.Carretti B, Borella E, De Beni R. Does strategic memory training improve the working memory performance of younger and older adults? Experimental Psychology. 2007;54:311–320. doi: 10.1027/1618-3169.54.4.311. [DOI] [PubMed] [Google Scholar]
- Chambless DL, Hollon SD. Defining empirically supported therapies. Journal of Consulting and Clinical Psychology. 1998;66:7–18. doi: 10.1037//0022-006x.66.1.7. [DOI] [PubMed] [Google Scholar]
- Cherry KE, Simmons-D’Gerolamo SS. Long-term effectiveness of spaced-retrieval memory training for older adults with probable Alzheimer’s Disease. Experimental Aging Research. 2005;31:261–289. doi: 10.1080/03610730590948186. [DOI] [PubMed] [Google Scholar]
- Colcombe S, Kramer AF. Fitness effects on the cognitive function of older adults: A meta-analytic study. Psychological Science. 2003;14:125–130. doi: 10.1111/1467-9280.t01-1-01430. [DOI] [PubMed] [Google Scholar]
- Clare L, Woods RT. Cognitive training and cognitive rehabilitation for people with early-stage Alzheimer disease: A review. Neuropsychological Rehabilitation. 2004;14:385–401. [Google Scholar]
- *.Craik FIM. Encoding and retrieval effects in human memory: A partial review. In: Long JB, editor. Attention and performance. Vol. 9. Hillsdale, NJ: Lawrence Erlbaum Associates Inc; 1981. pp. 383–402. [Google Scholar]
- Craik FIM, Winocur G, Palmer H, Binns MA, Edwards M, Bridges K, et al. Cognitive rehabilitation in the elderly: Effects on memory. Journal of the International Neuropsychological Society. 2007;13:132–142. doi: 10.1017/S1355617707070166. [DOI] [PubMed] [Google Scholar]
- Crawford JR, Stewart LE, Moore JW. Demonstration of savings on the AVLT and development of a parallel form. Journal of Clinical and Experimental Neuropsychology. 1989;11:975–981. doi: 10.1080/01688638908400950. [DOI] [PubMed] [Google Scholar]
- *.Dahlin E, Nyberg L, Bäckman L, Neely AS. Plasticity of executive functioning in young and older adults: Immediate training gains, transfer, and long-term maintenance. Psychology and Aging. 2008;23:720–730. doi: 10.1037/a0014296. [DOI] [PubMed] [Google Scholar]
- De Vreese L, Neri M, Fioravanti M, Belloi L, Zanetti O. Memory rehabilitation in Alzheimer’s Disease: A review of progress. International Journal of Geriatric Psychiatry. 2001;16:794–809. doi: 10.1002/gps.428. [DOI] [PubMed] [Google Scholar]
- Delis DC, Kramer JH, Kaplan E, Ober BA. California Verbal Learning Test. San Antonio, TX: The Psychological Corporation; 1987. [Google Scholar]
- *.Derwinger A, Neely AS, MacDonald S, Bäckman L. Forgetting numbers in old age: Strategy and learning speed matter. Gerontology. 2005;51:277–284. doi: 10.1159/000085124. [DOI] [PubMed] [Google Scholar]
- Desrosiers J, Demers L, Robichaud L, Vincent C, Belleville S, Ska B BRAD Group. Short-term changes in and predictors of participation of older adults after stroke following acute care or rehabilitation. Neurorehabilitation and Neural Repair. 2008;22:288–297. doi: 10.1177/1545968307307116. [DOI] [PubMed] [Google Scholar]
- Dunlap WP, Cortina JM, Vaslow JB, Burke MJ. Meta-analysis of experiments with matched groups or repeated measures designs. Psychological Methods. 1996;1:170–177. [Google Scholar]
- Dunlosky J, Cavallini E, Roth H, McGuire CL, Vecchi T, Hertzog C. Do self-monitoring interventions improve older adult learning? The Journal of Gerontology: Psychological Sciences and Social Sciences. 2007;62:70–76. doi: 10.1093/geronb/62.special_issue_1.70. [DOI] [PubMed] [Google Scholar]
- *.Dunlosky J, Kubat-Silman A, Hertzog C. Training monitoring skills improves older adults’ self-paced associative learning. Psychology and Aging. 2003;18:340–345. doi: 10.1037/0882-7974.18.2.340. [DOI] [PubMed] [Google Scholar]
- Ebbinghaus H. Memory: A contribution to experimental psychology. New York: Dover; 1895/1964. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Erickson KI, Colcombe SJ, Wadhwa R, Bherer L, Peterson MS, Scalf PE, et al. Training-induced plasticity in older adults: Effects of training on hemispheric asymmetry. Neurobiology of Aging. 2007;28:272–283. doi: 10.1016/j.neurobiolaging.2005.12.012. [DOI] [PubMed] [Google Scholar]
- *.Fabre C, Chamari K, Mucci P, Massé-Biron J, Préfaut C. Improvement of cognitive function by mental and/or individualized aerobic training in healthy elderly subjects. International Journal of Sports Medicine. 2002;23:415–421. doi: 10.1055/s-2002-33735. [DOI] [PubMed] [Google Scholar]
- Floyd M, Scogin F. Effects of memory training on the subjective memory functioning and mental health of older adults: A meta-analysis. Psychology and Aging. 1997;12:150–161. doi: 10.1037//0882-7974.12.1.150. [DOI] [PubMed] [Google Scholar]
- *.Flynn TM, Storandt M. Supplemental group discussions in memory training. Psychology and Aging. 1990;5:178–181. doi: 10.1037//0882-7974.5.2.178. [DOI] [PubMed] [Google Scholar]
- Gross AL, Rebok GW. Memory Training and Strategy Use in Older Adults: Results from the ACTIVE Study. Psychology and Aging. 2011;26:503–517. doi: 10.1037/a0022687. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gobet F, Lane PCR, Croker S, Cheng PCH, Jones G, Oliver I, Pine JM. Chunking mechanisms in human learning. Trends in Cognitive Sciences. 2001;5:236–243. doi: 10.1016/s1364-6613(00)01662-4. [DOI] [PubMed] [Google Scholar]
- González-Gross M, Marcos A, Pietrzik K. Nutrition and cognitive impairment in the elderly. The British Journal of Nutrition. 2001;86:313–321. doi: 10.1079/bjn2001388. [DOI] [PubMed] [Google Scholar]
- Gordon B, Berger L. Intelligent Memory. New York: Penguin Books; 2003. [Google Scholar]
- Grandmaison E, Simard M. A critical review of memory stimulation programs in Alzheimer’s disease. Journal of Neuropsychiatry and Clinical Neuroscience. 2003;15:130–144. doi: 10.1176/jnp.15.2.130. [DOI] [PubMed] [Google Scholar]
- Hanley IG, Lusty K. Memory aids in reality orientation: A single–case study. Behaviour Research and Therapy. 1984;22:709–712. doi: 10.1016/0005-7967(84)90134-7. [DOI] [PubMed] [Google Scholar]
- Hazlett EA, Buchsbaum MS, Mohs RC, Spiegel-Cohen J, Wei TC, Azueta R, et al. Age-related shift in brain region activity during successful memory performance. Neurobiology of Aging. 1998;19:437–445. doi: 10.1016/s0197-4580(98)00075-x. [DOI] [PubMed] [Google Scholar]
- Hertzog C, Kramer AF, Wilson RS, Lindenberger U. Enrichment effects on adult cognitive development: Can the functional capacity of older adults be preserved and enhanced? Psychological Science in the Public Interest. 2008;9:1–65. doi: 10.1111/j.1539-6053.2009.01034.x. [DOI] [PubMed] [Google Scholar]
- Heun R, Burkart M, Benkert O. Improvement of picture recall by repetition in patients with dementia of Alzheimer type. International Journal of Geriatric Psychiatry. 1997;12:85–92. doi: 10.1002/(sici)1099-1166(199701)12:1<85::aid-gps470>3.0.co;2-u. [DOI] [PubMed] [Google Scholar]
- Hildebrandt H, Bussmann-Mork B, Schwendemann G. Group therapy for memory impaired patients: A partial remediation is possible. Journal of Neurology. 2006;253:512–519. doi: 10.1007/s00415-006-0013-6. [DOI] [PubMed] [Google Scholar]
- *.Hill RD, Allen C, McWhorter P. Stories as a mnemonic aid for older learners. Psychology and Aging. 1991;6:484–486. doi: 10.1037//0882-7974.6.3.484. [DOI] [PubMed] [Google Scholar]
- Hill RD, Bäckman L, Stigsdotter-Neely A. Cognitive rehabilitation in old age. New York: Oxford University Press; 2000. [Google Scholar]
- *.Hill RD, Campbell BW, Foxley D, Lindsay S. Effectiveness of the number-consonant mnemonic for retention of numeric material in community-dwelling older adults. Experimental Aging Research. 1997;23:275–286. doi: 10.1080/03610739708254284. [DOI] [PubMed] [Google Scholar]
- *.Hill RD, Storandt M, Simeone C. The effects of memory skills training and incentives on free recall in older learners. Journal of Gerontology. 1990;45:227–232. doi: 10.1093/geronj/45.6.p227. [DOI] [PubMed] [Google Scholar]
- Howe ML, Brainerd CJ, Kingma J. Development of organization in recall: A stages–of–learning analysis. Journal of Experimental Child Psychology. 1985;39:230–251. [Google Scholar]
- Hunt EB, Love T. How good can memory be? In: Melton A, Martin E, editors. Coding process in human memory. Washington: V.H: Winston & Sons; 1972. [Google Scholar]
- Kennedy BA, Miller DJ. Persistent use of verbal rehearsal as a function of information about its value. Child Development. 1976;47:566–569. [Google Scholar]
- Kliegl R, Smith J, Baltes PB. Testing the limits and the study of adult age differences in cognitive plasticity of a mnemonic skill. Developmental Psychology. 1989;25:247–256. [Google Scholar]
- Kliegl R, Smith J, Baltes PB. On the locus and process of magnification of age differences during a mnemonic training. Developmental Psychology. 1990;26:894–904. [Google Scholar]
- Lachman ME, Weaver SL, Bandura M, Elliott E, Lewkowicz CJ. Improving memory and control beliefs. Journal of Gerontology. 1992;47:293–299. doi: 10.1093/geronj/47.5.p293. [DOI] [PubMed] [Google Scholar]
- *.Lustig C, Flegal KE. Targeting latent function: encouraging effective encoding for successful memory training and transfer. Psychology and Aging. 2008;23:754–764. doi: 10.1037/a0014295. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mahncke HW, Bronstone A, Merzenich MM. Memory enhancement in healthy older adults using a brain plasticity-based training program: A randomized, controlled study. Proceedings of the National Academy of Sciences. 2006;103:12523–12528. doi: 10.1073/pnas.0605194103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mandler G. Organization and memory. In: Spence KW, Spence KT, editors. The psychology of learning and motivation. New York: Academic Press; 1967. pp. 327–372. [Google Scholar]
- Martin M, Clare L, Altgassen AM, Cameron MH, Zehnder F. Cognition-based interventions for healthy older people and people with mild cognitive impairment. Cochrane Database of Systematic Reviews. 2011;(1) doi: 10.1002/14651858.CD006220.pub2. Art No.: CD006220. [DOI] [PubMed] [Google Scholar]
- McDaniel MA, Einstein GO, Jacoby LJ. New considerations in aging and memory. In: Craik FIM, Salthouse TA, editors. The handbook of aging and cognition. 4. London: Academic Press; 2008. pp. 251–310. [Google Scholar]
- McDougall GJ. Memory self-efficacy and memory performance among Black and White elders. Nursing Research. 2004;53:323–331. doi: 10.1097/00006199-200409000-00007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.McDougall GG, Becker H, Pituch K, Vaughan P, Acee T, Delville C. The SeniorWISE study: Improving everyday memory in older adults. Archives of Psychiatric Nursing. 2010 doi: 10.1016/j.apnu.2009.11.001. Published online 15 January 2010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McKitrick LA, Camp CJ, Black FW. Prospective memory intervention in Alzheimer’s disease. Journal of Gerontology. 1992;47:337–343. doi: 10.1093/geronj/47.5.p337. [DOI] [PubMed] [Google Scholar]
- McPherson A, Furniss FG, Sdogati C, Cesaroni F, Tartaglini B, Lindes A. Effects of individualized memory aids on the conversation of persons with severe dementia: A pilot study. Aging and Mental Health. 2001;5:289–294. doi: 10.1080/13607860120064970. [DOI] [PubMed] [Google Scholar]
- Mitrushina M, Boone KB, Razani J, D’Elia LF. Handbook of normative data for neuropsychological assessment. New York: Oxford University Press; 2005. [Google Scholar]
- *.Mohs RC, Ashman TA, Jantzen K, Albert M, Brandt J, Gordon B, Rasmusson DX, Grossman M, Jacobs D, Stern Y. A study of the efficacy of a comprehensive memory enhancement program in healthy elderly persons. Psychiatry Research. 1998;77:183–195. doi: 10.1016/s0165-1781(98)00003-1. [DOI] [PubMed] [Google Scholar]
- Morrell RW, Rager R, Harley JP, Herrmann DJ, Rebok GW, Parente R. Developing an online intervention for memory improvement: The sharper memory project. Cognitive Technology. 2006;11:34–46. [Google Scholar]
- Nolan BA, Mathews RM, Harrison M. Using external memory aids to increase room finding by older adults with dementia. American Journal of Alzheimers Disease and Other Dementias. 2001;16:251–254. doi: 10.1177/153331750101600413. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nyberg L, Sandblom J, Jones S, Neely AS, Petersson KM, Ingvar M, Bäckman L. Neural correlates of training-related memory improvement in adulthood and aging. Proceedings of the National Academy of Sciences. 2003;100:13728–13733. doi: 10.1073/pnas.1735487100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ornstein PA, Naus MJ. Rehearsal processes in children’s memory. In: Ornstein PA, editor. Memory development in children. Hillsdale, NJ: Erlbaum; 1978. [Google Scholar]
- Owen AM, Hampshire A, Grahn JA, Stenton R, Dajani S, Burns AS, Howard RJ, Ballard CG. Putting brain training to the test. Nature. 2010;465:775–778. doi: 10.1038/nature09042. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Poon LW, Walsh–Sweeney L, Fozard J. Memory skill training in the elderly: Salient issues on the use of mnemonics. In: Poon LW, Fozard JL, Cermak LS, Arenberg D, Thompson LW, editors. Proceedings of the George A Talland memorial conference. Lawrence Erlbaum Associates; Hillsdale, NJ: 1980. p. 461. [Google Scholar]
- Rankin JL, Karol R, Tuten C. Strategy use, recall, and recall organization in young, middle-aged, and elderly adults. Experimental Aging Research. 1984;10:193–196. doi: 10.1080/03610738408258463. [DOI] [PubMed] [Google Scholar]
- *.Rapp S, Brenes G, Marsh AP. Memory enhancement training for older adults with mild cognitive impairment: A preliminary study. Aging & Mental Health. 2002;6:5–11. doi: 10.1080/13607860120101077. [DOI] [PubMed] [Google Scholar]
- Rasmusson DX, Rebok GW, Bylsma FW, Brandt J. Effects of three types of memory training in normal elderly. Aging, Neuropsychology, and Cognition. 1999;6:56–66. [Google Scholar]
- Rebok GW, Balcerak LJ. Memory self-efficacy and performance differences in young and old adults: Effect of mnemonic training. Developmental Psychology. 1989;25:714–721. [Google Scholar]
- Rebok GW, Carlson MC, Langbaum JBS. Training and maintaining memory abilities in healthy older adults: Traditional and novel approaches. Journal of Gerontology. 2007;62B:53–61. doi: 10.1093/geronb/62.special_issue_1.53. [DOI] [PubMed] [Google Scholar]
- Rebok GW, Parisi JM, Gross AL, Ko J, Spira AP, Samus QM, Saczynski JS, Koh S, Holtzman RE. Evidence-based psychological treatments for improving memory function among older adults. In: Scogin F, Shah A, editors. Making Evidence-Based Psychological Treatments Work with Older Adults. Washington, DC: American Psychological Association; in press. [Google Scholar]
- Rey A. L’examen clinique en psychologie. Paris: Presses Universitaires de France; 1964. [Google Scholar]
- Richardson JT. The availability and effectiveness of reported mediators in associative learning: A historical review and an experimental investigation. Psychonomic Bulletin & Review. 1998;5:597–614. [Google Scholar]
- Rozzini L, Costardi D, Chilovi BV, Franzoni S, Trabucchi M, Padovani A. Efficacy of cognitive rehabilitation in patients with mild cognitive impairment treated with cholinesterase inhibitors. International Journal of Geriatric Psychiatry. 2007;22:356–360. doi: 10.1002/gps.1681. [DOI] [PubMed] [Google Scholar]
- Salthouse TA. Influence of age on practice effects in longitudinal neurocognitive change. Neuropsychology. 2010;24:563–572. doi: 10.1037/a0019026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Salthouse TA, Tucker-Drob EM. Implications of short-term retest effects for the interpretation of longitudinal change. Neuropsychology. 2008;22:800–811. doi: 10.1037/a0013091. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schmidt IW, Berg IJ, Deelman BG. Prospective memory training in older adults. Educational Gerontology. 2001;27:455–478. [Google Scholar]
- Schneider W, Sodian B. A longitudinal study of young children’s memory behaviour and performance in a sort-recall task (Paper 5) Munich, Germany: Max-Planck-Institut für Psychologische Forschung; 1988. [Google Scholar]
- *.Scogin F, Prohaska M. The efficacy of self-taught memory training for community-dwelling older adults. Educational Gerontology. 1992;18:751–766. [Google Scholar]
- *.Scogin F, Prohaska M, Weeks E. The comparative efficacy of self–taught and group memory training for older adults. Journal of Clinical Geropsychology. 1998;4:301–314. [Google Scholar]
- *.Scogin F, Storandt M, Lott L. Memory-skills training, memory complaints, and depression in older adults. Journal of Gerontology. 1985;40:562–568. doi: 10.1093/geronj/40.5.562. [DOI] [PubMed] [Google Scholar]
- Shapiro DM, Harrison DW. Alternate forms of the AVLT: a procedure and test of form equivalency. Archives of Clinical Neuropsychology. 1990;5:405–410. [PubMed] [Google Scholar]
- Sharps MJ, Price-Sharps JL. Visual memory support: An effective mnemonic device for older adults. The Gerontologist. 1996;36:706–708. doi: 10.1093/geront/36.5.706. [DOI] [PubMed] [Google Scholar]
- Singer T, Lindenberger U, Baltes PB. Plasticity of memory for new learning in very old age: a story of major loss? Psychology and Aging. 2003;18:306–317. doi: 10.1037/0882-7974.18.2.306. [DOI] [PubMed] [Google Scholar]
- Sitzer DI, Twamley EW, Jeste DV. Cognitive training in Alzheimer’s Disease: A meta-analysis of the literature. Acta Psychiatrica Scandinavia. 2006;114:75–90. doi: 10.1111/j.1600-0447.2006.00789.x. [DOI] [PubMed] [Google Scholar]
- Small G. The Memory Bible. New York: Hyperion; 2002. [Google Scholar]
- *.Smith GE, Housen P, Yaffe K, Ruff R, Kennison RF, Mahncke HW, Zelinski EM. A cognitive training program based on principles of brain plasticity: results from the Improvement in Memory with Plasticity-based Adaptive Cognitive Training (IMPACT) study. Journal of Geriatric Psychiatry. 2009;57:594–603. doi: 10.1111/j.1532-5415.2008.02167.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- StataCorp. Stata Statistical Software: Release 11. College Station, TX: StataCorp LP; 2010. [Google Scholar]
- Stern Y. What is cognitive reserve? Theory and research application of the reserve concept. Journal of the International Neuropsychological Society. 2002;8:448–460. [PubMed] [Google Scholar]
- *.Stigsdotter A, Bäckman L. Multifactorial memory training with older adults. Gerontology. 1989;35:260–267. doi: 10.1159/000213035. [DOI] [PubMed] [Google Scholar]
- Storandt M. Memory-skills training for older adults. Nebraska Symposium on Motivation. 1991;39:39–62. [PubMed] [Google Scholar]
- Studenski S, Carlson MC, Fillit H, Greenough WT, Kramer A, Rebok GW. From bedside to bench: Does mental and physical activity promote cognitive vitality in late life? Science of Aging Knowledge Environment. 2006:21. doi: 10.1126/sageke.2006.10.pe21. [DOI] [PubMed] [Google Scholar]
- Tárraga L, Boada M, Modinos G, Espinosa A, Diego S, Morera A, Guitart M, Balcells J, López OL, Becker JT. A randomised pilot study to assess the efficacy of an interactive, multimedia tool of cognitive stimulation in Alzheimer’s disease. Journal of Neurology, Neurosurgery & Psychiatry. 2006;77:1116–1121. doi: 10.1136/jnnp.2005.086074. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Taulbee LR, Folsom JC. Reality orientation for geriatric patients. Hospital & Community Psychiatry. 1966;17:133–135. doi: 10.1176/ps.17.5.133. [DOI] [PubMed] [Google Scholar]
- Troyer AK, Murphy KJ, Anderson ND, Moscovitch M, Craik FIM. Changing everyday memory behaviour in amnestic mild cognitive impairment: a randomised controlled trial. Neuropsychological Rehabilitation. 2008;18:65–88. doi: 10.1080/09602010701409684. [DOI] [PubMed] [Google Scholar]
- Verhaeghen P, Marcoen A. On the mechanisms of plasticity in young and older adults after instruction in the method of loci: Evidence for an amplification model. Psychology and Aging. 1996;11:164–178. doi: 10.1037//0882-7974.11.1.164. [DOI] [PubMed] [Google Scholar]
- Verhaeghen P, Marcoen A, Goossens L. Improving memory performance in the aged through mnemonic training: A meta-analytic study. Psychology and Aging. 1992;7:242–251. doi: 10.1037//0882-7974.7.2.242. [DOI] [PubMed] [Google Scholar]
- Weisz JR, Hawley KM. Procedural and coding manual for identification of evidence-based treatments. Los Angeles: University of California; 2001. [Google Scholar]
- West R. Memory fitness over 40. Gainesville, FL: Triad Publishing; 1985. [Google Scholar]
- Willis SL, Tennstedt SL, Marsiske M, Ball K, Elias J, Koepke KM, Morris JN, Rebok GW, Unverzagt FW, Stoddard AM, Wright E. Long-term effects of cognitive training on everyday functional outcomes in older adults. Journal of the American Medical Association. 2006;296:2805–2814. doi: 10.1001/jama.296.23.2805. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wilson B, Cockburn J, Baddeley A. The Rivermead Behavioural Memory Test. Bury St Edmunds, England: Thames Valley Test Company; 1985. [Google Scholar]
- Wolters G, Theunissen I, Bemelmans KJ, van der Does AJW, Spinhoven P. Immediate and intermediate-term effectiveness of a memory training program for the elderly. Journal of Cognitive Rehabilitation. 1996;14:16–22. [Google Scholar]
- Woods B, Thorgrimsen L, Spector A, Royan L, Orrell M. Improved quality of life and cognitive stimulation therapy in dementia. Aging and Mental Health. 2006;10:219–226. doi: 10.1080/13607860500431652. [DOI] [PubMed] [Google Scholar]
- *.Woolverton M, Scogin F, Shackelford J, Black S, Duke L. Problem-targeted memory training for older adults. Aging, Neuropsychology, and Cognition. 2001;8:241–255. [Google Scholar]
- Worthen JB, Hunt RR. Mnemonology: Mnemonics for the 21st century. Hove East Sussex: Psychology Press; 2011. [Google Scholar]
- Yates FA. The art of memory. Chicago: University of Chicago Press; 1966. [Google Scholar]
- Yesavage JA, Hoblyn J, Friedman L, Mumenthaler M, Schnieder B, O’Hara R. Should one use medications in combination with cognitive training? If so, which ones? Journal of Gerontology: Psychological Sciences and Social Sciences. 2007;62:11–18. doi: 10.1093/geronb/62.special_issue_1.11. [DOI] [PubMed] [Google Scholar]
- *.Yesavage JA. Imagery pretraining and memory training. Gerontology. 1983;29:271–275. doi: 10.1159/000213126. [DOI] [PubMed] [Google Scholar]
- *.Yesavage JA. Relaxation and memory training in 39 elderly patients. American Journal of Psychiatry. 1984;141:778–781. doi: 10.1176/ajp.141.6.778. [DOI] [PubMed] [Google Scholar]
- Yesavage JA, Sheikh JI, Friedman L, Tanke E. Learning mnemonics: Roles of aging and subtle cognitive impairment. Psychology and Aging. 1990;5:133–137. doi: 10.1037//0882-7974.5.1.133. [DOI] [PubMed] [Google Scholar]
- Yu F, Rose KM, Burgener SC, Cunningham C, Buettner LL, Beattie E, Bossen AL, Buckwalter KC, Fick DM, Fitzsimmons S, Kolanowski A, Janet K, Specht P, Richeson NE, Testad I, McKenzie SE. Cognitive training for early-stage Alzheimer’s Disease and dementia. Journal of Gerontological Nursing. 2009;35:23–29. doi: 10.3928/00989134-20090301-10. [DOI] [PubMed] [Google Scholar]
- Zanetti O, Binetti G, Magni E, Rozzini L, Bianchetti A, Trabucchi M. Procedural memory stimulation in Alzheimer’s disease: Impact of a training programme. Acta Neurologica Scandinavia. 1997;95:152–157. doi: 10.1111/j.1600-0404.1997.tb00087.x. [DOI] [PubMed] [Google Scholar]
- Zarit SH, Cole KD, Guider RL. Memory training strategies and subjective complaints of memory in the aged. The Gerontologist. 1981;21:158–164. doi: 10.1093/geront/21.2.158. [DOI] [PubMed] [Google Scholar]
- Zehnder F, Martin M, Altgassen M, Clare L. Memory training effects in old age as markers of plasticity: A meta-analysis. Restorative Neurology and Neuroscience. 2009;27:507–520. doi: 10.3233/RNN-2009-0491. [DOI] [PubMed] [Google Scholar]