

Abstract
There is no standardized dysphagia therapy for head and neck cancer patients and scant evidence to support any particular protocol, leaving institutions and individual speech language pathologists (SLPs) to determine their own protocols based on “typical” practices or anecdotal evidence. To gain an understanding of current usual practices, a national internet-based survey was developed and disseminated to SLPs who treat HNC patients. From a random sample of 4,000 ASHA SID 13 members, 1,931 fit the inclusion criteria, and 759 complete responses were recorded for a 39.3% response rate. Results were analyzed by institution type as well as by individual clinical experience. While some interesting trends emerged from the data, a lack of uniformity and consensus regarding best practices was apparent. This is undoubtedly due to a paucity of research adequately addressing the efficacy of any one therapy for dysphagia in the HNC population.
Keywords: deglutition, deglutition disorders, head and neck cancer, dysphagia therapy, usual care
INTRODUCTION
Rehabilitation of dysphagia has historically been delivered after insult to the system, whether that insult is surgery, neurologic disease, or another condition that has impaired the swallow. Treatment techniques include compensatory and rehabilitative methods, employed based on anticipated benefit from either approach. The same premise holds for head and neck cancer (HNC) patients who have had surgery as their primary treatment. Over the years, however, as radiation therapy (RT) has become more common in the treatment of head and neck malignancies, optimal timing and best treatment techniques for dysphagia have come into question. Unlike the surgical patient, the onset of a radiation induced dysphagia is unpredictable. Some patients never develop dysphagia, others develop a dysphagia during or soon after RT, and some patients do well for years and then report a worsening in their swallow.
In response to these observations, some SLPs (or the institutions they work for) have adopted a preventative approach to this potential problem, while others choose to wait and see if a dysphagia develops in consideration of the myriad of other priorities the patient manages during RT. Three non-randomized clinical trials have reported outcomes of early intervention (during RT) on swallow function post RT in HNC patients. Two of these studies reported a positive effect on swallowing after RT. However, the other trial reported no benefit to early intervention (1-3).
Efficacy (level 1 evidence) of any particular type of dysphagia therapy has not been established in this patient population, but there are a few studies that suggest treatment effect (level 2-4 evidence). Some patients appear to do well without any therapy while others manage well with only compensatory techniques (4). Some studies suggest that there may be benefit from electrical stimulation (5), Shaker’s exercise (6, 7), or traditional exercise therapy (6). Unfortunately, these studies were either preliminary, included a mixed group of patients (stroke, neurologic, HNC, etc), or the timing, intensity, and duration of therapy were variable.
Not surprisingly, best practice guidelines for HNC patients who undergo radiation therapy have not been published. A recent systematic review published in collaboration with the American Speech-Language-Hearing Association (ASHA) and the Department of Veterans Affairs (DVA) concluded that evidence is limited regarding the effects of any particular posture or maneuver in treating dysphagia in HNC (8). Most importantly, there were very few studies that looked at HNC patients in isolation and even fewer that looked at HNC patients following RT as compared to HNC patients following surgery. Because of the unique nature of this population and the unique pathophysiology involved in their dysphagia, results from other patient populations, including HNC patients treated with surgery only, may not generalize to patients who received RT.
With such limited evidence to guide practice, clinicians must rely on the few published articles that are available, their own anecdotal evidence, reports from so-called experts, and their institution’s historical patterns of treatment. Many decisions need to be made: 1. Should patients be put into therapy before a dysphagia begins or should it wait until a dysphagia develops? 2. If preventative therapy is offered, should it begin during RT or wait until the acute effects of RT are over? 3. How aggressive should the therapy be? 4. How long should the therapy last? 5. Are certain therapies more effective than others?
In response to these unanswered questions, a survey of practicing SLPs was conducted to determine prevalent practice patterns when working with HNC patients who underwent RT. It is important to understand “usual care” in order to move the field towards an evidence-based standard of care.
METHODS
In order to evaluate the usual practices of SLPs who treat HNC patients, an internet-based questionnaire was administered from October 5th to November 1st, 2010. Surveyed participants were drawn from the Special Interest Division 13 (SID13) membership directory of the American Speech-Language Hearing Association (ASHA) which contains listings for roughly 6,700 SLPs with interests in swallowing disorders. From this directory, 4,000 listings were randomly selected by using Microsoft Excel Analysis ToolPak’s Random Number Generator.
Of the 4000 randomly selected listings, individuals were excluded for the following reasons: a) their location was listed as outside of the United States and its territories, b) their employment facility was unlikely to treat HNC patients (ie. pediatric hospital, various school based settings), c) their listing was incomplete or d) the algorithm selected the same listing more than once. After this initial exclusion, 2,207 individuals remained. Of these, 276 had a missing or invalid email addresses. A final sample of 1,931 SLPs received an invitation to complete our web-based survey.
The survey was prepared on SurveyMonkey’s online interface (www.SurveyMonkey.com). Personalized email invitations with direct links to the survey were sent using SurveyMonkey’s Email Invitation Collector system which allowed the research team to maintain anonymity while tracking non-respondents. If an individual had previously opted out of emails from Survey Monkey, invitations were sent using a Boston Medical Center email address. One reminder email with a link to the survey was sent on October 12th, exactly one week after the initial invitation, and one final reminder was sent on October 20th. No compensation was offered to respondents, however those who wished could submit their email address to be entered into a raffle for a $20 gift card as well to receive a preliminary summary of the survey results. To maintain anonymity, the last page of the survey provided a link to an entirely independent survey which allowed users to enter their email addresses without linking their personal information to their responses in the primary survey.
Survey Questions
The survey contained 19 multiple choice questions, including one with the option to write in a response. All questions required a response to continue to the next question. There were three skip logic questions in which more detailed follow-up questions were skipped if the respondent previously indicated that a question did not pertain to their practice.
The first three questions inquired about the clinician’s work place and referral policies. Question number 4 asked the clinician when they generally began to intervene with dysphagia therapy for HNC patients. Questions 5-13 focused on the type, duration, and intensity of the clinician’s typical treatment protocol for any patients that they see a) during RT, b) after completion of RT who have no, or clinically insignificant dysphagia, and c) after completion of RT who have developed a dysphagia. Types of treatment were categorized as Compensatory techniques (e.g. position changes, bolus consistency changes, liquid wash), Stretches (e.g. neck, jaw, tongue), Non-swallow exercise (e.g. tongue base exercises, laryngeal exercises, pharyngeal exercises, Shaker), Swallow Maneuver Exercises (e.g. Mendelsohn, Effortful Swallow, Super Supraglottic), and Other Therapies that could be done by either the SLP or by other professionals (e.g. E-stim, massage or other soft tissue manipulation, acupuncture, lymphedema therapy). Duration of prescribed therapy was defined as days per week, and Intensity of prescribed therapy was defined as minutes per day.
Questions 14 and 15 asked about perceived compliance with dysphagia therapy programs prescribed to dysphagic and non-dysphagic patients while questions 16 and 17 asked about feeding tube policies and recommendations. The final two questions (18 and 19) asked what percent of the clinicians’ case load consists of head and neck cancer patients, and how many years they have worked with swallowing disorders in this patient population. The survey questions can be found in Appendix 1.
Analytical Decisions, Definitions, & Stratifications
Analytical Overview
There were many ways in which this data could have been analyzed, but two most meaningful ways were chosen. The first was to analyze the data by type of institution since different institutions may have access to different types of resources or personnel. The second was to analyze the data by clinician experience – specifically the number of years that a clinician has worked with head and neck cancer patients. The rationale behind the latter perspective was that prolonged work with this difficult to treat patient population may entice clinicians to either delve into the literature in search of studies supporting treatment efficacy, or to be more experimental with varying treatments in an attempt to find the “best” therapy program.
First Intervention
SLPs surveyed were asked when they generally first intervene with any type of dysphagia therapy (question 4). The choices differed in both timing of therapy and type of patient (see Table 1). While intervention times may depend on a number of factors – patient, circumstance, institutional policies, staffing, etc. – the participants were forced to choose one best answer to gauge general trends.
Table 1.
Usual First Interventions
| Timing – Patient Population | % of Respondents |
|---|---|
| 1. Before RT – with all patients | 13.3% |
| 2. Before RT – only with those patients who are motivated or complaining of difficulty swallowing |
10.8% |
| 3. During RT – with all patients | 5.0% |
| 4. During RT – only with those patients who are motivated or complaining of difficulty swallowing |
19.1% |
| 5. In first 3 months after RT – with all patients | 4.6% |
| 6. In first 3 months after RT – only with those patients who are motivated or complaining of difficulty swallowing |
28.6% |
| 7. After 3 months post RT – with all patients | 0.3% |
| 8. After 3 months post RT – only with those patients who are motivated or complaining of difficulty swallowing |
18.3% |
Since the answers were extremely varied, the responses were reduced into two distinct groups for further analysis: Proactive Therapy vs. Reactive Therapy. Proactive Therapy was strictly defined as intervening with all patients, before or during radiation therapy (responses 1 & 3). Reactive Therapy was strictly defined as intervening only if patients develop a dysphagia after completion of radiation therapy (responses 6 & 8).
Usual Practices
Determining “usual treatment” practices (questions 5-13) among SLPs who treat head and neck cancer patients for dysphagia is difficult since there are many variables impacting the type, duration, and intensity of treatment. Intuitively patients who are symptomatic would not only need more aggressive therapy, but may also be more motivated to comply with aggressive recommendations. Conversely, patients undergoing RT are often in pain, and are preoccupied with the myriad of medical appointments associated with their treatment regimen. As a result, usual practices were analyzed independently for three different populations: a) patients receiving prophylactic care during radiation therapy, b) patients who have completed RT and have no or mild dysphagia, and c) patients who have completed RT but have a moderate to severe dysphagia.
For each of these three patient populations, the surveyed SLPs were asked if they recommended any treatment. If treatment was recommended, then the type, frequency, and intensity of treatment were also evaluated. The treatment options (previously described) included compensatory techniques, stretches for range of motion, non-swallow exercises, swallow exercises, and other therapies that might be less conventional or less established. Respondents were allowed to select more than one type of therapy. Frequency was recorded in days per week, and intensity was recorded in minutes per day.
Statistics
All data management and statistical analyses were performed using SAS version 9.2. Frequencies were automatically performed by SurveyMonkey but repeated for validation purposes in SAS. Univariate logistic regression was used to test associations. Survey questions were divided by response levels to create dichotomous variables for testing purposes (i.e., subjects who responded they worked for Academic Teaching Hospitals versus all other subjects who provided a response to the question). Odds ratios were unadjusted.
RESULTS
From the 1,931 SLPs who were sent our survey, 793 responses were collected representing an initial 41.1% response rate. Of the 793 responses, 34 were excluded because they answered only the first three questions, which were concerned only with institutional demographics and policies and not with usual care practices. This left 759 usable responses (39.3%) that were ultimately included in the final analysis.
Clinical Setting & Experience
Respondents represented a variety of clinical settings, the largest number primarily working in Urban or Suburban Non-Teaching Hospitals (28.7%), Academic Teaching Hospitals (27.8%), and Skilled Nursing Facilities (25.0%). Since these institutions largely represent where HNC patients are seen as well as where the majority of respondents work, these three cohorts were of greatest interest to this study. However, several other clinical settings were represented as seen in Table 2.
Table 2.
Respondent Demographics
| Demographics | % of Respondents |
|---|---|
| Clinical Setting (N=759) | |
| % Academic Teaching Hospital | 27.8 |
| % Specialized Cancer Center | 0.9 |
| % Urban or Suburban Non-Teaching Hospital | 28.7 |
| % Rural Hospital | 10.0 |
| % Skilled Nursing Facility | 25.0 |
| % Private Practice | 2.9 |
| % Home Care | 4.6 |
| Years Working w/ HNC Patients (N=720) | |
| % Less than 1 year | 4.3 |
| % 1 to 4 years | 26.1 |
| % 5 to 10 years | 29.7 |
| % More than 10 years | 39.9 |
| Percent of Patients with HNC (N=720) | |
| % 25 Percent or less | 88.3 |
| % 33 Percent | 8.2 |
| % 50 Percent | 2.5 |
| % 67 Percent | 0.7 |
| % 75 Percent or more | 2.4 |
The sample represented SLPs with a range of HNC work experience. Roughly one quarter (26.1%) reported 1-4 years of experience, nearly one third (29.7%) reported 5-10 years of experience, and 39.9% reported over 10 years of experience. Only 4.3% reported less than 1 year of experience working with head and neck cancer patients. Of note, the overwhelming majority of the respondents do not primarily see head and neck cancer patients. Only 5.6% reported that 50% or more of their case load is comprised of head and neck cancer patients.
Institutional Policy & Referrals
Usual practices among healthcare providers are often guided by institutional protocols or directives. When asked what the institutional policy was for referring HNC patients going through RT, it was evident that most SLPs worked in institutions without any policy for referring these patients to speech pathologists. Of the respondents, 70.6% reported that “There is no institutional policy or referrals are made on a case-by-case basis.” Of those who responded that a policy did exist, two-thirds answered that the policy was wait to refer patients until a dysphagia presents, rather than automatically refer regardless of swallow status. These national patterns were similar across institution type except for Stand-Alone Cancer Centers, most of which had automatic referral policies.
Timing of First Intervention
The results suggested that, regardless of reason (institutional protocol, referrals, time, staffing, etc.), many more SLPs intervened reactively rather than proactively. Nearly half of all SLPs first intervened only after a dysphagia developed post-RT compared to only 18.3% who intervened proactively. Interestingly, no one institution was statistically more likely than the others to fall into either the proactive or reactive group, suggesting this trend was independent of institution type. Years of experience working with HNC patients did, however, correlate significantly with time of intervention. SLPs with 5 or more years of experience were three and a half times more likely to act proactively than SLPs with less than 5 years of experience (p=0.0096).
Usual Practices for Dysphagia Therapy
Treatment During RT
As stated above, only 18.3% of SLPs typically intervene proactively. But the majority of all SLPs (approximately 70%) say that they prescribe some sort of therapy program if a patient is referred to them during RT. Only 30% of SLPs reported they do not typically recommend any treatment during radiation therapy if a patient is referred to them at that time. Of those who did recommend dysphagia therapy, most respondents prescribed more than one type of treatment, but the most popular answer were compensatory maneuvers (64.6%). Approximately 50% recommended one or more of the other established treatments: stretches (49.1%), non-swallow exercises (54.8%), and swallow exercises (51.8%). [Figure 1]
Figure 1.
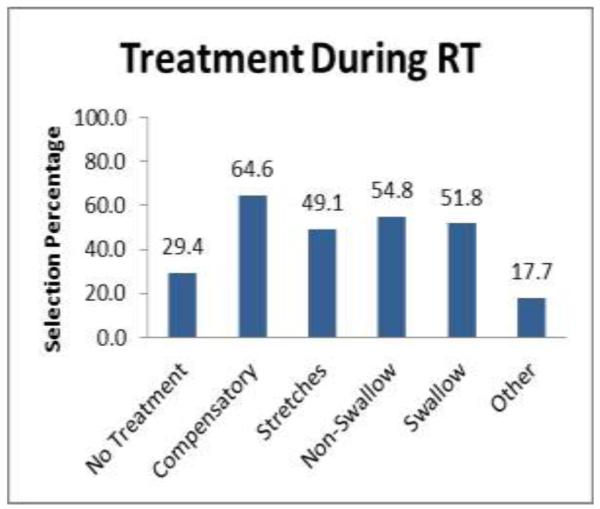
Treatment recommendations for patients during RT. (N=752)
When analyzing the answers by setting, SLPs at skilled nursing facilities were significantly more likely to recommend therapy during RT as compared to all other SLPs. They were 1.5 to 2 times more likely to recommend compensatory techniques (p=0.0171), stretches (p=0022), non-swallow exercises (p=0.0111), and swallow exercises (p<0.0001) as compared to other SLPs. When analyzing the results by clinical experience (independent of setting), the difference was even more pronounced. SLPs with five or more years experience were 5 times more likely to recommend some type of dysphagia therapy during RT than SLPs with less than 5 years of experience (p=0.0351). Of clinicians who recommended dysphagia therapy during RT, SLPs with five or more years of experience were 3.7 to 10.3 times more likely to recommend any of the aforementioned interventions than SLPs with less than 5 years of experience (p=0017-0.0369).
Treatment after RT for Patients with No or Mild Dysphagia
For patients who developed only mild or clinically insignificant dysphagia following RT, there was again, no clear concurrence on what kind of therapy should be recommended, or if therapy should be recommended at all. Over half of the respondents (52.6%) did not recommend any treatment protocol for this group of patients [Figure 2]. Interestingly, SLPs who did recommend dysphagia therapy only recommended, on average, two of the five treatment options (but not necessarily the same two treatments). Stretches and non-swallow exercises were the most popular but no clear consensus existed.
Figure 2.
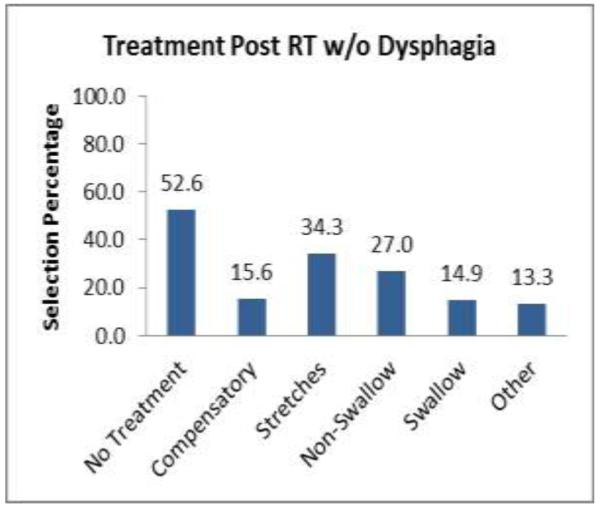
Treatment recommendations after RT for patients with mild or clinically insignificant dysphagia. (N=745)
Skilled nursing facility SLPs were more likely than SLPs at other institutions to prescribe some sort of dysphagia therapy to patients who had no or mild dysphagia after completion of RT (p=0.0115). They were about twice as likely as other SLPs to recommend stretches, non-swallow exercises, and swallow exercises. Years of experience did not statistically predict whether a SLP would recommend treatment to this group of patients. However, of the clinicians who did recommend some sort of dysphagia intervention, the more experienced SLPs recommend swallow exercises (p=0.0206) and non-swallow exercises (p=0.0427) more often than clinicians with less than 5 years of experience.
Treatment after RT for Patients with Moderate to Severe Dysphagia
When patients did develop a significant dysphasia after radiation therapy, the overall treatment response changed drastically [Figure 3]. Treatment protocols became much more aggressive, and the number of dysphagia therapies the average SLP recommended increased from 2 to approximately 4.
Figure 3.
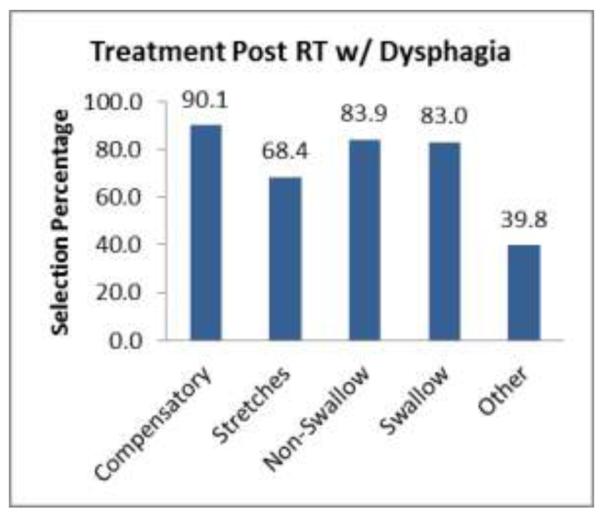
Treatment recommendations after RT for patients with moderate to severe dysphagia. (N=738) recommended for patients during RT. (N=728)
For dysphagic HNC patients, 9 out of 10 SLPs recommended compensatory maneuvers, and in every institutional setting nearly 80% or more recommended swallow and non-swallow exercises. Even the number of respondents recommending “other therapies” almost tripled to 39.8% as compared to patients without dysphagia. When comparing differences in traditional therapy recommendations between institutions, no single institution (with one exception) was statistically most likely to recommend a particular treatment as compared to other institutions. Similarly, with only one exception, there was no significant difference between SLPs with more or less than five years of experience. Overall, there was no meaningful difference in what type of therapy various clinicians prescribed when working with patients presenting with moderate to severe dysphagia.
Frequency and Intensity
Frequency & Intensity for Patients during RT
A little over 70% of all surveyed SLPs reported that they would recommend some sort of therapy program to a patient referred to them during RT. Nearly 50% of all survey SLPs would prescribe 7 days/week therapy programs [Figure 4] and for 10-20 minutes per day [Figure 5]. Only a small percentage recommended less than 10 minutes per day and for 2-3 days per week.
Figure 4.
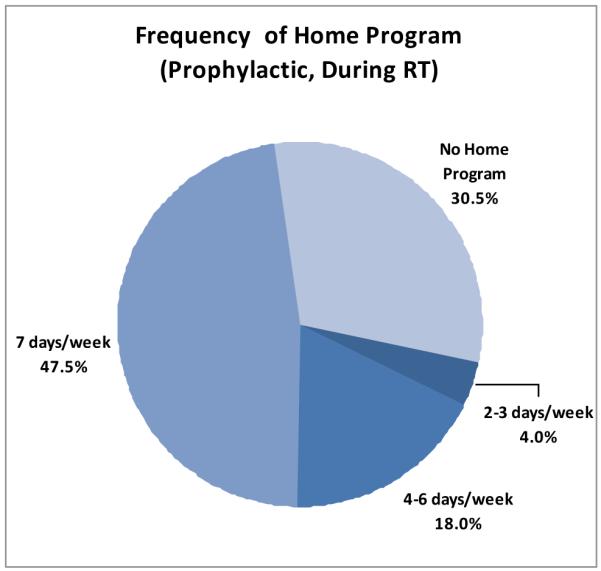
Frequency of home therapy programs recommended for patients during RT. (N=728)
Figure 5.
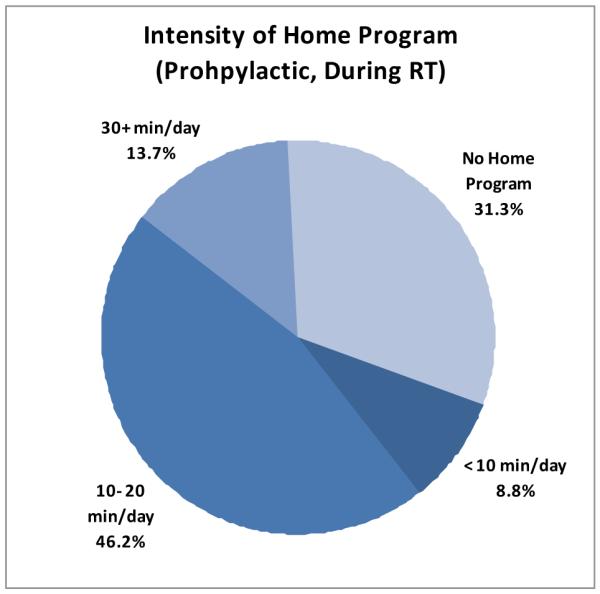
Intensity of home therapy programs recommended for patients during RT. (N=728)
Frequency & Intensity for Patients with mild or clinically insignificant dysphagia after RT
For patients presenting with mild or clinically insignificant dysphagia following RT, approximately 45% of surveyed SLPs said they would prescribe some sort of home program. A quarter of all SLPs still asked their patients to do some type of home therapy program 7 days per week, 10-20 minutes per day [Figure 6 and 7]. Of note, clinicians who recommended therapy after RT for this patient group were about twice as likely to prescribe the least frequent home program (2-3 days per week), and half as likely to prescribe the most intense home program (30+ minutes per day) as compared to the clinicians who recommended prophylactic therapy during RT.
Figure 6.
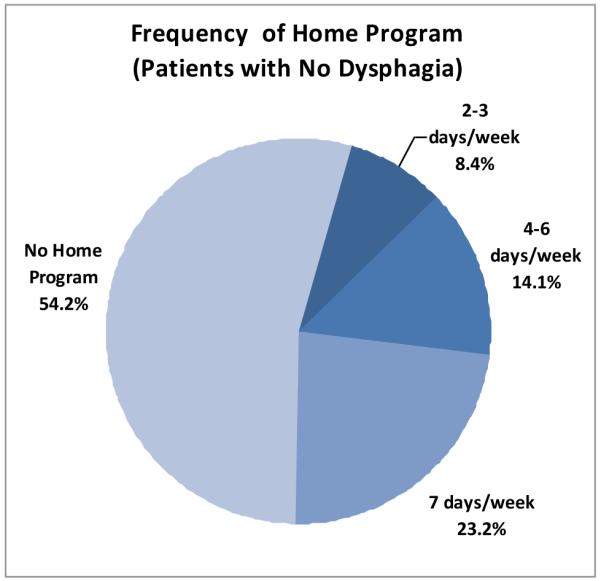
Frequency of home therapy programs recommended for patients following recommended for patients without dysphagia following RT. (N=723)
Figure 7.
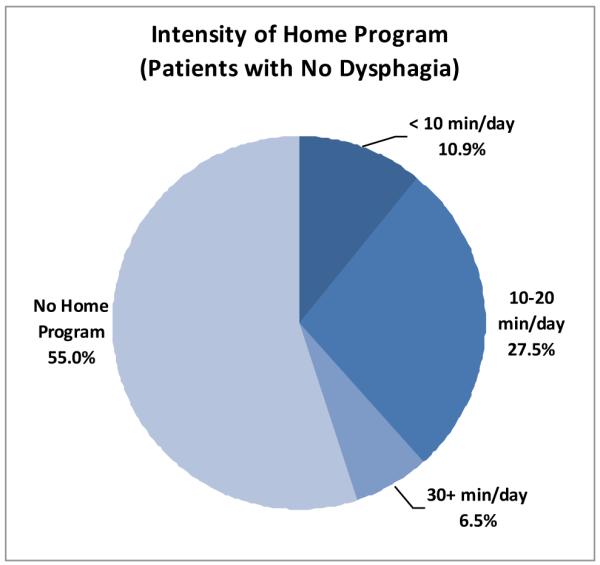
Intensity of home therapy programs recommended for patients without dysphagia following RT. (N=723)
Frequency & Intensity for Patients with moderate or severe dysphagia after RT
While most SLPs recommended almost all treatment options for patients with dysphagia after RT [Figure 3], not all SLPs recommended they be done with similar frequency. [Figure 8] When a patient did develop dysphagia after RT, a 7 days/week home therapy program was recommended by most SLPs (65.8%). However, slightly more than a quarter of respondents recommended a somewhat less intense program of 4-6 days/week. A similar pattern was observed when respondents were asked about the intensity of their prescribed treatment programs for their dysphagic patients. A majority (63.0%) recommended that home programs last 10-20 minutes per day, but again a large number of SLPs disagreed with that majority. Nearly a quarter of the respondents answered that 30 or more minutes per day was ideal, while 1 in 10 felt the opposite extreme was true and recommended less than 10 minutes per day. [Figure 9]
Figure 8.
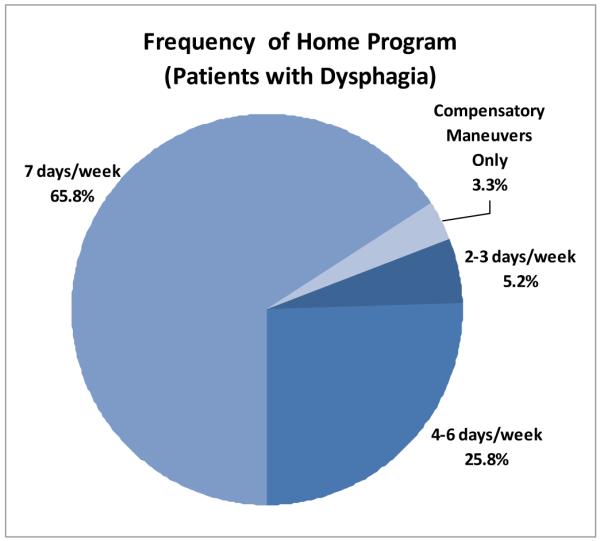
Frequency of home therapy programs recommended for patients with dysphagia following RT. (N=737)
Figure 9.
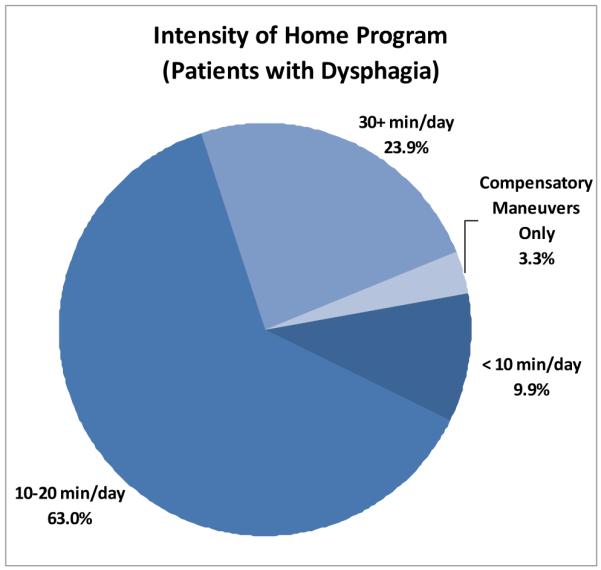
Intensity of home therapy programs recommended for patients with dysphagia following RT. (N=737)
Usual Practices of PEG / FT Use
The SLPs surveyed were asked two questions about feeding tube recommendations and practices. The first question asked about their institution’s policy for feeding tube placement in the HNC population. Most SLPs (71.3%) made it clear that their institutions recommend feeding tubes for patients only when needed. However, a small minority (13.3%) answered that their institutions recommend that all patients receive prophylactic feeding tubes, defined as before or within the first week of RT. The rest followed various other institution specific guidelines. General patterns of feeding tube placement were independent of institution type. However, among institutions that placed FTs reactively, Skilled Nursing Facilities, followed by Academic Teaching Hospitals, were statistically more likely (p=0.0004, OR=3.63 and p=0.0030, OR=1.95, respectively) to place such FTs as compared to all other institutions.
The second question asked how respondents generally recommended their patients use their feeding tubes if one was placed. The respondents were given the choices of “Use the feeding tube as much as possible”, “Use the feeding tube conservatively”, and “*Do+ not use the feeding tube unless absolutely necessary”. A majority of SLPs from every institution selected the broad intermediate response of “conservatively”. Conversely, this leaves nearly half of the respondents sharply divided between the two extremes of using the feeding tube “as much as possible” (20.5%), and only when “absolutely necessary” (22.3%). Such a division delineates just how inconsistent recommendations are for FT use [Figure 10].
Figure 10.

SLPs recommendations for PEG use among HNC patients who receive a prophylactic PEG. (N=722) .
Trends in Compliance
Survey participants were asked how compliant they believed patients were in carrying out their therapy recommendations. The question was asked separately for patients who had mild or clinically insignificant dysphagia, and for patients who had a moderate to severe dysphagia.
In patients who had mild to no dysphagia, regression analyses revealed little correlation between frequency / intensity of prescribed treatment and perceived home program compliance. The only meaningful correlation was a somewhat surprising one – SLPs who prescribed a 30+ minute per day home program were almost four times as likely to report that their patients were 75-100% compliant, as compared to SLPs who prescribed a less intense home program (OR=3.846, p=0.0027).
In patients who had moderate to severe dysphagia, SLPs who recommended 7 day per week programs were almost two times as likely to report that their patients were 75-100% compliant, as compared to SLPs who prescribed a less frequent home program (OR=1.653, p=0.0420). Interestingly, SLPs who prescribed a 4-6 day per week home program were almost two times as likely as all other SLPs to report that their patients were only 33% compliant with their recommendations (OR=1.815, p=0.0049).
DISCUSSION
Responses from 759 SLPs who treat HNC patients revealed that there are trends, but a lack of consensus regarding timing, type, frequency, or intensity of dysphagia therapy. The majority of institutions (70.6%) did not have a referral policy or referrals were made on a case by case basis. Of those who had policies, the majority indicated their policies were reactive, and patients were referred only once a dysphagia had developed. This suggests that the benefit of preventative treatment is not established but the need for intervention once a dysphagia develops is more widely recognized. Perhaps if there was stronger evidence of treatment efficacy and timing, more institutions would develop standard models for referring and treating these patients. Unfortunately, there is no level-1 evidence that has determined any one particular dysphagia therapy is effective in rehabilitating the dysphagic HNC patient, and only a handful of preliminary studies have suggested that proactive therapy may be beneficial in reducing long term morbidity.
Timing of SLP dysphagia therapy, perhaps unsurprisingly, correlates somewhat with institutional referral policies. Timing of first intervention is fairly evenly distributed between “Before RT”, “During RT”, “In the first 3 months post RT”, and “After 3 months post RT” *table 1]. Clearly there is a lack of consensus regarding optimal timing of dysphagia therapy. However, when teasing out the SLPs who intervened in a purely proactive manner (before or during RT with all patients, not just those who complained of dysphagia), it became clear that far more SLPs see patients reactively (46.9% vs. 18.3%).
One might assume that institutional constraints (staffing, history, etc) dictate when SLPs see these patients, and that would be a fair argument. Our survey also found that more experienced SLPs who have worked with HNC patients for 5+ years, are significantly more likely to intervene with patients proactively. The reason for this is not clear and the questionnaire did not ask them to defend their answer. Perhaps more seasoned SLPs, in an attempt to treat a difficult population, have looked to evidence from published literature that provides some limited support for this practice pattern.
The type of dysphagia therapy used by SLPs was very interesting when reviewed collectively. Even though most SLPs do not typically see patients proactively during RT, if a patient was to be referred to them, approximately 30% of all SLPs did not recommend any proactive interventions. Of those who did, they, on average, prescribed 2 of the 5 treatment types listed in the survey. There was also no consensus regarding which two treatment types should be prescribed. This represents a lack of strong evidence in the literature for any particular proactive intervention.
Once RT is completed, and if the patient has no, or clinically insignificant dysphagia, then SLPs overwhelmingly do not prescribe any dysphagia therapy. This is probably due to the fact that these patients have just completed a taxing cancer treatment, and SLPs realize many of them will not want to do swallowing exercises “just in case”. Of those who did prescribe therapy for these patients, the most common intervention was stretches, probably due to their relatively manageable nature at this point in time.
However, once a patient developed a dysphagia after RT, most SLPs prescribed almost all the different types of therapies available to them. Approximately two thirds of all surveyed SLPs prescribed these therapies 7 days per week, and 10-20 minutes per day. What appears to happen is that SLPs are fairly conservative in managing dysphagia proactively, but once their patients develop a dysphagia, “everything” is prescribed. Since strong evidence for a beneficial effect of any particular intervention is lacking in this population, a “package” is presumably recommended in the hopes that one or more of the therapies might help the patient.
Finally, it is important to recognize that the majority is not always correct, and the results of this survey do not affirm best practices or the efficacy of any treatment plan. While the majority of SLPs prescribe therapy 7 days per week, 10-20 min per day for the dysphagic patient, a substantial quarter of SLPs disagree with that recommendation and prescribe therapy 4-6 days per week, and 30+ minutes per day. Intuition would dictate that more therapy is better, but perhaps less can realize the same outcome, and with less burden to the patient. To date, there are no clinical trials that have attempted to determine optimal frequency or intensity for this patient population.
Interestingly, this survey found that clinicians who prescribed a 30+ minute per day home program to non-dysphagic patients who had completed RT also reported optimal compliance with this rigorous program. There could be a couple of explanations for this seeming anomaly. The first, and the optimistic explanation, is that patients who are prescribed intense exercise programs may take more seriously their potential dysphagia. Perhaps these particular clinicians are also exceptionally persuasive, or are part of a multidisciplinary team that is exceptionally dysphagia-centric. The second, and less optimistic explanation, is that clinicians who prescribe such intense proactive interventions are overly optimistic about their patient’s compliance, and assume the patient follows their prescribed plans. The true rate of compliance is, of course, not known.
Similarly, patients who present with a moderate to severe dysphagia, and who are prescribed a 7 day per week therapy program, seem to also have optimal compliance. Perhaps with this patient population, having something to do every day makes it easier to incorporate the therapy into their daily routines, rather than something they have to do as an “extra” chore during the work week. Perhaps this is why patients who are prescribed 4-6 days of therapy per week are more likely to have a seemingly abysmal 33% compliance rate. Again, the actual compliance rate is unknown.
Finally, usual practices regarding PEGs was of significant interest since PEG use can be viewed as both beneficial and detrimental to HNC patients. On one hand, a PEG can help a patient maintain proper nutrition and weight during a painful course of radiation therapy (9, 10). Conversely, there is a growing body of evidence suggesting that PEG use during RT may result in greater incidence and severity of long term dysphagia (11-13). The theory behind the latter argument is that PEG use may promote muscle atrophy, which, if coupled with a RT-induced fibrosis, can cripple one’s ability to use their swallowing musculature. When SLPs were asked if they recommended that a patient use his/her PEG “only if absolutely necessary”, “conservatively”, or “as much as possible”, they were being indirectly asked which school of thought they belonged to. The majority chose the safe middle ground, but almost half of the respondents were split between “only if absolutely necessary” and “as much as possible”. This again implies that information needed to make informed decisions regarding patient treatment, in this case optimal PEG use, is either lacking or not adequately established.
CONCLUSION
This survey effectively determined that while there are some trends in treatment practices, there is no consensus regarding optimal type, timing, and intensity of dysphagia therapy. In general, experienced clinicians were more likely to treat HNC patients proactively, but if a patient was referred to any SLP during RT, most SLPs prescribed some sort of conservative dysphagia therapy. However, once a patient did develop a dysphagia, most SLPs prescribed almost any and every type of therapy described in the literature. Institutional and individual protocols were variable because there is little evidence to support any particular dysphagia therapy, at any intensity, or at any time, for this unique patient population. Many randomized controlled clinical trials specific to this patient population will be required to establish evidence based practices not only to help guide clinical practice, but also to provide patients with therapies that are effective. Since the burden of dysphagia therapy largely rests on the SLP community, they are most likely the ones who must lead this necessary research endeavor.
Acknowledgments
This work was supported in part by a grant from the NIH/NCI #RO1CA120950-04
Footnotes
CONFLICT OF INTEREST
The authors have no conflict of interest.
Contributor Information
Gintas P. Krisciunas, Department of Otolaryngology, Boston University Medical Center, 820 Harrison Ave, Boston MA 02118.
William Sokoloff, Department of Otolaryngology, Boston University Medical Center, 820 Harrison Ave, Boston MA 02118.
Katherine Stepas, CAS Mathematics and Statistics, Boston University, 111 Cummington St, Boston MA 02215.
Susan E. Langmore, Department of Otolaryngology, Boston University School of Medicine, 820 Harrison Ave, Boston MA 02118; Boston University Sargent College of Health and Rehabilitation Sciences, 635 Commonwealth Ave, Boston MA 02215.
REFERENCES
- 1.Kulbersh BD, Rosenthal EL, McGrew BM, Duncan RD, McColloch NL, Carroll WR, Magnuson JS. Pretreatment, preoperative swallowing exercises may improve dysphagia quality of life. Laryngoscope. 2006;6:883–886. doi: 10.1097/01.mlg.0000217278.96901.fc. [DOI] [PubMed] [Google Scholar]
- 2.Carroll WR, Locher JL, Canon CL, Bohannon IA, McColloch NL, Magnuson JS. Pretreatment swallowing exercises improve swallow function after chemoradiation. Laryngoscope. 2008;1:39–43. doi: 10.1097/MLG.0b013e31815659b0. [DOI] [PubMed] [Google Scholar]
- 3.Ahlberg A, Engstrom T, Nikolaidis P, Gunnarsson K, Johansson H, Sharp L, Laurell G. Early self-care rehabilitation of head and neck cancer patients. Acta Otolaryngol. 2011;5:552–561. doi: 10.3109/00016489.2010.532157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Logemann JA, Rademaker AW, Pauloski BR, Kahrilas PJ. Effects of postural change on aspiration in head and neck surgical patients. Otolaryngol Head Neck Surg. 1994;2:222–227. doi: 10.1177/019459989411000212. [DOI] [PubMed] [Google Scholar]
- 5.Ryu JS, Kang JY, Park JY, Nam SY, Choi SH, Roh JL, Kim SY, Choi KH. The effect of electrical stimulation therapy on dysphagia following treatment for head and neck cancer. Oral Oncol. 2009;8:665–668. doi: 10.1016/j.oraloncology.2008.10.005. [DOI] [PubMed] [Google Scholar]
- 6.Logemann JA, Rademaker A, Pauloski BR, Kelly A, Stangl-McBreen C, Antinoja J, Grande B, Farquharson J, Kern M, Easterling C, Shaker R. A randomized study comparing the Shaker exercise with traditional therapy: a preliminary study. Dysphagia. 2009;4:403–411. doi: 10.1007/s00455-009-9217-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Shaker R, Easterling C, Kern M, Nitschke T, Massey B, Daniels S, Grande B, Kazandjian M, Dikeman K. Rehabilitation of swallowing by exercise in tube-fed patients with pharyngeal dysphagia secondary to abnormal UES opening. Gastroenterology. 2002;5:1314–1321. doi: 10.1053/gast.2002.32999. [DOI] [PubMed] [Google Scholar]
- 8.McCabe D, Ashford J, Wheeler-Hegland K, Frymark T, Mullen R, Musson N, Hammond CS, Schooling T. Evidence-based systematic review: Oropharyngeal dysphagia behavioral treatments. Part IV--impact of dysphagia treatment on individuals’ postcancer treatments. J Rehabil Res Dev. 2009;2:205–214. [PubMed] [Google Scholar]
- 9.Beer KT, Krause KB, Zuercher T, Stanga Z. Early percutaneous endoscopic gastrostomy insertion maintains nutritional state in patients with aerodigestive tract cancer. Nutr Cancer. 2005;1:29–34. doi: 10.1207/s15327914nc5201_4. [DOI] [PubMed] [Google Scholar]
- 10.Hearne BE, Dunaj JM, Daly JM, Strong EW, Vikram B, LePorte BJ, DeCosse JJ. Enteral nutrition support in head and neck cancer: tube vs. oral feeding during radiation therapy. J Am Diet Assoc. 1985;6:669–74. 677. [PubMed] [Google Scholar]
- 11.Langmore S, Krisciunas GP, Miloro KV, Evans SR, Cheng DM. Does PEG Use Cause Dysphagia in Head and Neck Cancer Patients? Dysphagia. 2011 doi: 10.1007/s00455-011-9360-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Chen AM, Li B, Lau DH, Farwell DG, Lu Q, Stuart K, Newman K, Purdy JA, Vijayakumar S. Evaluating the Role of Prophylactic Gastrostomy Tube Placement Prior to Definitive Chemoradiotherapy for Head and Neck Cancer. International Journal of Radiation Oncology*Biology*Physics. 2010;4:1026–1032. doi: 10.1016/j.ijrobp.2009.09.036. [DOI] [PubMed] [Google Scholar]
- 13.Morton RP, Crowder VL, Mawdsley R, Ong E, Izzard M. Elective gastrostomy, nutritional status and quality of life in advanced head and neck cancer patients receiving chemoradiotherapy. ANZ J Surg. 2009;10:713–718. doi: 10.1111/j.1445-2197.2009.05056.x. [DOI] [PubMed] [Google Scholar]