

Abstract
BACKGROUND:
Strength improvement of the shoulder muscles is a major goal in rehabilitation or athletic conditioning programs. The purpose of this study was to determine the effect of shoulder core exercises on the isometric torque of glenohumeral joint movements.
METHODS:
A total of 36 healthy females with no history of shoulder injury enrolled in this study. Subjects were randomly assigned into the control group (n = 18, 22 ± 2.19 years of age) or experimental group (n = 18, 21 ± 2.05 years of age). Subjects in experimental group performed shoulder core exercises, using progressive resistance training, three times a week for six weeks. Subjects in control group performed no exercise. The isometric torque of shoulder movements were measured with Dynatorq device in isolated test positions of glenohumeral muscles at the beginning and after six weeks in both groups.
RESULTS:
shoulder core exercise training led to an increase in maximal isometric torques of shoulder scaption at 0° and 90° arm elevation, external and internal rotation, horizontal adduction and extension movements (p < 0.001 in all instances). No significant difference was found between initial scores and scores after six weeks in the control group (p > 0.05).
CONCLUSIONS:
These findings indicated that shoulder core exercise training leads to an increase in peak torque for all glenohumeral movements that can be considered in glenohumeral muscles strengthening programs.
KEYWORDS: Shoulder Joint Movements, Shoulder Joint Exercise, Movement's Torque, Shoulder Rehabilitation
Shoulder problems are frequently reported in individuals who use theirs arm repetitively during work or recreational activities.1,2 Improvement of the shoulder muscles strength is a major goal in rehabilitation or athletic conditioning programs. Systematic reviews of interventions for shoulder pathologies suggest that exercise is an effective treatment on rotator cuff pathology and shoulder pain.3–6
Several investigators have demonstrated a direct relationship between integrated electromyography (EMG) and muscle force during isometric contractions, that is, at a given muscle length, the increase in muscle force parallels an increase in EMG activity.7 Many specific exercises were described using kinematic, kinetic and EMG data to strengthen the glenohumeral and scapulothoracic muscles. Considering that shoulder complex contains a large number of muscles, various exercises should be performed to specifically strengthen each muscle during each session of training program. Additionally, exercises may be done at home through guided self training in certain cases in which the pain and inflammation are considerably reduced. The increasing costs of rehabilitation also support the use of guided self-training (home exercises) in some cases. Several studies have shown that home exercises can be as effective as exercises that are carried out under the supervision of therapists in clinics.6,8 Therefore it would be of great value to offer a combination of exercises that can be considered a significant challenge for every glenohumeral and scapulothoracic muscles.
Bradley and Tibone9, Moseley et al.10 and Townsend et al.11 determined a shoulder core exercises program for glenohumeral and scapulothoracic muscles. Townsend et al.11 found four exercises [scaption with humeral internal rotation (SIR), flexion, horizontal abduction with externally rotated (HAER) and press-up] were considered core to the strengthening of glenohumeral muscles because this combination were responsible for a high level of EMG activity in all glenohumeral muscles (three parts of deltoid, latissimus dorsi, pectoralis major and rotator cuff muscles). McCarrick and Kemp12 reported an increase in internal and external rotation peak torque after 12 weeks of resistance training including three exercises: external rotation, SIR and HAER. The study conducted by McCarrick and Kemp12 only measured the torque output of rotator cuff muscles in isometric internal and external shoulder rotation. Jobe and Moyness13 stated that the rotator cuff muscles should be evaluated individually. Jenp et al.14 found the positions for isolated testing and strengthening of the rotator cuff muscles.
Although previous studies showed high EMG activity of all glenohumeral muscles during suggested core exercises, no study has been conducted to identify whether this core exercises program in progressive resistance training can lead to strength improvement of all glenohumeral muscles. We hypothesized that, if it would be possible to ascertain that a limited number of exercises could strengthen glenohumeral muscles to an acceptable level, preference may be given to such exercises over specific exercises of individual muscles of shoulder, where the objectives are to increase the general strength of glenohumeral muscles or the use of home exercises. Therefore, the purpose of this study was to investigate the effect of glenohumeral core exercises on isometric torque of glenohumeral joint movements in isolated activity positions of glenohumeral muscles.
Methods
This randomized control trial has been carried out in the biomechanical laboratory of University of Social Welfare and Rehabilitation Sciences in 2008 and 2009.
A sample of 36 female students with normal shoulders which were selected by convenience sampling method participated in this study. Subjects were randomly assigned into an either control group (n = 18), with the mean age of 22 ± 2.1 years, or experimental group (n = 18) with the mean age of 21 ± 2.0 years. Subjects were excluded if they had shoulder and cervical pain and pathology, shoulder instability, previous shoulder surgery, any upper extremity or spine abnormality. All subjects were right hand dominant with no history of resistance training. The right shoulder was examined. Before participating in the study, all subjects signed an informed consent form approved by the human subjects committee of University of Social Welfare and Rehabilitation Sciences. Physical characteristics of the subjects in each group are shown in table 1.
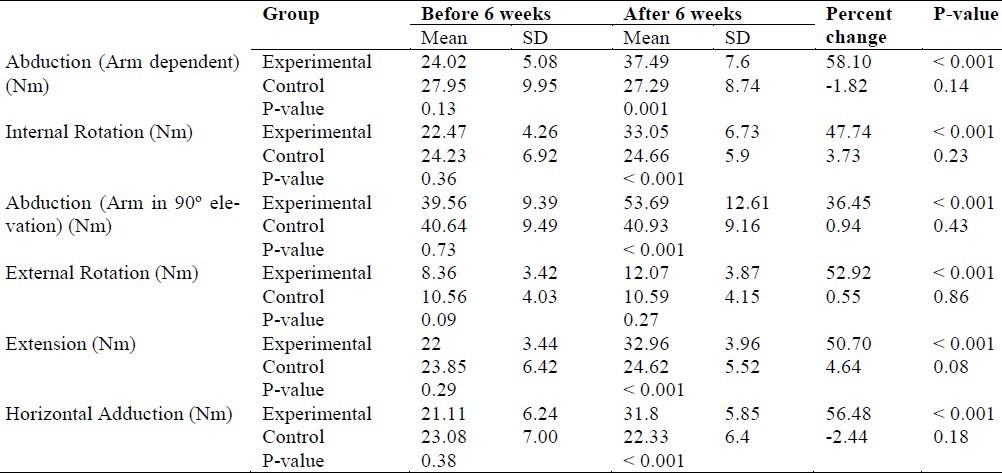
Table 1.
Descriptive Statistics for peak torque Scores before and after training in the two groups
The experimental group participated in 6 weeks of progressive resistive training protocol supervised by a physiotherapist. Four exercises identified as glenohumeral core exercise included SIR, HAER, flexion, and press-up.11 The control group received no training.
The training protocol for SIR, HAER, and flexion exercises: According to Delorme and Watkins regimen,15 the subjects were asked to select a weight in which they could perform 10 repetitions of each exercise (the so-called 10 repetition maximum; or 10 RM). Once the 10 RM was determined, training were divided into the following regimen: 3 sets of 10 RM, the first series with 50% of the 10 RM, the second series with 75% of the 10 RM and the third series with 100% of the 10 RM. The training was carried three times weekly. The 10 RM load was re-evaluated weekly.
The training protocol for press-up exercise: The subjects were instructed to continue the exercise until reaching to the limit of fatigue. After determining the maximal repetition of press-up exercise, the subjects performed 3 sets of maximal repetition every session and three times weekly. Ascertaining the new maximal repetition was performed every week. Three minutes rest period between each set and 15 minutes rest period between each exercise were allowed.
Test procedures: In both groups, isometric peak torque of the glenohumeral motions was measured at the beginning and after six weeks with a Dynatorque device (EASYTECH, S.R.L). Each participant undertook a familiarization session. After a brief explanation of the testing procedures, participants were asked to execute three submaximal trials to familiarize themselves with Dynatorq and the tests procedures. Test sessions consisted of five minutes warm up of shoulder stretching exercise. The subjects were seated in a chair, the trunk and non dominant arm were stabilized by straps. Maximal isometric torques of deltoid, supraspinatus, infraspinatus and teres minor, subscapularis, pectoralis major, latissimus dorsi musculatures were measured as follows:
-
1)
Deltoid: resisted scaption in dependent arm; shoulder at 0° elevation in scapular plane with 90° elbow flexion.16
-
2)
Supraspinatus: resisted scaption in 90° arm elevation; shoulder at 90°elevation in scapular plane and 45° and internal rotation with elbow extension.16
-
3)
Infraspinatus and teres minor: resisted external rotation; shoulder at 90°elevation in sagittal plane and half external rotation with 90°elbow flexion (Figure 1).14
-
4)
Subscapularis: resisted internal rotation; shoulder at 90° elevation in scapular plane and neutral rotation with 90° elbow flexion.16
-
5)
Pectoralis major: resisted horizontal adduction; shoulder at 90° elevation in scapular plane with 90° elbow flexion.16
-
6)
Latissimus dorsi: resisted extension; shoulder at 45° elevation in scapular plane with 90°elbow flexion.16
Figure 1.

Measurement of maximal isometric external rotation torque
Subjects were verbally encouraged to maintain maximal effort while peak torque data were collected for 5 seconds. The mean of three repetitions of maximal isometric contraction was measured in Newton meter (Nm) as peak torque. The order of exercises and test positions were randomized to minimize the effects of fatigue.
Test-retest reliability of the Dynatorq was determined in a pilot study prior to data collection by testing a single shoulder twice, conducted on one day, according to the methodology described above. Ten healthy subjects that were not included in the main study were tested for reliability testing.
Data analysis: The data was analyzed using the SPSS statistical software version 11.5. The peak torque values during six isometric tests were collected in Newton meters from the Dynatorq computer system. Results were normalized by expressing the peak torque value for each subject's weight and presented by the percent. Means and standard deviation were calculated. The intra-class correlation coefficient (ICC), two way mixed effect model, and standard error of measurement (SEM) values were used to assess intra-tester reliability of the measurement. We calculated the ICC (3, 1) as described by Shrout and Fleiss,17 because only one judge evaluated the same population of subjects.
Repeated measures ANOVA accounting for condition (pre-test vs. post-test), group (control vs. training) and interaction of condition and group effects was used to assess the differences between the pre-test and post-test for each group and to compare the differences between the two groups during pre-test and the post-test. The significance level of 0.05 was used for all statistical tests.
Results
The mean ± SD of the age and BMI of the participants in experimental and control groups were 21.7 ± 2.0 years, 20.9 ± 2.6 kg/m2 and 22.3 ± 2.2 years, 20.7 ± 2.7 kg/m2, respectively. There was no statistically significant difference in subject's age (p = 0.39) and BMI (p = 0.79) between the two groups. Descriptive statistics for the measurement scores before and after 6 weeks are presented in table 1.
The result of repeated measures ANOVA showed significant condition by group interaction effect for isometric torque of the all glenohumeral motions (p < 0.001). The main effect of training on isometric torque was also statistically significant for all tested motions. Our analysis revealed a significant increase in peak torque of all tests in experimental group after six weeks core exercises training (p < 0.001). However, no significant difference was found between initial scores and after six weeks scores in the control group (p > 0.05) (Table 1).
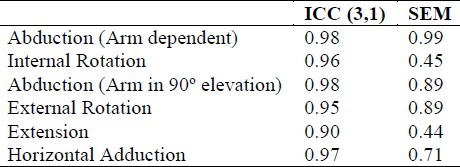
Table 2 presents the ICC and SEM values for test-retest reliability of the each measurement taken in the pilot study. ICC values for the all measurements of maximal isometric torque were greater than 0.90.
Table 2.
Intraclass correlation coefficient (ICC) and standard error of measurement (SEM) values for intratester reliability Variables (n = 10)
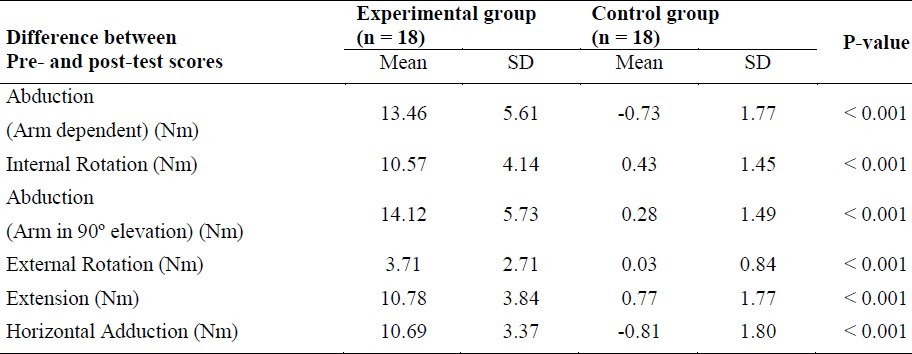
Difference between pre- and post-test scores in two groups is shown in table 3. We found that difference between pre- and post-test scores was significantly greater in experimental group compared with control group for all tested motions (p < 0.001).
Table 3.
Mean difference between pre- and post-tests’ scores in experimental and controls groups (the bold cells indicate significant difference between two groups)
Discussion
The results of present study suggested that shoulder core exercises are effective in improvement of isometric torque of all tested shoulder muscles. The isometric peak torque of scaption movement in dependent arm increased 58.1%. Scaption in dependent arm used to optimal position in generating maximal isometric deltoid torque.16 Abduction movement at 90° elevation in scapular plane showed 36.4% increase in peak torque. This position was regarded as the optimal shoulder position in generating maximal supraspinatus muscle torque.16 Optimal functions of deltoid and rotator cuff muscles are essential for smooth and efficient motion of the glenohumeral joint. The supraspinatus has been identified as the most frequently injured muscle of the rotator cuff group.18,19,13 Thus, restoration and maintenance of supraspinatus strength is one of the important components of shoulder rehabilitation. EMG has been commonly used as the primary criteria for selecting strengthening exercises.20,13 Jobe and Moyness13 were the first who recommended SIR (empty can exercise) to strengthen the supraspinatus muscle using EMG finding. In Townsend et al.11 study on EMG activity of the supraspinatus muscle during a rehabilitation program, SIR or flexion exercises generated at least 50% of its manual muscle test. Similar findings have been reported by others.21,22 Reinold et al.23 and Malanga et al.24 compared three exercises (HAER, SIR and scaption with external rotation) and concluded that these exercises showed similar activity of the supraspinatus. The obvious explanation for increasing of isometric peak torques of scaption in dependent arm and 90° arm elevation is that the supraspinatus and deltoid are adequately exercised with SIR, flexion and HAER that were included in our training program. Thigpen et al.25 however, found that there is more scapular internal rotation and anterior tipping during SIR compared to scaption with external rotation exercise. The empty can exercise was used in this study, because it was one of the exercises that were responsible for a high level of electromyography activity in all glenohumeral muscles. Scaption with external rotation (full can exercise) demonstrated a significantly lower amount of middle and posterior deltoid activity compared to the SIR and HAER exercises. Reinold et al.26 however suggested that the middle and anterior deltoid may have significant impact on superior humeral translation, and exercises with high levels of middle and anterior deltoid such as empty can exercise, should likely be minimized for rotator cuff pathology or a deficiency in glenohumeral stabilization that are symptomatic. Thus, when maintenance of the subacromial space is important (such as impingement syndrome patients), use of scaption with external rotation exercises seems most appropriate for supraspinatus strengthening,25 though asymptomatic subjects were included in our study. However, Levy et al.27 found that anterior deltoid rehabilitation was effective in improving the function and pain in elderly patients with massive cuff tears.
Our training also produced 47.7% increases in peak torque of subscapularis that was measured during internal rotation when the arm was positioned in scapular plane, elevated to 90° and in neutral rotation. Jenp et al.14 found the scapular plane with 90° of shoulder elevation in neutral rotation best isolated the subscapularis from pectoralis major .In Townsend et al.11 study, side lying internal rotation at 0° of abduction failed to activate the subscapularis at levels that met their criteria. The flexion and SIR exercises have been considered as the optimal exercises for subscapularis muscle.11 Hintermeister et al.21 also identified internal rotation elicited lower peak activity of subscapularis than did the shrug and seated rowing exercises. Decker et al.28 reported similar results in which the activity of subscapularis in push up plus and diagonal exercises was higher than traditional internal rotation exercise. Interestingly, internal rotation, which is commonly used for selective subscapularis muscle strengthening, is not an optimal exercise. In agreement with our results, McCarrick and Kemp12 reported increasing of internal rotation peak torque after 12 weeks of resistance training including HAER and SIR exercises.
Another finding of the present study was 52.9% increases in maximal isometric strength of infraspinatus and teres minor that was measured during external rotation peak torque when the shoulder was positioned at 90° elevation in sagittal plane and half external rotation with 90° elbow flexion.14 There was no significant difference in post-test score of external rotation torque between the two groups. Although external rotation torque in the experimental group changed from 8.36 (pre-test) to 12.07 (post-test) but in the control group were 10.56 and 10.59 in pre-test and post-test measurements, respectively.
Several authors have advocated emphasis on shoulder external rotation strengthening during rotator cuff pathologies rehabilitation or overhead athletes conditioning programs.1,2,30–32 Townsend et al.11 determined that the best exercises for infraspinatus and teres minor muscles were to perform HAER and side lying external rotation. Reinold et al.33 suggested that the side lying external rotation produce the highest amount of muscle activity for the external rotators. However, their statistical analysis showed no significant differences among side lying external rotation and HAER.33 Blackburn et al.20 also reported high levels of EMG activity of the infraspinatus and teres minor during prone shoulder external rotation and HAER. McCarrick and Kemp12 also reported an increase in eccentric external rotation strength after 12 weeks of resistance training including three exercises (HAER, SIR, External rotation).
It was also found that the glenohumeral core exercise training can increase maximal isometric strengths of horizontal adduction (56.4%) and extension (51.9%) that were considered as isolated test positions for pectoralis major and latissimus dorsi respectively. The exercise that was known as optimal for both latissimus dorsi and pectoralis major in Townsend et al.11 study was press-up. The press-up exercise is a complex-closed kinetic chain exercise. It has been shown that closed kinetic chain upper limb training facilitates co-contraction of shoulder muscles, improving functional joint stability and strengthening the weak and strong muscles.34–36 Bang and Deyle37 reported a positive effect of exercises, such as press-up on impingement syndrome patients.
Several limitations of the present study must be addressed. Our sample was a homogeneous group of healthy and non-athletic females. Subjects with shoulder pathology and history of resistance training may respond differently to a strengthening program. It is unclear if our results can be applied across populations. Given this limitation, caution should be used in applying these results to the injured and athletic population, so further study in those areas would be necessary. Another limitation of this study is that measurements were taken at the beginning and end of the training by the same and no blinded examiner. However, all subjects were instructed in a similar manner. Finally, it is important to note that in the present study, only maximal isometric torque of glenohumeral motions was measured. We cannot definitely claim that our measurement improvements were due to muscular hypertrophy. The measurement of hypertrophy, as assessed with imaging techniques or neural factors, as judged from EMG activity were not included in this study.
Conclusion
Shoulder core exercise training leads to increase peak torque for all glenohumeral movements and this can be considered in strengthening programs.
Authors’ Contributions
ANM carried out the design and coordinated the study, participated in most of experiments and prepared the manuscript. RM participated in data collection and writing the manuscript. AMA provided assistance for study design and data analysis. AK carried out the data analysis. All authors have read and approved the content of the manuscript.
Acknowledgement
The authors wish to thank all subjects who kindly participated in this research and also the academic members of the Physical Therapy Department of the University of Social Welfare and Rehabilitation Sciences, Tehran, Iran. The manuscript extracted from an MSc thesis numbered: 100-159.
Footnotes
Conflict of Interests Authors have no conflict of interests.
References
- 1.Wilk KE, Arrigo C. Current concepts in the rehabilitation of the athletic shoulder. J Orthop Sports Phys Ther. 1993;18(1):365–78. doi: 10.2519/jospt.1993.18.1.365. [DOI] [PubMed] [Google Scholar]
- 2.Wilk KE, Meister K, Andrews JR. Current concepts in the rehabilitation of the overhead throwing athlete. Am J Sports Med. 2002;30(1):136–51. doi: 10.1177/03635465020300011201. [DOI] [PubMed] [Google Scholar]
- 3.Dorrestijn O, Stevens M, Winters JC, van der Meer K, Diercks RL. Conservative or surgical treatment for subacromial impingement syndrome? A systematic review. J Shoulder Elbow Surg. 2009;18(4):652–60. doi: 10.1016/j.jse.2009.01.010. [DOI] [PubMed] [Google Scholar]
- 4.Faber E, Kuiper JI, Burdorf A, Miedema HS, Verhaar JA. Treatment of impingement syndrome: a systematic review of the effects on functional limitations and return to work. J Occup Rehabil. 2006;16(1):7–25. doi: 10.1007/s10926-005-9003-2. [DOI] [PubMed] [Google Scholar]
- 5.Azadeh H, Dehghani M, Zarezadeh A. Incidence of trapezius myofascial trigger points in patients with the possible carpal tunnel syndrome. J Res Med Sci. 2010;15(5):250–5. [PMC free article] [PubMed] [Google Scholar]
- 6.Kuhn JE. Exercise in the treatment of rotator cuff impingement: a systematic review and a synthesized evidence-based rehabilitation protocol. J Shoulder Elbow Surg. 2009;18(1):138–60. doi: 10.1016/j.jse.2008.06.004. [DOI] [PubMed] [Google Scholar]
- 7.Vredenbregt J, Rau G. Surface electromyography in relation to force, muscle length and endurance. In: Desmedt JE, editor. New Developments in Electromyography and Clinical Neurophysiology. Basel: S Karger AG; 1974. [Google Scholar]
- 8.Walther M, Werner A, Stahlschmidt T, Woelfel R, Gohlke F. The subacromial impingement syndrome of the shoulder treated by conventional physiotherapy, self-training, and a shoulder brace: results of a prospective, randomized study. J Shoulder Elbow Surg. 2004;13(4):417–23. doi: 10.1016/j.jse.2004.02.002. [DOI] [PubMed] [Google Scholar]
- 9.Bradley JP, Tibone JE. Electromyographic analysis of muscle action about the shoulder. Clin Sports Med. 1991;10(4):789–805. [PubMed] [Google Scholar]
- 10.Moseley JB, Jr, Jobe FW, Pink M, Perry J, Tibone J , .EMG analysis of the scapular muscles during a shoulder rehabilitation program. Am J Sports Med. 1992;20(2):128–34. doi: 10.1177/036354659202000206. [DOI] [PubMed] [Google Scholar]
- 11.Townsend H, Jobe FW, Pink M, Perry J. Electromyographic analysis of the glenohumeral muscles during a baseball rehabilitation program. Am J Sports Med. 1991;19(3):264–72. doi: 10.1177/036354659101900309. [DOI] [PubMed] [Google Scholar]
- 12.McCarrick MJ, Kemp JG. The effect of strength training and reduced training on rotator cuff musculature. Clin Biomech (Bristol , Avon ) 2000;15(Suppl 1):S42–S45. doi: 10.1016/s0268-0033(00)00060-7. [DOI] [PubMed] [Google Scholar]
- 13.Jobe FW, Moynes DR. Delineation of diagnostic criteria and a rehabilitation program for rotator cuff injuries. Am J Sports Med. 1982;10(6):336–9. doi: 10.1177/036354658201000602. [DOI] [PubMed] [Google Scholar]
- 14.Jenp YN, Malanga GA, Growney ES, An KN. Activation of the rotator cuff in generating isometric shoulder rotation torque. Am J Sports Med. 1996;24(4):477–85. doi: 10.1177/036354659602400412. [DOI] [PubMed] [Google Scholar]
- 15.Delorme TL, Watkins AL. Technics of progressive resistance exercise. Arch Phys Med Rehabil. 1948;29(5):263–73. [PubMed] [Google Scholar]
- 16.Kelly BT, Williams RJ, Cordasco FA, Backus SI, Otis JC, Weiland DE, et al. Differential patterns of muscle activation in patients with symptomatic and asymptomatic rotator cuff tears. J Shoulder Elbow Surg. 2005;14(2):165–71. doi: 10.1016/j.jse.2004.06.010. [DOI] [PubMed] [Google Scholar]
- 17.Shrout PE, Fleiss JL. Intraclass correlations: uses in assessing rater reliability. Psychol Bull. 1979;86(2):420–8. doi: 10.1037//0033-2909.86.2.420. [DOI] [PubMed] [Google Scholar]
- 18.Burke WS, Vangsness CT, Powers CM. Strengthening the supraspinatus: a clinical and biomechanical review. Clin Orthop Relat Res. 2002;(402):292–8. [PubMed] [Google Scholar]
- 19.Gschwend N, Ivosevic-Radovanovic D, Patte D. Rotator cuff tear--relationship between clinical and anatomopathological findings. Arch Orthop Trauma Surg. 1988;107(1):7–15. doi: 10.1007/BF00463518. [DOI] [PubMed] [Google Scholar]
- 20.Blackburn TA, McLeod WD, White B, Wofford L. EMG analysis of posterior rotator cuff exercises. Athl Train. 1990;25:40–5. [Google Scholar]
- 21.Hintermeister RA, Lange GW, Schultheis JM, Bey MJ, Hawkins RJ. Electromyographic activity and applied load during shoulder rehabilitation exercises using elastic resistance. Am J Sports Med. 1998;26(2):210–20. doi: 10.1177/03635465980260021001. [DOI] [PubMed] [Google Scholar]
- 22.McCann PD, Wootten ME, Kadaba MP, Bigliani LU. A kinematic and electromyographic study of shoulder rehabilitation exercises. Clin Orthop Relat Res. 1993;(288):179–88. [PubMed] [Google Scholar]
- 23.Reinold MM, Macrina LC, Wilk KE, Fleisig GS, Dun S, Barrentine SW, et al. Electromyographic analysis of the supraspinatus and deltoid muscles during 3 common rehabilitation exercises. J Athl Train. 2007;42(4):464–9. [PMC free article] [PubMed] [Google Scholar]
- 24.Malanga GA, Jenp YN, Growney ES, An KN. EMG analysis of shoulder positioning in testing and strengthening the supraspinatus. Med Sci Sports Exerc. 1996;28(6):661–4. doi: 10.1097/00005768-199606000-00003. [DOI] [PubMed] [Google Scholar]
- 25.Thigpen CA, Padua DA, Morgan N, Kreps C, Karas SG. Scapular kinematics during supraspinatus rehabilitation exercise: a comparison of full-can versus empty-can techniques. Am J Sports Med. 2006;34(4):644–52. doi: 10.1177/0363546505281797. [DOI] [PubMed] [Google Scholar]
- 26.Reinold MM, Escamilla RF, Wilk KE. Current concepts in the scientific and clinical rationale behind exercises for glenohumeral and scapulothoracic musculature. J Orthop Sports Phys Ther. 2009;39(2):105–17. doi: 10.2519/jospt.2009.2835. [DOI] [PubMed] [Google Scholar]
- 27.Levy O, Mullett H, Roberts S, Copeland S. The role of anterior deltoid reeducation in patients with massive irreparable degenerative rotator cuff tears. J Shoulder Elbow Surg. 2008;17(6):863–70. doi: 10.1016/j.jse.2008.04.005. [DOI] [PubMed] [Google Scholar]
- 28.Decker MJ, Tokish JM, Ellis HB, Torry MR, Hawkins RJ. Subscapularis muscle activity during selected rehabilitation exercises. Am J Sports Med. 2003;31(1):126–34. doi: 10.1177/03635465030310010601. [DOI] [PubMed] [Google Scholar]
- 29.Ellenbecker TS, Mattalino AJ. Concentric isokinetic shoulder internal and external rotation strength in professional baseball pitchers. J Orthop Sports Phys Ther. 1997;25(5):323–8. doi: 10.2519/jospt.1997.25.5.323. [DOI] [PubMed] [Google Scholar]
- 30.Ramsi M, Swanik KA, Swanik CB, Straub S, Mattacola C. Shoulder-Rotator Strength of High School Swimmers Over the Course of a Competitive Season. J Sport Rahabil. 2004;13:9–18. [Google Scholar]
- 31.Van Cingel R, Kleinrensink G, Stoeckart R, Aufdemkampe G, de Bie R, Kuipers H. Strength values of shoulder internal and external rotators in elite volleyball players. J Sport Rahabil. 2006;15(3):237–45. [Google Scholar]
- 32.Wilk KE, Andrews JR, Arrigo CA, Keirns MA, Erber DJ. The strength characteristics of internal and external rotator muscles in professional baseball pitchers. Am J Sports Med. 1993;21(1):61–6. doi: 10.1177/036354659302100111. [DOI] [PubMed] [Google Scholar]
- 33.Reinold MM, Wilk KE, Fleisig GS, Zheng N, Barrentine SW, Chmielewski T, et al. Electromyographic analysis of the rotator cuff and deltoid musculature during common shoulder external rotation exercises. J Orthop Sports Phys Ther. 2004;34(7):385–94. doi: 10.2519/jospt.2004.34.7.385. [DOI] [PubMed] [Google Scholar]
- 34.Giannakopoulos K, Beneka A, Malliou P, Godolias G. Isolated vs.complex exercise in strengthening the rotator cuff muscle group. J Strength Cond Res. 2004;18(1):144–8. doi: 10.1519/1533-4287(2004)018<0144:ivceis>2.0.co;2. [DOI] [PubMed] [Google Scholar]
- 35.Myers JB, Wassinger CA, Lephart SM. Sensorimotor contribution to shoulder stability: effect of injury and rehabilitation. Man Ther. 2006;11(3):197–201. doi: 10.1016/j.math.2006.04.002. [DOI] [PubMed] [Google Scholar]
- 36.Ubinger ME. Effect of closed kinetic chain training on neuromuscular control in the upper extremity. J Sport Rahabil. 1999;18(3):184–94. [Google Scholar]
- 37.Bang MD, Deyle GD. Comparison of supervised exercise with and without manual physical therapy for patients with shoulder impingement syndrome. J Orthop Sports Phys Ther. 2000;30(3):126–37. doi: 10.2519/jospt.2000.30.3.126. [DOI] [PubMed] [Google Scholar]