

Abstract
AIM: To study the epidemiologic indicators of uptake and characteristic colonoscopic findings in the Croatian National Colorectal Cancer Screening Program.
METHODS: Colorectal cancer (CRC) was the second leading cause of cancer mortality in men (n = 1063, 49.77/100 000), as well as women (n = 803, 34.89/100 000) in Croatia in 2009. The Croatian National CRC Screening Program was established by the Ministry of Health and Social Welfare, and its implementation started in September, 2007. The coordinators were recruited in each county institute of public health with an obligation to provide fecal occult blood testing (FOBT) to the participants, followed by colonoscopy in all positive cases. The FOBT was performed by hypersensitive guaiac-based Hemognost card test (Biognost, Zagreb). The test and short questionnaire were delivered to the home addresses of all citizens aged 50-74 years consecutively during a 3-year period. Each participant was required to complete the questionnaire and send it together with the stool specimen on three test cards back to the institute for further analysis. About 4% FOBT positive cases are expected in normal risk populations. A descriptive analysis was performed.
RESULTS: A total of 1 056 694 individuals (born between 1933-1945 and 1952-1957) were invited to screening by the end of September 2011. In total, 210 239 (19.9%) persons returned the envelope with a completed questionnaire, and 181 102 of them returned it with a correctly placed stool specimen on FOBT cards. Until now, 12 477 (6.9%), FOBT-positive patients have been found, which is at the upper limit of the expected values in European Guidelines for Quality Assurance in CRC Screening and Diagnosis [European Union (EU) Guidelines]. Colonoscopy was performed in 8541 cases (uptake 66%). Screening has identified CRC in 472 patients (5.5% of colonoscopied, 3.8% of FOBT-positive, and 0.26% of all screened individuals). This is also in the expected range according to EU Guidelines. Polyps were found and removed in 3329 (39% of colonoscopied) patients. The largest number of polyps were found in the left half of the colon: 64% (19%, 37% and 8% in the rectum, sigma, and descendens, respectively). The other 36% were detected in the proximal part (17% in the transverse colon and 19% in ceco-ascending colon). Small polyps in the rectum (5-10 mm in diameter), sigmoid and descending colon were histologically found to be tubular adenomas in 60% of cases, with a low degree of dysplasia, and 40% were classified as hyperplastic. Polyps of this size in the transverse or ceco-ascending colon in almost 20% had a histologically villous component, but still had a low degree of dysplasia. Polyps sized 10-20 mm in diameter were in 43% cases tubulovillous, and among them, 32% had areas with a high degree of dysplasia, especially those polyps in the ceco-ascending or transverse part. The characteristics of the Croatian CRC Screening National Program in the first 3 years were as follows: relatively low percentage of returned FOBT, higher number of FOBT-positive persons but still in the range for population-based programs, and higher number of pathologic findings (polyps and cancers).
CONCLUSION: These results suggest a need for intervention strategies that include organizational changes and educational activities to improve awareness of CRC screening usefulness and increase participation rates.
Keywords: Colorectal cancer screening, Fecal occult blood testing, Croatian National Colorectal Cancer Screening Program, Colonoscopy, Uptake
INTRODUCTION
The incidence of colorectal cancer (CRC) has been increasing during recent decades, and the lifetime risk for CRC in industrialized countries is about 5%[1]. CRC is the one of major global public health problems, with approximately 950 000 newly diagnosed cases each year[2]. CRC is a good candidate for screening, because it is a disease with high prevalence, has recognized precursor lesions, and early treatment is beneficial. Reducing the number of deaths from CRC depends on detecting and removing precancerous colorectal polyps, as well as detecting and treating the cancer in its early stages[3]. Approximately 3000 new cases of CRC are diagnosed annually in Croatia and around 1900 people die of CRC each year. According to the Croatian Cancer Registry, in 2008 there were 1255 (54.5/100 000) women and 1819 (85.1/100 000) men with newly diagnosed CRC[4]. The incidence and crude mortality rates from CRC have increased since the 1970s (Figure 1), and the incidence and mortality increase considerably after the age of 50 years. In Croatia it was the second leading cause of cancer mortality in men (n = 1063, 49.77/100 000), as well as in women (n = 803, 34.89/100 000) in 2009[5]. CRC constitutes 12.9% of all newly diagnosed carcinomas in the European population (men 12.8%, women 13.1%) and accounts for 12.2% of deaths caused by malignancy[6]. Compared to other European Union (EU) members where organized population screening programs have existed for several years, in Croatia the standardized mortality rates of CRC are higher, but still lower than those in some western countries (Figure 2). The joinpoint analysis showed that CRC in men in Croatia has increasing trends of both incidence calculated as estimated annual percent change (EAPC 2.9%) and mortality (EAPC 2.1%), while in women, the increase in incidence was not significant, but mortality rates in the last 15 years showed a significant increase (EAPC 1.1%)[7].
Figure 1.
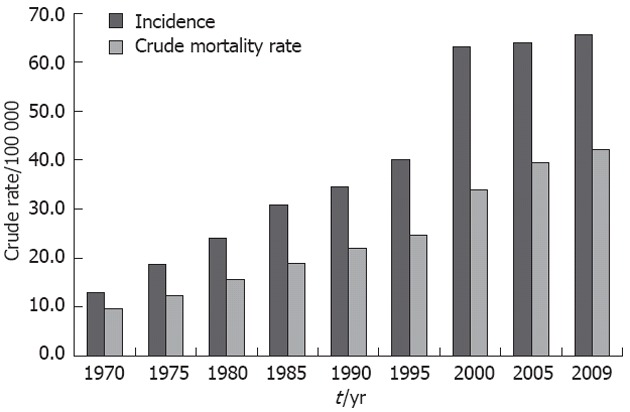
Incidence and crude mortality rate of colorectal cancer in Croatia from 1970 to 2009 year.
Figure 2.
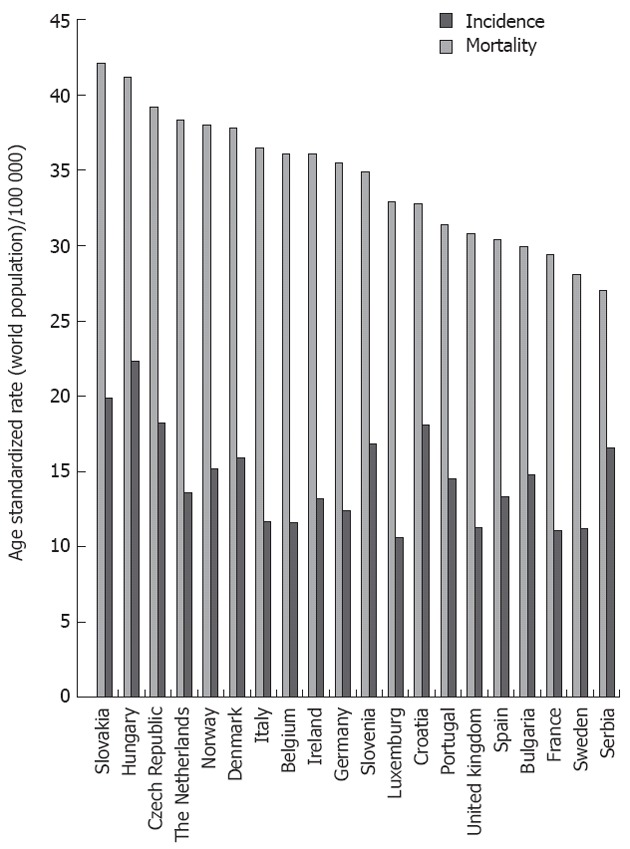
Incidence and mortality rates of colorectal cancer in European countries[40].
A number of randomized trials and one Cochrane review provided strong evidence that fecal occult blood test (FOBT) followed by colonoscopy, if offered every 2 years, reduced mortality rates associated with CRC by 16%[8,9]. In the Czech Republic the rates were higher in a previous period, but, owing to the implementation of organized screening, in 2007 they became lower than in Croatia (Figure 3)[10,11]. Hungary is one of the transitional countries with higher mortality than that in Croatia, and a pilot program has now been completed there and preparations for a nation-wide program are ongoing[12,13]. The EU council recommendation of December 2003, stated that screening for CRC by FOBT in men and women aged 50-74 years met the requirements of the public health program.
Figure 3.
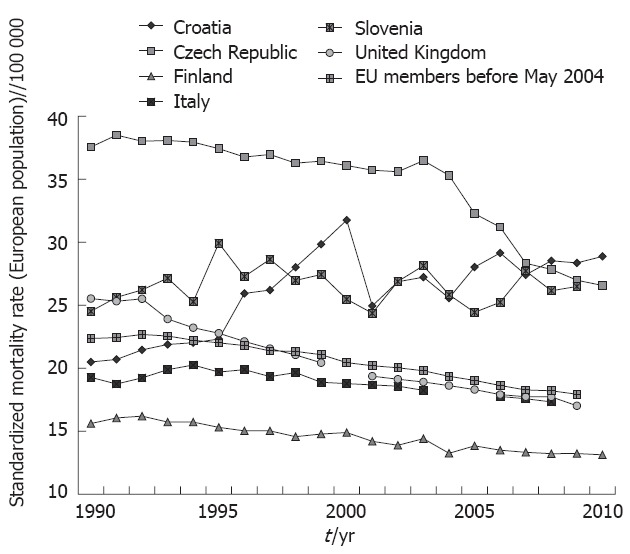
Comparison of standardized mortality rate of colorectal cancer in Croatia and some other European Union countries (source: World Health Organization, European Mortality Database, Health for All 2011).
The Croatian Cancer Registry is a nation wide population-based registry, covering over 90% of cancer cases in the country. The existence of cancer registry allows us to evaluate effects of screening on changes in CRC incidence, which is expected to be higher for the first few years. CRC is also expected to be increasingly detected at an earlier stage owing to the screening program. Therefore, after 5 years, it is expected that our national mortality data will show a reduction in CRC mortality. The aim of this paper is to describe the population-based screening program for CRC whose implementation started during 2008. The political decision to launch it was made by the Ministry of Health and Social Welfare at the end of 2007 according to the previously published proposal[14]. Due to some unexpected organizational difficulties, it is planned that first round will be finished during 2011.
MATERIALS AND METHODS
Program organization: the Republic of Croatia is divided in 20 counties plus the capital city of Zagreb and there is one public health institute in each county and city. In each local public health institute there is a coordinator nominated for the National Screening Program. At the national level, a coordinator from the Croatian National Public Health Institute has been nominated, and all 22 coordinators are members of the Committee for Program Performance. An Expert Committee has also been nominated by the Minister of Health and Social Welfare with the main task to evaluate professional qualification of colonoscopists included in the National Program and to attend to other issues during the program performance. The Committee consists of project co-ordinators from the Ministry of Health and Social Welfare, the National Co-ordinator from the Croatian National Public Health Institute, three members of the Croatian Gastroenterology Society, and representatives of oncologists and primary care physicians. The co-ordinators (medical specialists in epidemiology or in public health) in each local institute of public health are obliged to ensure performance of FOBT, followed by colonoscopy in all positive cases. They also ensure the collection of data on colonoscopic diagnosis, histopathologic findings, cancers and polyps, and to keep records about tests performed in each person. If a patient is diagnosed with CRC, the co-ordinator’s obligation is to inform the patient’s primary care physician. The co-ordinator also has to provide the answers to the questionnaire for each person tested in a web-based database, and to send the report with cumulative data about diagnostic findings to the national co-ordinator. Upon the receipt of the data, the national co-ordinator compiles all data and, according to results, controls the performance in each county. A national report is sent twice monthly to all members of the Expert Committee and to the member in the Ministry of Health and Social Welfare. The main indicators available from these reports include: uptake (compliance), number of persons who correctly applied specimens on cards, number of persons with positive FOBT, number of patients invited to colonoscopy, number of colonoscopies performed, number of patients in whom CRC was diagnosed, number of patients where polyp (polyps) was detected, number of patients where other disease was found (e.g., diverticula, inflammatory bowel diseases, hemorrhoids). The test and short questionnaire were planned to be delivered at the home addresses of all citizens aged 50-74 years consecutively during 3 years. So far, the population born between 1933-1945 and 1952-1957 has been invited. Each participant was required to complete the questionnaire, and send it together with the stool specimen on three test cards (each with four windows) by prepaid mail to the institute for further analysis. Most current FOBT methods are guaiac-based tests, as established more than a century ago. The pseudoperoxidase activity of heme converts colorless guaiac to a blue color in the presence of hydrogen peroxide. The FOBT is performed by guaiac-based HemoGnost card (Biognost, Zagreb, Savica-Šanci) test with a detection limit of 0.252-0.348 mg hemoglobin/g stool. Cards were designed for easy mailing, with a space to write the name of the participant and the date of fecal sampling. Each card had four windows for stool specimens. A leak proof storage and a return envelope were included. The manufacturer’s instructions were closely followed concerning dietary restrictions and advice about taking samples. Dietary restrictions 3 d before and during sampling include avoiding raw meat, liver or blood dishes and large amounts of supplemental vitamin C (> 250 mg/d). Last year, in order to encourage people to take the test, printing the strip-form instruction on the back of the manufacturer’s instructions was arranged. Colonoscopies were done in colonoscopic units (38 of them in Croatia) by well-trained and experienced colonoscopists.
Statistical analysis
A descriptive analysis of epidemiologic indicators was done. Results were compared with the reference range in European Guidelines for Quality Assurance in Colorectal Cancer Screening and Diagnosis[15].
RESULTS
By the end of 2011 a total of 1 056 694 (84% of eligible) individuals (born between 1933-1945 and 1952-1957) were invited to screening. Among them, 210 239 persons (19.9%) returned the envelope with the completed questionnaire and 181 102 of them returned correctly completed FOBT cards. Until now, 12 477 positive FOBT patients have been found (6.9%). Colonoscopy was performed in 8541 cases (uptake 66%). Screening has identified CRC in 472 patients (3.6% of FOBT-positive and 0.26% of all individuals screened through the program). Polyps have been found and removed in 3329 (39% of FOBT-positive) patients (Table 1).
Table 1.
Epidemiologic indicators of colorectal cancer screening uptake and diagnostic findings
| Indicator | n (%) | Relative to issue |
| Invited | 1 056 694 (84.0) | Eligible |
| Returned envelopes | 210 239 (19.9) | Invited |
| Returned with specimen | 181 102 (17.1) | Invited |
| Positive FOBT | 12 477 (6.9) | Returned with specimen and examined |
| Colonoscopy done | 8541 (66.0) | Positive FOBT |
| Hp confirmed Ca | 472 (5.5) | Colonoscopied |
| Patients with polyp(s) | 3329 (39.0) | Colonoscopied |
| Diverticula | 1238 (14.6) | Colonoscopied |
| IBD and other findings | 320 (3.7) | Colonoscopied |
| Hemorrhoids | 2345 (27.5) | Colonoscopied |
FOBT: Fecal occult blood test; Hp: Histopathologically; Ca: Carcinoma; IBD: Inflammatory bowel disease.
Unfortunately, there were great differences in the percentage of returned FOBTs between Croatian counties as well as in the number of pathologic findings (Table 2). Generally, people from continental counties returned FOBT more frequently (13.8%-30.7%), then those from the coastal areas (10.7%-21.7%). The number of CRCs identified varied from 1.0% to 12.2% of all colonoscopy participants (Table 2). There are several reasons for such differences; only partially this depends on variation in CRC and polyp incidence. Probably, the main reason can be attributed to the unequal experience and skills of the endoscopic teams, as well as the inadequate number of endoscopic instruments and equipment in some counties. An additional cause can be found in the greater response of people who had some symptoms of disease (e.g., pain, discomfort, irregular stool evacuation). Some data support this thesis because among false-positive FOBT results for CRC detection, hemorrhoids, inflammatory bowel disease and diverticula in 27.5%, 3.7% and 14.6% of cases, respectively, were found, as well as other changes which can cause positive FOBT results.
Table 2.
Uptake, positive fecal occult blood test and colorectal cancer diagnosed through screening program in Croatian counties
| County | Invited (n) | Uptake-FOBT (%) | Positive | Percentage of pos. FOBT relative to tested persons (%) | Colonoscopied persons (n) | Diagnosed CRC (n) | Percentage of CRC relative to FOBT pos. persons (%) | Percentage of CRC relative to colonscopied persons (%) |
| Bjelovarsko-bilogorska | 29 763 | 24.0 | 385 | 7.8 | 223 | 14 | 3.6 | 6.3 |
| Brodsko-posavska | 39 586 | 19.2 | 526 | 8.8 | 431 | 24 | 4.4 | 5.6 |
| Dubrovačko-neretvanska | 28 971 | 20.2 | 318 | 7.3 | 41 | 5 | 1.6 | 12.2 |
| Istarska | 52 324 | 19.1 | 757 | 7.6 | 600 | 6 | 0.8 | 1.0 |
| Karlovačka | 37 301 | 25.4 | 1107 | 8.7 | 380 | 19 | 3.6 | 5.0 |
| Koprivničko-križevačka | 26 573 | 19.0 | 356 | 7.3 | 104 | 10 | 2.7 | 9.6 |
| Krapinsko-zagorska | 29 440 | 21.2 | 478 | 8.9 | 334 | 29 | 6.1 | 8.7 |
| Ličko-senjska | 16 711 | 13.8 | 647 | 23.9 | 281 | 7 | 1.9 | 2.5 |
| Međimurska | 24 965 | 30.7 | 790 | 11.6 | 703 | 39 | 4.9 | 5.5 |
| Osiječko-baranjska | 75 823 | 19.1 | 1369 | 9.9 | 803 | 58 | 4.2 | 7.2 |
| Požeško slavonska | 19 997 | 28.7 | 401 | 9.8 | 251 | 11 | 2.7 | 4.4 |
| Primorsko-goranska | 78 055 | 21.7 | 905 | 4.1 | 383 | 41 | 6.3 | 10.7 |
| Sisačko-moslavačka | 50 441 | 18.3 | 703 | 8.1 | 585 | 22 | 3.1 | 3.8 |
| Splitsko-dalmatinska | 103 659 | 14.6 | 1287 | 9.0 | 848 | 42 | 3.3 | 5.0 |
| Šibensko-kninska | 32 845 | 10.7 | 160 | 5.0 | 140 | 10 | 6.3 | 7.1 |
| Varaždinska | 38 462 | 21.3 | 522 | 6.5 | 408 | 12 | 2.3 | 2.9 |
| Virovitičko-podravska | 21 176 | 18.7 | 299 | 9.1 | 193 | 7 | 2.3 | 3.6 |
| Vukovarsko-srijemska | 45 562 | 22.2 | 633 | 9.1 | 483 | 17 | 2.7 | 3.5 |
| Zadarska | 45 505 | 16.3 | 582 | 8.2 | 496 | 23 | 4.0 | 4.6 |
| Zagreb town | 190 200 | 22.3 | 361 | 2.9 | 680 | 62 | 6.4 | 9.1 |
| Zagrebačka | 69 335 | 17.2 | 327 | 3.1 | 174 | 14 | 3.9 | 8.0 |
| Total | 1 056 694 | 19.9 | 12 477 | 6.9 | 8541 | 472 | 3.8 | 5.5 |
FOBT: Fecal occult blood test; CRC: Colorectal cancer; pos.: Positive.
We found some differences in characteristics of polyps according to localization and size (Table 3). The largest number of polyps were found in the left half of the colon: 64% (19%, 37% and 8% in the rectum, sigmoid, and descending, respectively). The other 36% were detected in the proximal part (17% in the transverse colon, and 19% in the ceco-ascending). During screening colonoscopy, all polyps up to 15 mm in diameter were removed; 80% of those up to 20 mm in diameter, and 50% of those larger than 20 mm, were later removed by endoscopy or surgery.
Table 3.
Characteristics of polyps detected through colorectal cancer screening program in Croatia
| Part of colon | Localization | Percent (%) | Size 5-10 mm | Size 10-20 mm | Size ≥ 20 mm |
| Left | Rectum | 19 | 60% tubular adenoma, low degree of dysplasia | 43% tubulovillous, among them 32% had areas with a high degree of dysplasia, especially in the ceco-ascending or transverse part | 48% tubular adenomas |
| Sigmoid | 37 | 40% hyperplastic | |||
| Descending | 8 | Tubulovillous and villous | |||
| Right | Transverse | 17 | 20% villous component, low degree of dysplasia | 41% with high grade dysplasia | |
| Ceco-ascending | 19 | 8% intramucosal carcinoma |
Small polyps in the rectum (5-10 mm in diameter), sigmoid and descending colon were histologically tubular adenomas in 60% of cases, with a low degree of dysplasia, and 40% were classified as hyperplastic. Polyps of this size in the transverse or ceco-ascending part in almost 20% had a histologically villous component, but still were at a low degree of dysplasia. Forty-three percent of polyps 10-20 mm in diameter were tubulovillous, and among these 32% had areas with a high degree of dysplasia, especially those polyps in the ceco-ascending or transverse part.
Polyps over 20 mm in the rectum and sigmoid were tubular adenomasin 48% of cases, while others, as well as all the larger polyps in transverse or coecoascendent part were tubulovillous, villous or in 41% with high grade dysplasia, and 8% intramucosal carcinoma.
DISCUSSION
In order to ensure health-care equality, we covered 100% of the available population aged 50-74 years, and 84% of them received the test package at their home address. Sometimes in our program, we were faced with problems such as a lack of educated colonoscopists and/or equipment in some counties. However, this also makes it possible for us to test feasibility in this part of the national health-care system and to plan program costs and the additional resources needed in leading time (mainly colonoscopies and education of population). This study of Croatian colonoscopic practice indicates that there are centers with practice of the highest quality, but considerable effort is required to improve the overall quality of colonoscopy. High quality of endoscopic service, early training, regular refresher courses, and continuous audit of standards at local and national levels must be a priority for all endoscopists performing colonoscopy[16].
Additional efforts must be made to improve the quality of FOBT performance in public health institutes in order to avoid false positives.
Another problem is increasing the uptake, which is in our country significantly lower for CRC than for breast cancer (the uptake for mammography is up to 70%). On one hand, this issue results from unwillingness to take stool specimens and, on the other hand, from non- compliance with avoiding complicated food and therapy restriction before testing. In order to increase the uptake, newly written recommendations by the Group for Quality Control of the International CRC Network support the decision that the procedure and prescriptions have to be simplified, so that they can be changed for the next cycle immediately[15]. We are aware that guaiac FOBT shows notable variations in the performance characteristics between different studies[17]. These differences most likely reflect the different populations tested and the methods for identifying neoplasia. Indeed, from the first results by Allison et al[17] and Greenberg et al[18] to meta-analysis by Soares-Weiser et al[19], different sensitivities for the same tests in different populations or conditions have been reported[20]. In the same reports, some advantages and disadvantages of immuno-FOBT are discussed. In the process of decision making on which test to choose for the Croatian Program, we considered the arrangement of mailing the tests, time from taking specimens to testing, and relatively high surrounding temperatures in almost half a year which all can influence the accuracy of immuno-FOBT[21]. So, we have decided that guaiac card-based tests are more convenient for screening in Croatia. Data about higher percentage of FOBT-positive persons indicated that the population screened so far was not really asymptomatic; people who returned tests most frequently had evident symptoms; mostly blood in stool or impairment of bowel discharge, constipation or diarrhea, with or without pain in the distal abdomen. Thus, there is a need actively to include the individuals who are in the “normal and healthy” population. This is frequently seen at the start of every screening program[22,23]. It is well known that the effectiveness of any screening program depends not only on the diagnostic performance of the screening, but also on the uptake and general acceptance of the test by the public[23,24]. In a field trial, urban-rural differences in the screening uptake were detected[25]. Among some other issues, one of the important problems is to find how to improve uptake. There is clear evidence in our national program of early diagnosis of breast cancer, where we reached a 70% uptake level, that education of a focused population group can increase uptake[25]. We must continue to improve awareness that screening for CRC can reduce the mortality associated with the disease. According to other studies, compliers with CRC screening are less deprived; they have higher education than non-compliers. There is also a need to advance knowledge and promote engagement of primary care physicians, according to other data[21]. However, the Croatian Adult Health Survey showed that self-reported compliance for CRC screening was 4.5% for females and 6.1% for males included in study[26]. It is obvious that the response in the National Screening Program was higher and it depended on the age group of the invited population and county. The results of a control field trial showed a significantly higher response rate to FOBT when given by primary care physicians[27], but, unfortunately, in that study a small number of physicians was voluntarily included, precluding us from achieving conclusive results on the whole population. In addition, this experience cannot be easily implemented to the whole country due to organizational difficulties and presence or absence of willingness of physicians to be included in organized national screening. The results of a population study from Italy confirmed that there is a higher response if the FOBT kit was sent by mail, but in non-responders it incurred higher costs[28]. Response to screening depends on population education but also on willingness of all included in the program, and it has to be carefully planned[29-34]. We still do not have a detailed analysis of costs and possible differences if the test kit is not sent by mail, so this remains to be done for the next cycle.
There are some other reasons for nonparticipation which could be targeted in interventions aimed at increasing participation rates in Croatia. For example, it may be difficult to make arrangements for colonoscopy for people who live on islands and must travel to hospitals in the nearest city on the coast; they feel uncomfortable traveling by ferry while prepared for colonoscopy and must be near the toilet during that journey. Hence, in that case, it might be reasonable to provide a mobile colonoscopy service.
Another problem of CRC screening is people with false-positive FOBT results, who occupy time in colonoscopic units and represent unnecessary procedures. According to our data, most false positive FOBT persons (false-positive to CRC but not to bleeding) had hemorrhoids or anal fissures, which is consistent with the other data[35]. This can be avoided with adequate education of the population and active inclusion of primary care physicians[36].
Successful intervention strategies include organizational changes, such as providing reminders to healthcare providers or users about screening opportunities, better financial support and educational strategies to improve awareness and attitudes toward CRC screening[37,38]. In our future work we also must think about reducing inequalities related to socio economic position and ethnicity in the uptake of screening (e.g., Roma population).
In conclusion, the main characteristics of the Croatian CRC National Program are as follows: low percentage of returned FOBTs, a relatively higher number of FOBT-positive persons, but still in the range for population-based program; and a higher number of pathologic findings (CRC at the upper range and polyps above the upper range)[39].
There are many possible strengthening mechanisms for this activity, which include multifactorial interventions that target more than one level of the screening process and likely can have greater effects. Firstly, much effort must be given to population education and mass campaign with whole society inclusion.
ACKNOWLEDGMENTS
The authors thank all persons included in the implementation and performance of this National Program.
COMMENTS
Background
Colorectal cancer (CRC) screening by either guaiac or immuno fecal occult blood test (FOBT) followed by colonoscopy of all positive patients is recommended worldwide. The main purpose of this screening is to detect CRC in early phase, or in pre-cancer phase when polyps can be easily removed by colonoscopy. This type of cancer can be prevented and/or diagnosed early, and patients can have a better quality of life, and mortality of CRC can be reduced.
Research frontiers
The implementation of the National CRC Screening Program in Croatia gives opportunity for better monitoring uptake of screening and to explore characteristic colonoscopic findings.
Innovations and breakthroughs
The CRC screening program in Croatia is organized through a network of public health institutes and represents good co-operation between public health and clinicians. But, there is still a place for improvement.
Applications
Epidemiologic data of screening uptake and characteristic colonoscopic findings compared with other data and also with expected ranges in European Guidelines for Quality Assurance in Colorectal Cancer Screening and Diagnosis showed similar values in Croatia, but authors found some differences between counties.
Terminology
FOBT can detect very small amounts of blood in stools, which cannot be seen visually without this laboratory test. Patients who have polyps or CRC can be detected by this test. Colonoscopy is still the gold standard to make the final diagnosis and to remove polyps in order to prevent CRC.
Peer review
This study reported data on the CRC Screening Program in Croatia performed with FOBT followed by colonoscopy in positive cases. CRC detection rates widely ranged from 2.5% to 12.2% (mean 5.5%). There are several possible causes for these differences. Data on the histology of polyps removed at endoscopy showed differences between location in colon and size of polyps.
Footnotes
Peer reviewer: Angelo Zullo, MD, Department of Gastroenterology and Digestive Endoscopy, Nuovo Regina Margherita Hospital, Via E Morosini 30, 00153 Roma, Italy
S- Editor Gou SX L- Editor Kerr C E- Editor Zhang DN
References
- 1.Jemal A, Siegel R, Xu J, Ward E. Cancer statistics, 2010. CA Cancer J Clin. 2010;60:277–300. doi: 10.3322/caac.20073. [DOI] [PubMed] [Google Scholar]
- 2.Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer. 2010;127:2893–2917. doi: 10.1002/ijc.25516. [DOI] [PubMed] [Google Scholar]
- 3.Levin B, Lieberman DA, McFarland B, Smith RA, Brooks D, Andrews KS, Dash C, Giardiello FM, Glick S, Levin TR, et al. Screening and surveillance for the early detection of colorectal cancer and adenomatous polyps, 2008: a joint guideline from the American Cancer Society, the US Multi-Society Task Force on Colorectal Cancer, and the American College of Radiology. CA Cancer J Clin. 2008;58:130–160. doi: 10.3322/CA.2007.0018. [DOI] [PubMed] [Google Scholar]
- 4.Znaor A. Cancer Incidence in Croatia 2008. Zagreb: Croatian National Institute of Public Health; 2009. [Google Scholar]
- 5.Čorić T, Mihel S, Miler A, Ivičević Uhernik A, Pristaš I, Petruša B. Umrle osobe u Hrvatskoj u 2010. godini, Hrvatski zavod za javno zdravstvo, zagreb srpanj 2011. Available from: http: //www.hzjz.hr/publikacije/umrli_2010.pdf. [Google Scholar]
- 6.Ferlay J, Autier P, Boniol M, Heanue M, Colombet M, Boyle P. Estimates of the cancer incidence and mortality in Europe in 2006. Ann Oncol. 2007;18:581–592. doi: 10.1093/annonc/mdl498. [DOI] [PubMed] [Google Scholar]
- 7.Kirac I, Sekerija M, Simunović I, Zgaga L, Velimir Vrdoljak D, Kovacević D, Kulis T, Znaor A. Incidence and mortality trends of gastric and colorectal cancers in Croatia, 1988-2008. Croat Med J. 2012;53:124–134. doi: 10.3325/cmj.2012.53.124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Mandel JS, Church TR, Bond JH, Ederer F, Geisser MS, Mongin SJ, Snover DC, Schuman LM. The effect of fecal occult-blood screening on the incidence of colorectal cancer. N Engl J Med. 2000;343:1603–1607. doi: 10.1056/NEJM200011303432203. [DOI] [PubMed] [Google Scholar]
- 9.Towler B, Irwig L, Glasziou P, Kewenter J, Weller D, Silagy C. A systematic review of the effects of screening for colorectal cancer using the faecal occult blood test, hemoccult. BMJ. 1998;317:559–565. doi: 10.1136/bmj.317.7158.559. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Zavoral M. Colorectal cancer screening in the Czech Republic. Z Gastroenterol. 2008;46 Suppl 1:S29–S30. doi: 10.1055/s-2007-963486. [DOI] [PubMed] [Google Scholar]
- 11.Zavoral M, Suchanek S, Zavada F, Dusek L, Muzik J, Seifert B, Fric P. Colorectal cancer screening in Europe. World J Gastroenterol. 2009;15:5907–5915. doi: 10.3748/wjg.15.5907. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Döbrôssy L, Kovács A, Budai A, Cornides A, Ottó S, Tulassay Z. [The state of the colorectal screening in Hungary: lessons of the pilot programs] Orv Hetil. 2007;148:1787–1793. doi: 10.1556/OH.2007.28192. [DOI] [PubMed] [Google Scholar]
- 13.Boncz I, Brodszky V, Péntek M, Agoston I, Nagy Z, Kárpáti K, Kriszbacher I, Fuszek P, Gulácsi L. The disease burden of colorectal cancer in Hungary. Eur J Health Econ. 2010;10 Suppl 1:S35–S40. doi: 10.1007/s10198-009-0192-z. [DOI] [PubMed] [Google Scholar]
- 14.Šamija M, Strnad M, Ebling Z, Kovačić L, Znaor A. Prijedlog nacionalnog programa prevencije i ranog otkrivanja raka u Hrvatskoj. Zagreb: Ministarstvo zdravstva; 2006. [Google Scholar]
- 15.Segnan N, Patnick J, von Karsa L. European Guidelines for Quality Assurance in Colorectal Cancer Screening and Diagnosis. 1st. Luxembourg: Office for Official Publications of the European Communities; 2010. [Google Scholar]
- 16.Bowles CJ, Leicester R, Romaya C, Swarbrick E, Williams CB, Epstein O. A prospective study of colonoscopy practice in the UK today: are we adequately prepared for national colorectal cancer screening tomorrow? Gut. 2004;53:277–283. doi: 10.1136/gut.2003.016436. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Allison JE, Tekawa IS, Ransom LJ, Adrain AL. Improving the fecal occult-blood test. N Engl J Med. 1996;334:1607–1608. doi: 10.1056/NEJM199606133342414. [DOI] [PubMed] [Google Scholar]
- 18.Greenberg PD, Bertario L, Gnauck R, Kronborg O, Hardcastle JD, Epstein MS, Sadowski D, Sudduth R, Zuckerman GR, Rockey DC. A prospective multicenter evaluation of new fecal occult blood tests in patients undergoing colonoscopy. Am J Gastroenterol. 2000;95:1331–1338. doi: 10.1111/j.1572-0241.2000.02032.x. [DOI] [PubMed] [Google Scholar]
- 19.Soares-Weiser K, Jane Burch J, Duffy S, St John J, Smith S, Westwood M, Kleijnen J. Diagnostic accuracy and cost-effectiveness of faecal occult blood tests (fobt) used in screening for colorectal cancer: a systematic review. York: University of York; 2007. pp. 15–35. [Google Scholar]
- 20.Burch JA, Soares-Weiser K, St John DJ, Duffy S, Smith S, Kleijnen J, Westwood M. Diagnostic accuracy of faecal occult blood tests used in screening for colorectal cancer: a systematic review. J Med Screen. 2007;14:132–137. doi: 10.1258/096914107782066220. [DOI] [PubMed] [Google Scholar]
- 21.Duffy MJ, van Rossum LG, van Turenhout ST, Malminiemi O, Sturgeon C, Lamerz R, Nicolini A, Haglund C, Holubec L, Fraser CG, et al. Use of faecal markers in screening for colorectal neoplasia: a European group on tumor markers position paper. Int J Cancer. 2011;128:3–11. doi: 10.1002/ijc.25654. [DOI] [PubMed] [Google Scholar]
- 22.Pox C, Schmiegel W, Classen M. Current status of screening colonoscopy in Europe and in the United States. Endoscopy. 2007;39:168–173. doi: 10.1055/s-2007-966182. [DOI] [PubMed] [Google Scholar]
- 23.Power E, Miles A, von Wagner C, Robb K, Wardle J. Uptake of colorectal cancer screening: system, provider and individual factors and strategies to improve participation. Future Oncol. 2009;5:1371–1388. doi: 10.2217/fon.09.134. [DOI] [PubMed] [Google Scholar]
- 24.Cai SR, Zhang SZ, Zhu HH, Zheng S. Barriers to colorectal cancer screening: a case-control study. World J Gastroenterol. 2009;15:2531–2536. doi: 10.3748/wjg.15.2531. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Stamenić V, Strnad M. Urban-rural differences in a population-based breast cancer screening program in Croatia. Croat Med J. 2011;52:76–86. doi: 10.3325/cmj.2011.52.76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Polasek O, Kolcic I, Voncina L, Strnad M, Vuletic S, Kern J. Breast, colon, and prostate screening in the adult population of Croatia: does rural origin matter? Rural Remote Health. 2007;7:749. [PubMed] [Google Scholar]
- 27.Trtica LM, Strnad M, Gmajnić R, Ebling B, Ebling Z, Marković I, Samija M. Efforts in fighting against cancer in Croatia have to be focused on the primary health care. Coll Antropol. 2008;32:709–724. [PubMed] [Google Scholar]
- 28.Giorgi Rossi P, Grazzini G, Anti M, Baiocchi D, Barca A, Bellardini P, Brezzi S, Camilloni L, Falini P, Maccallini V, et al. Direct mailing of faecal occult blood tests for colorectal cancer screening: a randomized population study from Central Italy. J Med Screen. 2011;18:121–127. doi: 10.1258/jms.2011.011009. [DOI] [PubMed] [Google Scholar]
- 29.Birkenfeld S, Niv Y. Survey of primary physicians’ knowledge of colorectal cancer screening. J Clin Gastroenterol. 2006;40:64–67. doi: 10.1097/01.mcg.0000190763.18734.cd. [DOI] [PubMed] [Google Scholar]
- 30.Pontone S. Colorectal cancer screening behavior and willingness. World J Gastroenterol. 2012;18:2885–2886. doi: 10.3748/wjg.v18.i22.2885. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Lee CS, Ronan L, O’Morain C, McNamara D. Screening for colorectal cancer: what fits best? Expert Rev Gastroenterol Hepatol. 2012;6:301–312. doi: 10.1586/egh.12.12. [DOI] [PubMed] [Google Scholar]
- 32.Van Roosbroeck S, Hoeck S, Van Hal G. Population-based screening for colorectal cancer using an immunochemical faecal occult blood test: A comparison of two invitation strategies. Cancer Epidemiol. 2012:Epub ahead of print. doi: 10.1016/j.canep.2012.04.003. [DOI] [PubMed] [Google Scholar]
- 33.Lionis C, Petelos E. Early detection of colorectal cancer: barriers to screening in the primary care setting. Fam Pract. 2011;28:589–591. doi: 10.1093/fampra/cmr110. [DOI] [PubMed] [Google Scholar]
- 34.Stockbrugger R. Isolated colorectal cancer screening or integrated cancer prevention? A provocative suggestion! Dig Dis. 2012;30:316–319. doi: 10.1159/000337005. [DOI] [PubMed] [Google Scholar]
- 35.Garcia M, Milà N, Binefa G, Borràs JM, Espinàs JA, Moreno V. False-positive results from colorectal cancer screening in Catalonia (Spain), 2000-2010. J Med Screen. 2012;19:77–82. doi: 10.1258/jms.2012.012013. [DOI] [PubMed] [Google Scholar]
- 36.Gillberg A, Ericsson E, Granstrom F, Olsson L. A population-based audit of the clinical use of faecal occult blood testing in primary care for colorectal cancer. Colorectal Dis. 2012;14:e539–546. doi: 10.1111/j.1463-1318.2012.03149.x. [DOI] [PubMed] [Google Scholar]
- 37.Damery S, Clifford S, Wilson S. Colorectal cancer screening using the faecal occult blood test (FOBt): a survey of GP attitudes and practices in the UK. BMC Fam Pract. 2010;11:20. doi: 10.1186/1471-2296-11-20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Sarfaty M, Wender R. How to increase colorectal cancer screening rates in practice. CA Cancer J Clin. 2007;57:354–366. doi: 10.3322/CA.57.6.354. [DOI] [PubMed] [Google Scholar]
- 39.Sieg A, Friedrich K. Perspectives of colorectal cancer screening in Germany 2009. World J Gastrointest Endosc. 2009;1:12–16. doi: 10.4253/wjge.v1.i1.12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.GLOBOCAN 2008. Cancer incidence, mortality and prevalence worldwide. IARC Cancer Base.Section CI5 I.VIII (Detailed), Last accessed on 2012-10-06. Available from: http: //www.dep.iarc.fr/