

Abstract
Background
Reductions in transfusion requirements/improvements in hematologic parameters have been associated with iron chelation therapy in transfusion-dependent patients, including those with myelodysplastic syndromes; data on there reductions/improvements have been limited to case reports and small studies.
Design and Methods
To explore this observation in a large population of patients, we report a post-hoc analysis evaluating hematologic response to deferasirox in a cohort of iron-overloaded patients with myelodysplastic syndromes enrolled in the Evaluation of Patients’ Iron Chelation with Exjade® (EPIC) study using International Working Group 2006 criteria.
Results
Two-hundred and forty-seven, 100 and 50 patients without concomitant medication for myelodysplastic syndromes were eligible for analysis of erythroid, platelet and neutrophil responses, respectively. Erythroid, platelet and neutrophil responses were observed in 21.5% (53/247), 13.0% (13/100) and 22.0% (11/50) of the patients after a median of 109, 169 and 226 days, respectively. Median serum ferritin reductions were greater in hematologic responders compared with non-responders at end of study, although these differences were not statistically significant. A reduction in labile plasma iron to less than 0.4 μmol/L was observed from week 12 onwards; this change did not differ between hematologic responders and non-responders.
Conclusions
This analysis suggests that deferasirox treatment for up to 1 year could lead to improvement in hematologic parameters in some patients with myelodysplastic syndromes.
Keywords: myelodysplastic syndromes, deferasirox, iron overload, iron chelation therapy, hematologic response
Introduction
Myelodysplastic syndromes (MDS) comprise a heterogeneous range of hematopoietic diseases in which bone marrow dysfunction frequently leads to anemia, neutropenia and/or thrombocytopenia with a propensity to evolve to acute myeloid leukemia.1 As a result, key goals for MDS therapy include the improvement of hematologic parameters and transfusion independence.2
Red blood cell transfusions remain an essential therapy to treat the anemia associated with MDS, but transfusion dependency has been identified as an independent factor associated with decreased survival.1,3,4 Furthermore, chronic transfusion therapy can lead to iron overload and subsequent toxicity, to which patients with MDS may be particularly vulnerable as a result of co-morbidities associated with their typically advanced age.5 Various clinical practice guidelines recommend the use of iron chelation therapy in lower-risk MDS patients.6–15
In addition to reports of reduction in iron burden,16,17 a number of recently published case reports and studies have reported improvements in hematologic parameters and transfusion requirements during iron chelation therapy with deferasirox.17–26 There is also limited evidence of hematologic improvement in patients with MDS treated with deferoxamine,27,28 although the exact mechanism of the hematologic response to iron chelators is unknown.
The assessment of transfusion requirements and pre-transfusion blood counts throughout the Evaluation of Patients’ Iron Chelation with Exjade® (EPIC) study,29 which included 341 patients with MDS,16 has enabled post-hoc analysis of hematologic parameters in a large cohort of patients with MDS. Here we report the changes in transfusion requirements, hemoglobin level and platelet and neutrophil counts in patients with MDS treated with deferasirox in the EPIC study, using the hematologic response criteria outlined by the International Working Group (IWG) 2006.30
Design and Methods
Study design and patients
EPIC was a prospective, 1-year, multicenter, open-label, phase IIIb trial (clinicaltrials.gov identifier: NCT00171821). Hematologic parameters were assessed in all patients enrolled in the study. The design of the EPIC study, including the inclusion and exclusion criteria, has been described previously.16,29 In brief, male or female patients with MDS with transfusional iron overload [as shown by serum ferritin levels ≥1000 ng/mL, or <1000 ng/mL but with a history of multiple transfusions (>20 transfusions or >100 mL/kg of red blood cells) and a liver iron concentration of >2 mg Fe/g dry weight as confirmed by R2 magnetic resonance imaging] and a life expectancy of at least 1 year were enrolled. For this post-hoc analysis, patients were assessed for a hematologic response if they received at least one deferasirox dose during the EPIC study, met the inclusion criteria reported in Figure 1 and did not receive concomitant MDS medication.
Figure 1.

Inclusion criteria and definitions of hematologic responses.30 Hb: hemoglobin; RBC: red blood cell.
The study was conducted in accordance with Good Clinical Practice guidelines and the Declaration of Helsinki and was approved by an Institutional Review Board/Independent Ethics Committee.
Deferasirox dosing
Deferasirox dosing for patients with MDS in the EPIC study has been described previously.16 In brief, an initial dose of 20 mg/kg/day was recommended for patients receiving 2–4 units of packed red blood cells/month (7–14 mL/kg/month). Initial doses of 10 or 30 mg/kg/day were considered for patients with lower or higher transfusion frequencies, respectively. Dose adjustments of 5 or 10 mg/kg/day (in the range 0–40 mg/kg/day) were permitted based on 3-monthly serum ferritin trends and safety markers.
Assessments and statistical methods
The IWG 2006 criteria30 (Figure 1) were used to assess erythroid, platelet and neutrophil responses during deferasirox treatment. Time to hematologic response was assessed as the number of days from the first dose of deferasirox to the onset of an erythroid, platelet or neutrophil response.
The definition for erythroid relapse was a reduction in hemoglobin by at least 1.5 g/dL sustained for at least 8 weeks or transfusion dependence after becoming transfusion independent.30 The IWG definitions for platelet and neutrophil relapse were a decrease of 50% or greater from maximum levels in platelets or granulocytes, respectively, for at least 8 weeks.30 The survival time without relapse was defined as duration between response onset and first significant decrease corresponding to the onset of relapse (as assessed by Kaplan–Meier analysis).
Routine hematology assessments during the EPIC study were performed at a central laboratory at baseline, every 4 weeks and at the end of the study. Pre-transfusion blood counts were used in this analysis. Details of ongoing transfusions were recorded throughout the study. Serum ferritin levels were assessed every 4 weeks. Labile plasma iron (LPI) levels were evaluated using methods described previously31 and analyzed at a central laboratory using an assay that measures iron-specific redox cycling capacity in the presence of low ascorbate concentrations.16 LPI assessments were made pre-dose and 2 hours post-dose at weeks 12, 28 and 52. Safety and tolerability were evaluated by monitoring the incidence and type of adverse events. Statistical significance was calculated based on a Wilcoxon rank test.
Results
Patients’ characteristics
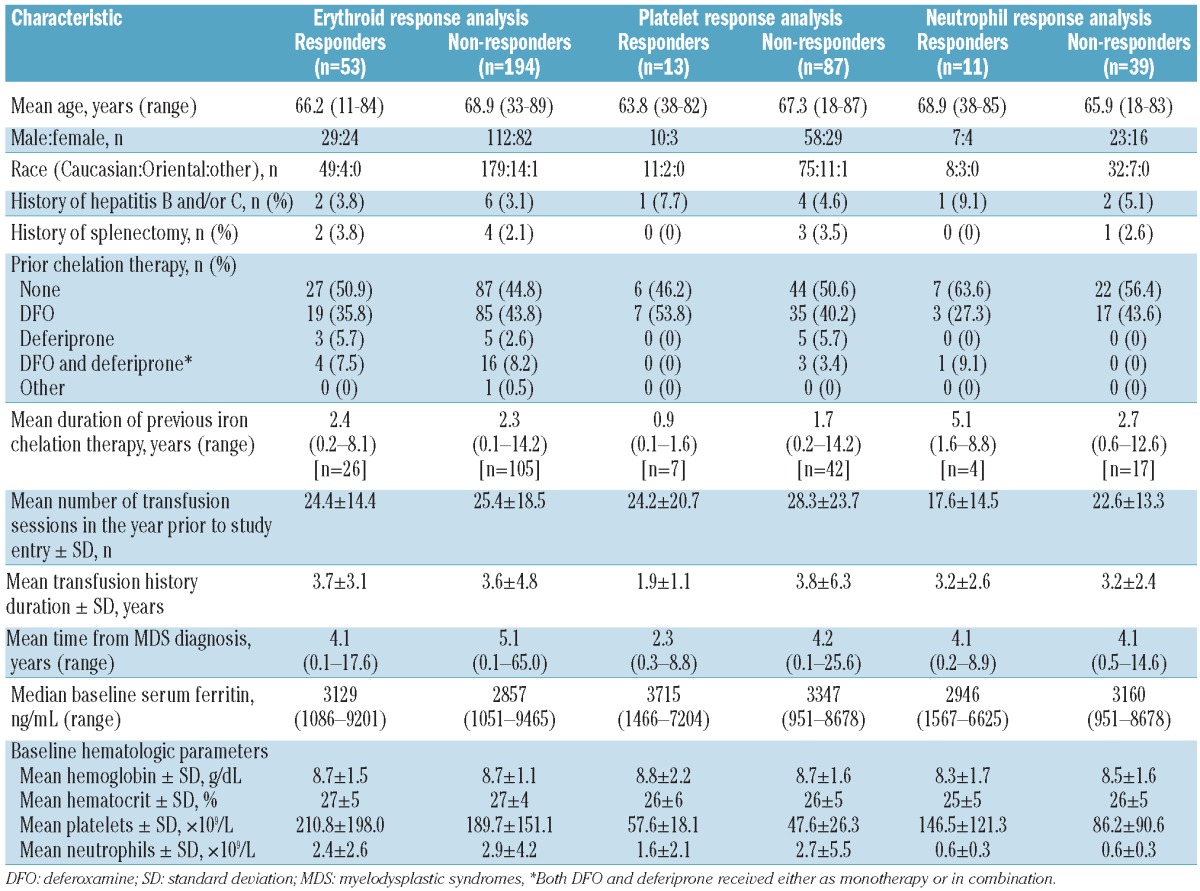
Of the 341 patients with MDS enrolled in the EPIC study, 247 met the erythroid inclusion criteria for response analysis, 100 met the platelet inclusion criterion and 50 met the neutrophil inclusion criterion. The patients’ demographics and characteristics at baseline are presented in Table 1A.
Table 1A.
Characteristics of patients eligible for hematologic analyses.
Deferasirox dosing and exposure
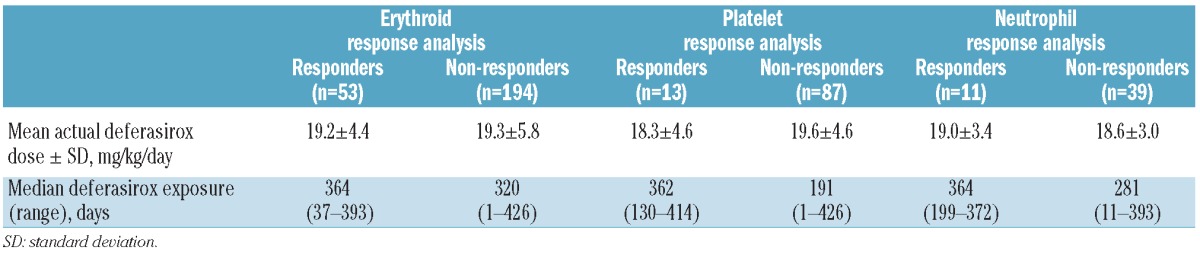
The mean deferasirox dose and median deferasirox exposure are summarized for each hematologic response analysis group in Table 1B. The deferasirox dose was similar in each group and in hematologic responders and non-responders. The median deferasirox exposure was also similar across each group, with the exception of platelet non-responders, who had significantly shorter median exposure compared with platelet responders (191 versus 362 days; P=0.016).
Table 1B.
Deferasirox dosing and exposure.
Effect of deferasirox on hematologic parameters
Erythroid responses, comprising reductions in transfusion requirements or increases in hemoglobin levels were observed in 21.5% (53/247) of patients with a median time to response of 109 days [range, 1–286 days (day on which response started and then lasted for at least 8 weeks); Figure 2A and B]. Twenty-eight patients (11.3%) had a transfusion-only erythroid response and 22 patients (8.9%) had a hemoglobin-only erythroid response. Three patients (1.2%) had both transfusion and hemoglobin erythroid responses (Figure 2A). The overall median time to transfusion response was 100 days (range, 1–283 days). The overall median time to hemoglobin response was 113 days (range, 29–286 days; Figure 2B).
Figure 2.
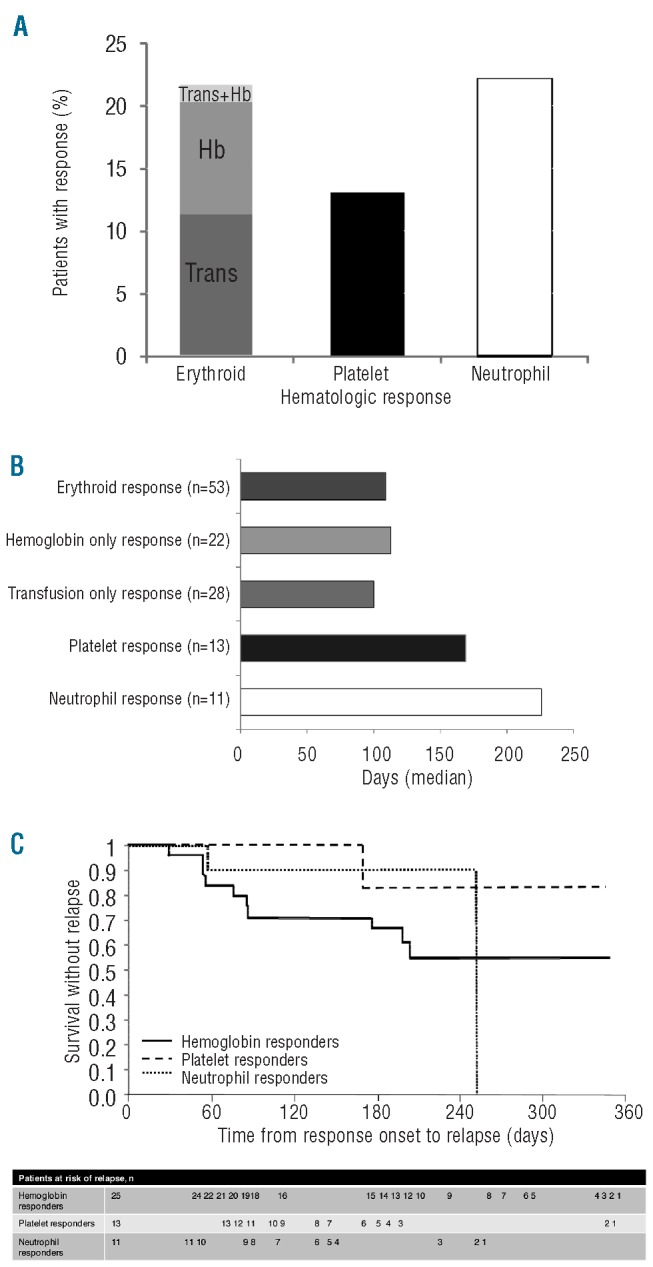
(A) Percentage of patients experiencing hematologic responses, (B) median time to hematologic responses during deferasirox treatment and (C) time from response onset to relapse in patients with hemoglobin, platelet and neutrophil hematologic responses. Trans, transfusion reduction-only response; Hb, hemoglobin improvement-only response; Hb+Trans, both transfusion reduction and hemoglobin response. On the neutrophil curve, from day 248, there is only one patient left at risk, leading to a drop on day 252 when he relapsed.
Platelet responses were observed in 13.0% (13/100) of patients with a median time to response of 169 days (range, 27–320 days; Figure 2A and B). Neutrophil responses were observed in 22.0% (11/50) of patients with a median time to response of 226 days (range, 57–337 days; Figure 2A and B).
Time from response onset to hematologic relapse
Time from response onset to relapse in hematologic response is shown as a Kaplan–Meier curve in Figure 2C. Among transfusion responders, only three patients did not receive any transfusions during the study and were considered as transfusion-independent. Therefore, in accordance with the IWG criteria, relapse in erythroid response was restricted to patients with a hemoglobin response only. Despite this limitation, it is possible to compare transfusion requirements pre-treatment with those after response. Although some patients had an increase in transfusion requirement following their transfusion response, the overall mean number of transfused units in the 8 weeks prior to treatment was 9.1 units, whereas after the transfusion response the overall mean number of transfused units/8-week period was 4.2 units. Relapse rates were highest for hemoglobin responders (40.0%; n=10), followed by neutrophil responders (18.2%; n=2) and lowest among platelet responders (7.7%; n=1). The median time from response onset to relapse in hemoglobin responders was 83.5 days (range, 29 to 204 days). The time from response onset to relapse was 168 days in the one platelet responder who relapsed, and 56 and 252 days (median 154 days) in the two neutrophil responders who relapsed. For those patients with a neutrophil relapse, it should be noted that from day 248, there was only one patient left at risk of relapse, leading to a drop on day 252 when this patient relapsed.
Changes in markers of iron overload in hematologic responders and non-responders
Serum ferritin
Median baseline serum ferritin levels were comparable in both hematologic responders and non-responders across all groups analyzed (Table 1A). By the end of the study, decreases in median serum ferritin were greater in hematologic responders than in non-responders (Figure 3A). In the erythroid response analysis group, responders experienced a reduction in serum ferritin of −560 ng/mL (range, −5194 to 2064 ng/mL) compared with a reduction of −222 ng/mL (range, −7125 to 6124 ng/mL) in erythroid non-responders (P=0.1231). In the platelet response analysis group, responders experienced a reduction in serum ferritin of −976 ng/mL (range, −4488 to 6124 ng/mL) compared with a reduction of −115 ng/mL (range, −3900 to 5357 ng/mL) in platelet non-responders (P=0.0560). In the neutrophil response analysis group, responders experienced the greatest reduction in serum ferritin overall, with a median decrease of −1316 ng/mL (range, −3284 to 6124 ng/mL) compared with a reduction of −583 ng/mL (range, −3900 to 1719 ng/mL) in neutrophil non-responders (P=0.3772).
Figure 3.
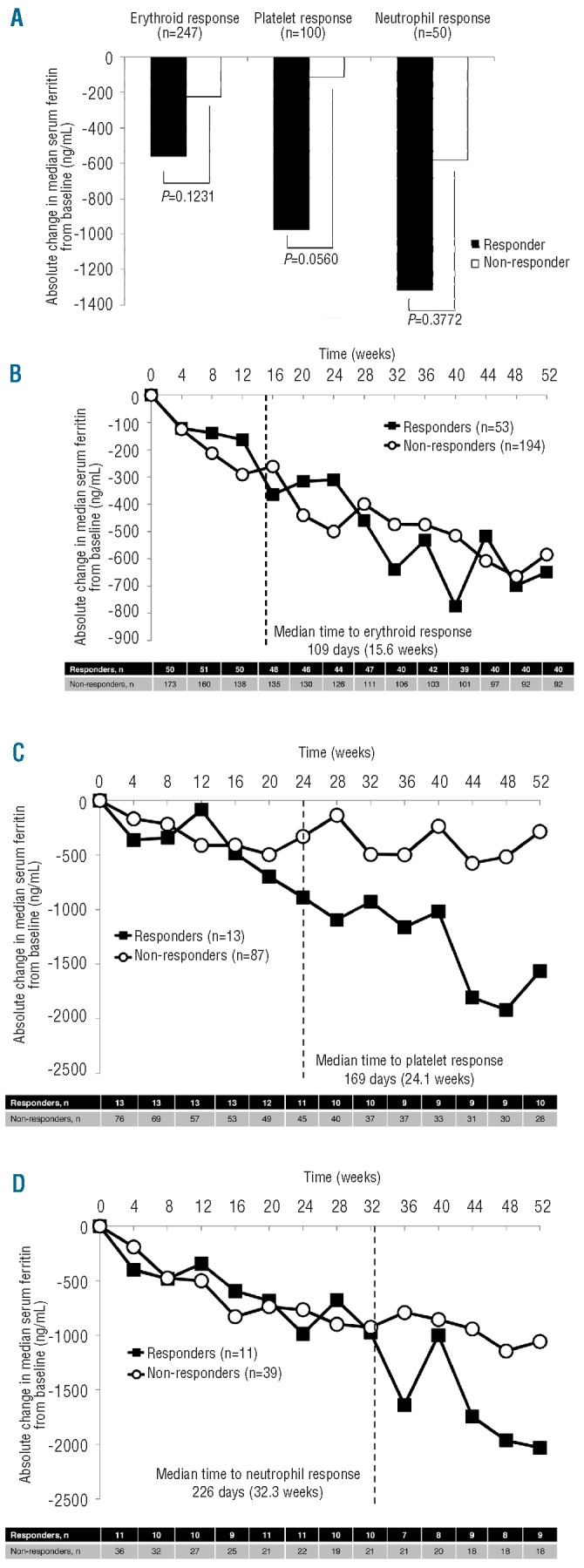
Median decrease in serum ferritin from (A) baseline to end of study and over the course of the study in (B) erythroid, (C) platelet and (D) neutrophil analysis groups.
The median absolute change in serum ferritin levels was also evaluated over time during the study. In the erythroid analysis group, the trend in absolute change in serum ferritin was similar for responders and non-responders, both before and after the median time to response (Figure 3B). In the platelet analysis group, absolute change in serum ferritin was greater in responders than in non-responders from 24 weeks onwards (Figure 3C). In the neutrophil analysis group, the trends in serum ferritin decrease were similar for responders and non-responders before the median time to response, after which the serum ferritin decrease was generally greater in responders than in non-responders (Figure 3D).
Labile plasma iron
At baseline, mean pre-dose LPI levels were above the normal threshold of 0.4 μmol/L in all responder and non-responder groups except platelet non-responders (0.379±0.54 μmol/L). The mean LPI was maintained at less than 0.4 μmol/L at all subsequent pre-dose assessments. During deferasirox treatment, there were no apparent differences in mean LPI levels between responders and non-responders in each analysis group.
Safety and tolerability
Study drug discontinuation
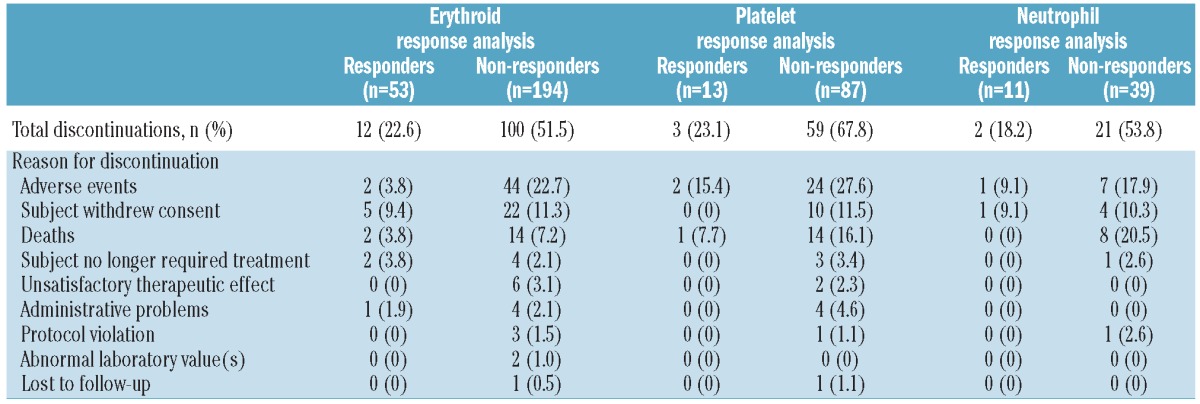
Overall, 54.7, 38.0 and 54.0% of patients in the erythroid, platelet and neutrophil analysis groups, respectively, completed the study (Table 2). Across all groups, completion rates were higher in responders than in non-responders [77.4 versus 48.5% (erythroid response analysis); 76.9 versus 32.2% (platelet response analysis); 81.8 versus 46.2% (neutrophil response analysis)]. Overall, the most common reasons for discontinuation included adverse events, withdrawal of consent and death (Table 2). Adverse events leading to discontinuation were higher in the platelet analysis group (n=26, 26.0%) than in either the erythroid (n=46, 18.6%), or neutrophil (n=8, 16.0%) analysis group. In particular, gastrointestinal adverse events leading to discontinuations were higher in the platelet analysis group (n=15, 15.0%) than in either the erythroid (n=24, 9.7%) or neutrophil (n=6, 12.0%) analysis group.
Table 2.
Patients discontinuing the study and their reasons for doing so.
Adverse events
Adverse events in patients with MDS enrolled in the EPIC study have been described in detail previously.16 In patients who met the criteria for hematologic response analyses, the frequency of drug-related adverse events were similar across erythroid (n=160, 64.8%), platelet (n=63, 63.0%) and neutrophil (n=31, 62.0%) analysis groups; diarrhea was the most frequently reported drug-related adverse event in all analysis groups.
Discussion
This post-hoc analysis in a large group of patients with MDS adds to the existing data from small studies and case reports showing improvements in hematologic parameters with the iron chelator deferasirox. Here iron-overloaded patients with MDS treated with deferasirox for 1 year had improvements in hematologic parameters with an overall erythroid response of 21.5%, platelet response of 13.0% and neutrophil response of 22.0%. Patients taking concomitant MDS medication were removed from the analyses to eliminate any influence of such medication on hematologic responses. However, when previously assessed there was no apparent bias towards either responders or non-responders in the small number of patients who received concomitant medication (data not shown).
Deferasirox dosing and exposure were similar in both responders and non-responders across all analysis groups, with the exception of platelet non-responders, for whom median deferasirox exposure was significantly shorter. This corresponds with the higher rate of discontinuation among patients in the platelet analysis group.
The results are consistent with those of several case reports and small studies describing hematologic improvements, including transfusion independence, in patients with MDS receiving deferasirox treatment.18–22,25 Interestingly, in one case, improvements in transfusional requirements and hemoglobin levels observed after 3 months of deferasirox treatment were reversed following deferasirox interruption, but regained when deferasirox was resumed.25 The IWG 2000 criteria, which classify hematologic responses as major or minor depending on the extent of the improvement,2 were used in a recent retrospective analysis of eight transfused patients (seven patients with MDS, one patient with myelofibrosis) treated with deferasirox (seven patients) and deferoxamine (one patient). Minor erythroid responses (1–2 g/dL increase in hemoglobin in patients with pretreatment hemoglobin concentrations <11 g/dL or 50% decrease in transfusion requirements in transfusion-dependent patients) were observed in five patients treated with deferasirox. A major platelet response was observed in one patient treated with deferasirox (a major platelet response was defined as an absolute increase in platelet count of ≥30×109/L in patients with a pretreatment platelet count <100×109/L or stabilization of platelet counts and platelet transfusion independence in platelet transfusion-dependent patients).23 The IWG 2006 criteria were used to analyze data from 173 patients with lower-risk MDS treated with deferasirox in the large US03 study; hematologic improvements were reported in 51 (28%) patients.17 There are limited reports of hematologic improvement in patients with MDS treated with deferoxamine. One study in 11 patients showed a reduction in hemoglobin requirement of 50% or more in 7/11 (64%) patients and five patients (46%) became transfusion-independent.28 Platelet and neutrophil counts increased in 7/11 (64%) and 7/9 (78%) evaluable patients, respectively. There are even fewer published data on hematologic improvements with deferiprone; a case study in a single patient with myelofibrosis showed an increase in hemoglobin levels following deferiprone treatment.32 Hematologic improvement has been demonstrated during iron chelation therapy in other diseases including myelofibrosis18,23,32,33 and aplastic anemia.22,34 The latter observation suggests that the effect of iron chelation therapy on hematopoiesis may not be a MDS-specific phenomenon and warrants further investigation in other anemias.
Given that a hematologic response to deferasirox was not observed in all treated patients, it was of interest to determine factors that may be associated with this response. Of note, reductions in serum ferritin at the end of the study were generally greater in hematologic responders than in non-responders. Although these differences were not statistically significant, the observation suggests that hematologic response might be at least partially dependent on serum ferritin reductions. On assessment of LPI levels, no differences were noted with respect to reduction in LPI between hematologic responders and non-responders. We, therefore, speculate that a serum ferritin reduction may not be sensitive enough or perhaps too slow to be used as an early discriminator between responders and non-responders. LPI assessment, on the other hand, may be too sensitive as it is suppressed in all chelated patients (both hematologic responders and non-responders). It may be that other parameters such as labile cellular iron could discriminate between responders and non-responders and warrant further investigation. Of course, a connection between responders and deferasirox exposure may also exist, in that responders may have better compliance to their medication than non-responders.
The mechanism underlying improvements in hematologic response to deferasirox has yet to be elucidated. Reduction in oxidative stress, a state which has a variety of inhibitory effects on erythroid and hematopoietic function,35 has been proposed as a possible explanation for the observed hematologic improvement.21,24–26 This hypothesis is supported by the ability of deferasirox to provide 24-hour sustained suppression of LPI17 and to significantly reduce reactive oxygen species.37 In vitro and in vivo data in leukemia cell lines and peripheral mononuclear cells collected from patients with MDS have demonstrated the inhibitory effects of deferasirox on nuclear factor-κB (NF-κB) activity.38 This protein has been shown to be constitutively activated in bone marrow samples from patients with MDS,39 and is involved in several cellular processes including cell proliferation and differentiation and suppression of apoptosis.40 This inhibition was not observed with either deferoxamine or deferiprone, and analyses have suggested the observed inhibitory effects may be independent of the iron chelation effect.38 As hematologic responses have been reported with deferoxamine as well as with deferiprone, albeit in small numbers of patients,28,32 the importance of NF-κB in the hematologic response is uncertain. NF-κB levels were not assessed in this study, but the greater reduction in serum ferritin levels observed in hematologic responders in this study are more supportive of a role for iron reduction in the response mechanism. Alternative mechanisms may include other pharmacological effects of deferasirox on hematopoiesis, redistribution of iron from storage sites to hematopoietic tissue41 or an effect on the neoplastic clone or bone marrow microenvironment.18
This study does have a number of limitations including the lack of a control arm comparing deferasirox to best supportive care. Other treatments including the hypomethylating drug azacitidine and lenalidomide have been shown to improve hematologic parameters in patients with MDS42–44 and are approved for that purpose; azacitidine for all five French-American-British (FAB) subtypes of MDS45 and lenalidomide in del 5q syndrome.46,47 Deferasirox, on the other hand, is approved for the treatment of iron overload in patients with MDS, hence the implications of the observed hematologic improvements with regard to outcomes of MDS patients remain to be elucidated further in future trials. This is especially true given that transfusion dependency is associated with a negative effect on overall survival48 likely due to the fact that a transfusion-dependent state reflects severe bone marrow disease as well as causing iron overload. Hence, the ability of agents such as deferasirox to reduce transfusion requirements may have a potential impact on patients’ survival. However, this can only be confirmed in prospective randomized trials.
A number of issues arose concerning the analysis and interpretation of the findings of this study, regarding the IWG 2006 criteria.2 Within these criteria, the hemoglobin response (defined as an increase in hemoglobin of at least 1.5g/dL) does not distinguish between patients who are not transfused or constantly transfused. In the present study, all patients underwent measurement of hemoglobin prior to each transfusion. Although no change in transfusion requirements was observed in these hemoglobin responders, the increase in hemoglobin reported is clinically important even in patients requiring regular transfusions, as this is associated with better outcomes such as improved quality of life and a reduction in complications. In addition, when considering transfusion relapse following initial response, adhering strictly to the IWG 2006 criteria2 (achievement of transfusion independence followed by a return to transfusion dependence) meant that those patients with an erythroid response based on their transfusion requirements could not be analyzed for subsequent relapse. Despite this, it is important to note that overall the mean number of transfused units over an 8-week period following transfusion response was lower than in the pre-treatment 8-week period.
In conclusion, given the large number of patients included in this analysis, these results provide additional evidence supporting previous observations that deferasirox treatment over 1 year may improve hematologic parameters in patients with MDS. Further prospective, controlled studies are required to confirm the hematologic improvements observed in this study. Additional studies into the mechanisms involved in this response and whether any factors can predict response are also warranted to enhance understanding of this additional benefit of deferasirox.
Acknowledgments
We thank John Mc Intyre for medical editorial assistance with this manuscript.
Footnotes
Funding: this study was sponsored by Novartis Pharma AG. Financial support for medical editorial assistance was provided by Novartis Pharmaceuticals.
Authorship and Disclosures
The information provided by the authors about contributions from persons listed as authors and in acknowledgments is available with the full text of this paper at www.haematologica.org.
Financial and other disclosures provided by the authors using the ICMJE (www.icmje.org) Uniform Format for Disclosure of Competing Interests are also available at www.haematologica.org.
References
- 1.Cazzola M, Malcovati L. Myelodysplastic syndromes - coping with ineffective hematopoiesis. N Engl J Med. 2005;352(6):536–8. doi: 10.1056/NEJMp048266. [DOI] [PubMed] [Google Scholar]
- 2.Cheson BD, Bennett JM, Kantarjian H, Pinto A, Schiffer CA, Nimer SD, et al. Report of an international working group to standardize response criteria for myelodysplastic syndromes. Blood. 2000;96(12):3671–4. [PubMed] [Google Scholar]
- 3.Malcovati L, Della Porta MG, Pascutto C, Invernizzi R, Boni M, Travaglino E, et al. Prognostic factors and life expectancy in myelodysplastic syndromes classified according to WHO criteria: a basis for clinical decision making. J Clin Oncol. 2005;23(30):7594–603. doi: 10.1200/JCO.2005.01.7038. [DOI] [PubMed] [Google Scholar]
- 4.Sanz G, Nomdedeu B, Such E, Bernal T, Belkaid M, Ardanaz T, et al. Independent impact of iron overload and transfusion dependency on survival and leukemic evolution in patients with myelodysplastic syndrome. Blood. 2008;112(11) abst 640. [Google Scholar]
- 5.Gattermann N. Iron overload in myelodysplastic syndromes. Hematol Oncol Clin North Am. 2005;19(Suppl 1):1–26. [Google Scholar]
- 6.National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology v.2: Myelodysplastic Syndromes. 2010. Available at: http://www.nccn.org/professionals/physician_gls/pdf/mds.pdf.
- 7.Bowen D, Culligan D, Jowitt S, Kelsey S, Mufti G, Oscier D, et al. Guidelines for the diagnosis and therapy of adult myelodysplastic syndromes. Br J Haematol. 2003;120(2):187–200. doi: 10.1046/j.1365-2141.2003.03907.x. [DOI] [PubMed] [Google Scholar]
- 8.Gattermann N, Porter J, Lopes LF, Seymour J. Consensus statement on iron overload in myelodysplastic syndromes. Hematol Oncol Clin North Am. 2005;19(Suppl 1):18–25. [Google Scholar]
- 9.Santini V, Alessandrino PE, Angelucci E, Barosi G, Billio A, Di MM, et al. Clinical management of myelodysplastic syndromes: update of SIE, SIES, GITMO practice guidelines. Leuk Res. 2010;34(12):1576–88. doi: 10.1016/j.leukres.2010.01.018. [DOI] [PubMed] [Google Scholar]
- 10.Bennett JM. Consensus statement on iron overload in myelodysplastic syndromes. Am J Hematol. 2008;83(11):858–61. doi: 10.1002/ajh.21269. [DOI] [PubMed] [Google Scholar]
- 11.Arrizabalaga B, del Cañizo C, Remacha A, Sanz G, Villegas A. Guía clínica de quelación del paciente con síndrome mielodisplásico [Clinical guide to chelation therapy for patients with myelodysplastic syndrome (Spanish Guidelines)] Haematologica. 2008;93(Suppl 1):3–10. [Google Scholar]
- 12.Mittelman M, Lugassy G, Merkel D, Tamary H, Sarid N, Rachmilewitz E, et al. Iron chelation therapy in patients with myelodysplastic syndromes: consensus conference guidelines. Isr Med Assoc J. 2008;10(5):374–6. [PubMed] [Google Scholar]
- 13.Suzuki T, Tomonaga M, Miyazaki Y, Nakao S, Ohyashiki K, Matsumura I, et al. Japanese epidemiological survey with consensus statement on Japanese guidelines for treatment of iron overload in bone marrow failure syndromes. Int J Hematol. 2008;88(1):30–5. doi: 10.1007/s12185-008-0119-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Valent P, Krieger O, Stauder R, Wimazal F, Nösslinger T, Sperr WR, et al. Iron overload in myelodysplastic syndromes (MDS) - diagnosis, management, and response criteria: a proposal of the Austrian MDS platform. Eur J Clin Invest. 2008;38(3):143–9. doi: 10.1111/j.1365-2362.2007.01915.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Wells RA, Leber B, Buckstein R, Lipton JH, Hasegawa W, Grewal K, et al. Iron overload in myelodysplastic syndromes: a Canadian consensus guideline. Leuk Res. 2008;32(9):1338–53. doi: 10.1016/j.leukres.2008.02.021. [DOI] [PubMed] [Google Scholar]
- 16.Gattermann N, Finelli C, Della Porta M, Fenaux P, Ganser A, Guerci-Bresler A, et al. Deferasirox in iron-overloaded patients with transfusion-dependent myelodysplastic syndromes: Results from the large 1-year EPIC study. Leuk Res. 2010;34(9):1143–50. doi: 10.1016/j.leukres.2010.03.009. [DOI] [PubMed] [Google Scholar]
- 17.List AF, Baer MR, Steensma DP, Raza A, Esposito J, Martinez-Lopez N, et al. Deferasirox reduces serum ferritin and labile plasma iron in RBC transfusion-dependent patients with myelodysplastic syndrome. J Clin Oncol. 2012;30(17):2134–9. doi: 10.1200/JCO.2010.34.1222. [DOI] [PubMed] [Google Scholar]
- 18.Messa E, Cilloni D, Messa F, Arruga F, Roetto A, Saglio G. Deferasirox treatment improved the hemoglobin level and decreased transfusion requirements in four patients with the myelodysplastic syndrome and primary myelofibrosis. Acta Haematol. 2008;120(2):70–4. doi: 10.1159/000158631. [DOI] [PubMed] [Google Scholar]
- 19.Capalbo S, Spinosa G, Franzese MG, Palumbo G. Early deferasirox treatment in a patient with myelodysplastic syndrome results in a long-term reduction in transfusion requirements. Acta Haematol. 2009;121(1):19–20. doi: 10.1159/000209206. [DOI] [PubMed] [Google Scholar]
- 20.Okabe H, Suzuki T, Omori T, Mori M, Uehara E, Hatano K, et al. Hematopoietic recovery after administration of deferasirox for transfusional iron overload in a case of myelodysplastic syndrome. Rinsho Ketsueki. 2009;50(11):1626–9. [PubMed] [Google Scholar]
- 21.Badawi MA, Vickars LM, Chase JM, Leitch HA. Red blood cell transfusion independence following the initiation of iron chelation therapy in myelodysplastic syndrome. Adv Hematol. 2010;2010:164045. doi: 10.1155/2010/164045. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Oliva EN, Ronco F, Marino A, Alati C, Pratico G, Nobile F. Iron chelation therapy associated with improvement of hematopoiesis in transfusion-dependent patients. Transfusion. 2010;50(7):1568–70. doi: 10.1111/j.1537-2995.2010.02617.x. [DOI] [PubMed] [Google Scholar]
- 23.Molteni A, Riva M, Speziale V, Morra E, Cappellini MD. Iron-chelation therapy in MDS/IMF patients: does it really impact on transfusion requirements? Haematologica. 2010;95(suppl 2) abst 1410. [Google Scholar]
- 24.Nishiuchi T, Okutani Y, Fujita T, Yoshida K, Ohnishi H, Haba R. Effect of iron chelator deferasirox on chronic anemia and thrombocytopenia in a transfusion-dependent patient with myelodysplastic syndrome. Int J Hematol. 2010;91(2):333–5. doi: 10.1007/s12185-010-0500-5. [DOI] [PubMed] [Google Scholar]
- 25.Breccia M, Loglisci G, Salaroli A, Cannella L, Santopietro M, Alimena G. Deferasirox treatment interruption in a transfusion-requiring myelodysplastic patient led to loss of erythroid response. Acta Haematol. 2010;124(1):46–8. doi: 10.1159/000314961. [DOI] [PubMed] [Google Scholar]
- 26.Guariglia R, Martorelli MC, Villani O, Pietrantuono G, Mansueto G, D’Auria F, et al. Positive effects on hematopoiesis in patients with myelodysplastic syndrome receiving deferasirox as oral iron chelation therapy: a brief review. Leuk Res. 2011;35(5):566–7. doi: 10.1016/j.leukres.2010.11.027. [DOI] [PubMed] [Google Scholar]
- 27.Jensen PD, Jensen IM, Ellegaard J. Desferrioxamine treatment reduces blood transfusion requirements in patients with myelodysplastic syndrome. Br J Haematol. 1992;80(1):121–4. doi: 10.1111/j.1365-2141.1992.tb06411.x. [DOI] [PubMed] [Google Scholar]
- 28.Jensen PD, Heickendorff L, Pedersen B, Bendix-Hansen K, Jensen FT, Christensen T, et al. The effect of iron chelation on haemopoiesis in MDS patients with transfusional iron overload. Br J Haematol. 1996;94(2):288–99. doi: 10.1046/j.1365-2141.1996.d01-1795.x. [DOI] [PubMed] [Google Scholar]
- 29.Cappellini MD, Porter JB, El-Beshlawy A, Li C-K, Seymour JF, Elalfy M, et al. Tailoring iron chelation by iron intake and serum ferritin trends: the prospective multicenter EPIC study of deferasirox in 1744 patients with various transfusion-dependent anemias. Haematologica. 2010;95(4):557–66. doi: 10.3324/haematol.2009.014696. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Cheson BD, Greenberg PL, Bennett JM, Lowenberg B, Wijermans PW, Nimer SD, et al. Clinical application and proposal for modification of the International Working Group (IWG) response criteria in myelodysplasia. Blood. 2006;108(2):419–25. doi: 10.1182/blood-2005-10-4149. [DOI] [PubMed] [Google Scholar]
- 31.Esposito BP, Breuer W, Sirankapracha P, Pootrakul P, Hershko C, Cabantchik ZI. Labile plasma iron in iron overload: redox activity and susceptibility to chelation. Blood. 2003;102(7):2670–7. doi: 10.1182/blood-2003-03-0807. [DOI] [PubMed] [Google Scholar]
- 32.Smeets ME, Vreugdenhil G, Holdrinet RS. Improvement of erythropoiesis during treatment with deferiprone in a patient with myelofibrosis and transfusional hemosiderosis. Am J Hematol. 1996;51(3):243–4. doi: 10.1002/(SICI)1096-8652(199603)51:3<243::AID-AJH12>3.0.CO;2-H. [DOI] [PubMed] [Google Scholar]
- 33.Di Tucci AA, Murru R, Alberti D, Rabault B, Deplano S, Angelucci E. Correction of anemia in a transfusion-dependent patient with primary myelofibrosis receiving iron chelation therapy with deferasirox (Exjade®, ICL670) Eur J Haematol. 2007;78(6):540–2. doi: 10.1111/j.1600-0609.2007.00840.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Park SJ, Han CW. Complete hematopoietic recovery after continuous iron chelation therapy in a patient with severe aplastic anemia with secondary hemochromatosis. J Korean Med Sci. 2008;23(2):320–3. doi: 10.3346/jkms.2008.23.2.320. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Ghaffari S. Oxidative stress in the regulation of normal and neoplastic hematopoiesis. Antioxid Redox Signal. 2008;10(11):1923–40. doi: 10.1089/ars.2008.2142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.List AF, Baer MR, Steensma D, Raza A, Esposito J, Virkus J, et al. Deferasirox (ICL670; Exjade®) reduces serum ferritin (SF) and labile plasma iron (LPI) in patients with myelodysplastic syndromes (MDS) Blood. 2007;110(11) abst 1470. [Google Scholar]
- 37.Ghoti H, Fibach E, Merkel D, Perez-Avraham G, Grisariu S, Rachmilewitz EA. Changes in parameters of oxidative stress and free iron biomarkers during treatment with deferasirox in iron-overloaded patients with myelodysplastic syndromes. Haematologica. 2010;95(8):1433–4. doi: 10.3324/haematol.2010.024992. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Messa E, Carturan S, Maffé C, Pautasso M, Bracco E, Roetto A, et al. Deferasirox is a powerful NF-kB inhibitor in myelodysplastic cells and in leukemia cell lines acting independently from intracellular iron chelation and reactive oxygen species scavenging. Haematologica. 2010;95(8):1308–16. doi: 10.3324/haematol.2009.016824. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Braun T, Carvalho G, Coquelle A, Vozenin MC, Lepelley P, Hirsch F, et al. NF-kappaB constitutes a potential therapeutic target in high-risk myelodysplastic syndrome. Blood. 2006;107(3):1156–65. doi: 10.1182/blood-2005-05-1989. [DOI] [PubMed] [Google Scholar]
- 40.Aggarwal BB. Nuclear factor-kappaB: the enemy within. Cancer Cell. 2004;6(3):203–8. doi: 10.1016/j.ccr.2004.09.003. [DOI] [PubMed] [Google Scholar]
- 41.Vreugdenhil G, Smeets M, Feelders RA, van Eijk HG. Iron chelators may enhance erythropoiesis by increasing iron delivery to haematopoietic tissue and erythropoietin response in iron-loading anaemia. Acta Haematol. 1993;89(2):57–60. doi: 10.1159/000204488. [DOI] [PubMed] [Google Scholar]
- 42.Lyons RM, Cosgriff TM, Modi SS, Gersh RH, Hainsworth JD, Cohn AL, et al. Hematologic response to three alternative dosing schedules of azacitidine in patients with myelodysplastic syndromes. J Clin Oncol. 2009;27(11):1850–6. doi: 10.1200/JCO.2008.17.1058. [DOI] [PubMed] [Google Scholar]
- 43.Sekeres MA, List AF, Cuthbertson D, Paquette R, Ganetzky R, Latham D, et al. Phase I combination trial of lenalidomide and azacitidine in patients with higher-risk myelodysplastic syndromes. J Clin Oncol. 2010;28(13):2253–8. doi: 10.1200/JCO.2009.26.0745. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Raza A, Mehdi M, Mumtaz M, Ali F, Lascher S, Galili N. Combination of 5-azacytidine and thalidomide for the treatment of myelodysplastic syndromes and acute myeloid leukemia. Cancer. 2008;113(7):1596–604. doi: 10.1002/cncr.23789. [DOI] [PubMed] [Google Scholar]
- 45.Vidaza (azacitidine) Basic Prescribing Information. 2011. Available at: http://www.vidaza.com/pdf/PI_FINAL.pdf.
- 46.REVLIMID® (lenalidomide) Basic Prescribing Information. 2011. Available at: http://www.revlimid.com/pdf/REVLIMID_PI.pdf.
- 47.Nimer SD. Clinical management of myelodysplastic syndromes with interstitial deletion of chromosome 5q. J Clin Oncol. 2006;24(16):2576–82. doi: 10.1200/JCO.2005.03.6715. [DOI] [PubMed] [Google Scholar]
- 48.Malcovati L, Germing U, Kuendgen A, Della Porta MG, Pascutto C, Invernizzi R, et al. Time-dependent prognostic scoring system for predicting survival and leukemic evolution in myelodysplastic syndromes. J Clin Oncol. 2007;25(23):3503–10. doi: 10.1200/JCO.2006.08.5696. [DOI] [PubMed] [Google Scholar]