

Abstract
Background:
Accurate information about Acquired Immunodeficiency Syndrome (AIDS) and Human Immunodeficiency Virus (HIV) is important for their prevention.
Objectives:
This study is intended to assess knowledge on AIDS in students of secondary schools in Buraidah city and to measure the effect of a health education program on their knowledge about AIDS in general, modes of HIV transmission and the degree of their misperception about the transmission of the disease through casual contact.
Methodology:
A well-designed health education program using personal communication and visual media techniques was conducted for 483 secondary school students in Buraidah secondary schools during the year 1997. Pre and post-tests were done to examine their knowledge about AIDS.
Results and recommendations:
The results of this study pointed out that a health education program on AIDS for students of secondary schools greatly and significantly improved their scores on general knowledge on AIDS views on its transmission and misperception of AIDS (p<0.01). Continuous in-service programs for secondary students are recommended.
Keywords: AIDS, Knowledge, Transmission, Misperception, Students
INTRODUCTION
Acquired Immunodeficiency Syndrome (AIDS) is one of the chief public health issue of the twentieth century. It has attracted unprecedented attention all over the world and has become a focus for priority attention by politicians, public health workers and the general public. This is because in addition to being a new disease with a fatal outcome and a certain amount of mystery surrounding it there is no specific drug for its treatment. Moreover, since it is related to sex,1,2 young people are increasingly at risk3 in many countries and with the emotional and peer pressure and physical violence often used to force many young people into unwanted sex, there is an urgent need for young people to protect themselves against HIV.4
Accurate information about AIDS is important for its prevention. Much of the effort towards this end has focused on educating both the general public and specific high risk groups.5 Periodic evaluation of this effort is therefore important in determining its success and to examine factors that influence the knowledge acquired.6,7
This study was intended to assess knowledge about AIDS in general, modes of transmission of human immuno-deficiency virus (HIV) and the degree of misperception among secondary school students in Buraidah about transmission of the disease through casual contact. It also aimed at finding out how much influence the health education program had had on their knowledge.
SUBJECTS AND METHODS
This study was carried out on 483 students from the Secondary Institute of Commerce (the only institute of commerce in the city), the Secondary Institute of Islamic Science (the only Islamic Science Secondary Institute in the city), Al-Amir Sultan Teaching Compound (the biggest general school for boys in the city) and the 19th secondary school for girls (this is the only girls’ secondary school accessible for this study). The different types of schools for secondary education in Buraidah city during the year 1997 (Technical, Islamic Science and General Education respectively) were represented in the study. The health education program on AIDS was implemented in these institutes. All students in each institute were invited to participate in the program and random cluster samples were chosen from those attending as the study population.
The standard questionnaire administered was used in the U.S. National Health Interview Survey of AIDS knowledge. It was designed to assess knowledge about AIDS and mode of HIV transmission.7,8 The questionnaire was modified to comply with the culture of our community, translated into Arabic and tested before being used.
The questionnaire contained three scales reflecting knowledge of AIDS: general knowledge, transmission knowledge and misperception scores. Seven statements were used to assess general knowledge on AIDS and the number of correct responses was summed up to yield a general knowledge score ranging from 0 to 7. Also, three questions were used to assess knowledge about recognized modes of HIV transmission (sexual, perinatal, and parenteral) and the number of correct responses was summed up to produce a transmission knowledge score ranging from 0 to 3. Higher scores indicate more knowledge. Seven other questions were used to assess perception about HIV transmission through casual contact, the sum of incorrect responses yielding a misperception score that ranged from 0 to 7. A higher score indicates greater misperception.
Every participant in this work was asked to give his personal data including; age, sex, and school grade as well as type of education. The questionnaire was distributed twice. The first time was considered a pre-test before the health education program was launched. This program was designed to improve the knowledge of the target group with regard to general information, modes of transmission and to reduce the degree of misperception about transmission of HIV through casual contact. The strategy adopted relied on a mix of communication methods including health talks, discussions, posters as well as booklets and pamphlets (in Arabic). At the end of the course, the same questionnaire was used as a post-test to evaluate the effectiveness of the program.
Statistical analysis was done using the SPSS/Win Release 6 statistical package.9 The data were grouped and tabulated. Means, standard deviation, student's t-test, paired t-test and F-value of analysis of variance were calculated.
RESULTS AND DISCUSSION
The age of the target sample ranged from 15 to 27 years, and the mode was 17 years. The majority of the students approached were males (81.8%). Grade 2 secondary students formed 39.3% of the sample, 33.6% were grade I and 27.1% were grade III. Moreover, about half of the sample (45.3%) approached were general secondary students, 41% were commercial secondary students, and 13.7% were affiliated to Institute of Islamic Science.
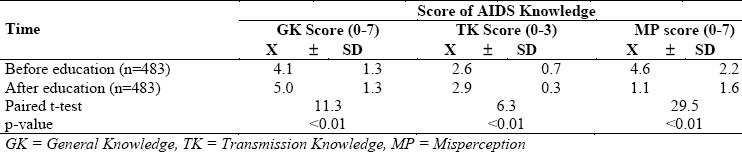
Table 1 clearly shows that the mean values of knowledge scores among the studied sample were 4.1 ± 1.3 for general knowledge, 2.6 ± 0.7 for transmission knowledge and 4.6 ± 2.2 for misperception. These scores greatly improved after the program of health education to 5.0 ± 1.3; 2.9 ± 0.3 and 1.1 ± 1.6 respectively. The differences observed were statistically significant (p<0.01). McCaig et al (1990)7 found that among US adult population, the mean values of the same scores were 4.80 ± 1.02, 2.80 ± 0.01 and 2.90 ± 0.03 respectively. St. Lawrence et al (1989)10 reported that successful efforts to educate the population could result in an increased knowledge of the disease, as well as lowered misperceptions.
Table 1.
AIDS knowledge among the studied-group before and after health education program
It was noted that among the three age groups, knowledge scores had improved significantly by the end of the course (p<0.01) (Table 2). When the different age groups were compared in their pre-test as well as post-test scores, no significant differences were observed in any of the different components of the questionnaire except for general knowledge score after education which was significantly lower in those >18 years of age than the other two age groups (4.7 ± 1.4, 5.0 ± 1.1 and 5.2 ± 1.3 respectively) (Table 3). Wassif et al (1993)11 found no significant differences in any of the different components of the questionnaire among the different age groups. However, Diclemente et al (1988),12 Keeter and Bradford (1988)13 and Hardy et al (1989)14 reported that older persons were less knowledgeable about AIDS.
Table 2.
Comparison of AIDS knowledge among the studied-group before and after health education program according to some demographic variables
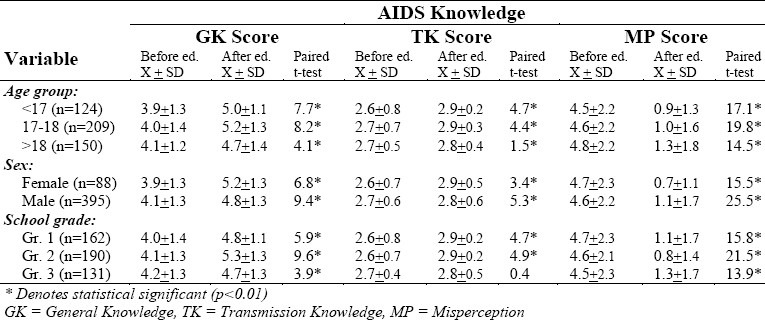
Table 3.
AIDS knowledge among the studied-group according to some demographic variables
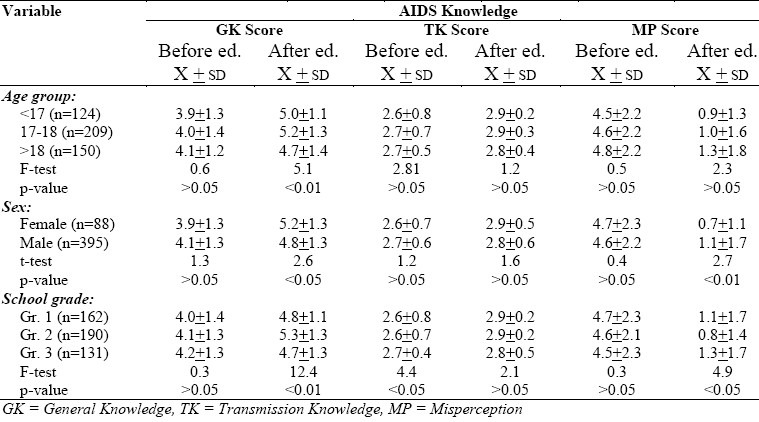
Table 2 reveals that among females, the mean values of knowledge scores were significantly higher in the post-test than in the pre-test and the misperception score was significantly reduced (P<0.01). The same pattern was observed among males. In the pre-test, no significant differences were observed between males and females regarding all the components of the questionnaire (p>0.05). On examination of the results of the post-test, it was found that females had become more knowledgeable than males, but the difference was only significant in the general knowledge scores (p>0.05). Also, the misperception score was significantly more improved in females than in males (0.7 ± 1.1 and 1.1 ± 1.7 respectively) (Table 3)
Grade 1 and Grade II students showed significantly higher scores of general and transmission knowledge as well as significantly lower misperception score in the post-test than in the pre-test results (Table 2). However, Grade III group showed a significant improvement in their general knowledge and misperception scores, while the change in their transmission knowledge score was not statistically significant (Table 2).
Before the health education program, Grade III students had higher scores in general knowledge (4.2 ± 1.3) and transmission knowledge (2.7 ± 0.4) as well as lower misperception score (4.5 ± 2.3) than Grade I and Grade II groups (Table 3) the only significant difference being the transmission scoring (p<0.05). At the end of the program the Grade III group showed the least improvement of the three grades in their knowledge and misperception scores. They had significantly lower general knowledge score as well as significantly higher misperception score than the other two groups (Table 3).
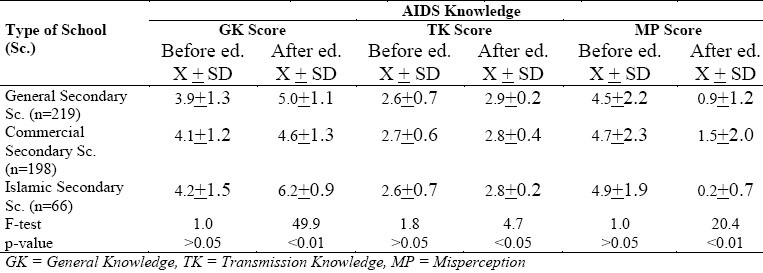
The health education program on AIDS significantly improved the general knowledge, transmission knowledge and misperception scores among students affiliated to general and Islamic science secondary education (p<0.01) (Table 4). However, the effect of the program among those in commercial secondary education was statistically significant on general knowledge and misperception scores, but not for transmission knowledge score (Table 4).
Table 4.
Comparison of AIDS knowledge among the studied-group before and after health education program according to type of school
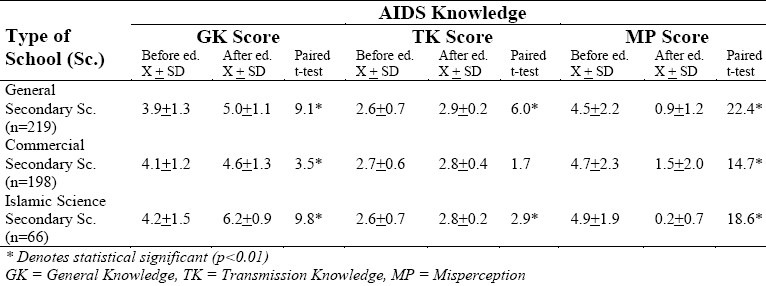
Before conducting the program, students of Islamic science education had higher scores of general knowledge and misperception than general and commercial education groups, as commercial secondary students had the higher transmission knowledge score. However, the differences in the scores for all components of pre-test questionnaire were not statistically significant (p>0.05). By the end of the program, however, students of Islamic Science Education had the highest score for general knowledge (6.2 ± 0.9) and the lowest score for misperception (0.2 ± 0.7) among the three groups, as those in general secondary education had the highest score of transmission knowledge (2.9 ± 0.2). These differences were statistically significant (p<0.05) (Table 5).
Table 5.
AIDS knowledge among the studied-group according to type of school
We concluded that health education program on AIDS had greatly improved the knowledge and misperception scores for students of secondary schools varying according to their level and their individual ability. Individual demographic characteristics, beliefs of the problem, motivation to acquire knowledge, etc., are important factors in health education.15–16
The present study recommends the setting up of extra-curricular activities such as school counseling services, health clubs and discussion groups in secondary schools to talk about AIDS, explain in detail the modes of transmission and the precautions that could be taken against it. Research among other high-risk groups is also recommended.
REFERENCES
- 1.W.H.O. Epidemiology of Acquired Immunodeficiency Syndrome. EM/AIDS/14-E. (2nd edition) 1991:1–7. [Google Scholar]
- 2.Drotman DP, Curran JW. Public Health & Preventive Medicine. 13th ed. Rosenau-last: Prentice-Hall International Inc; 1992. Epidemiology & Prevention of acquired immunodeficiency syndrome. Cited in Maxy; pp. 115–124. [Google Scholar]
- 3.Walter HJ, Vaughan RD, Gladis MM, Rgin DF, Kasen S, Cohall AT. Factors associated with AIDS risk behaviours among high School Students in an AIDS Epicenter. AM J Public Health, 1992;82(4):528–32. doi: 10.2105/ajph.82.4.528. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.AIDS Action (The international newsletter on AIDS prevention and care). Young people first. AHRTAG. 1994 Jun-Aug;(25):1–3. [Google Scholar]
- 5.W.H.O. Epidemiology of Acquired Immunodeficiency Syndrome. EM/GPA/014/E/L. (5th edition) 1993:25–9. [Google Scholar]
- 6.Blake SM, Arkin EB. AIDS information Monitor. Washington, DC: American Red Cross; 1986. A summary of national public opinion surveys on AIDS : 1983 through 1986. [Google Scholar]
- 7.McCaig LF, Hardy AM, Deborah MW. Knowledge about AIDS and HIV in the U.S. adult population: Influence of the Local Incidence of AIDS. Am J Public Health. 1991;81(12):1591–5. doi: 10.2105/ajph.81.12.1591. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.C.D.C. (Centers for Disease Control) AIDS and human immunodeficiency virus infection in the United States : Update. MMWR. 1998;38(suppl 4):1–38. [PubMed] [Google Scholar]
- 9.SPSS Inc. 444 N. Michigan Avenue Chicago, Illinois 60611, USA. 1993 [Google Scholar]
- 10.St. Lawrence JS, Hood HV, Brasfield T, Kelly JA. Differences in men's AIDS risk knowledge and behavior patterns in high and low AIDS prevalence cities. Public Health Report. 1989;104:391–5. [PMC free article] [PubMed] [Google Scholar]
- 11.Wassif OM, El-Gendy MF, Saleh MA, El-Sawaf EM. Effect of Health Education Program on knowledge about AIDS and HIV Transmission in Paramedical personnel working in Benha Hospitals. The Journal of Egyptian Public Health Association. 1993;LXVIII(1,2):143–159. [PubMed] [Google Scholar]
- 12.Diclemente RJ, Boyer DB, Moraies ES. Minorities and AIDS : knowledge, attitudes and misperceptions among Black and Latin adolescents. Am J Public Health. 1988;78:55–7. doi: 10.2105/ajph.78.1.55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Keeter S, Bradford JB. knowledge of AIDS and related behavior change among unmarried adults in a low prevalence city. Am J Prev Med. 1988;4:146–152. [PubMed] [Google Scholar]
- 14.Hardy AM, Dawson DA. Advance data from vital and health statistics, No. 175. Hyattsville, M.D: National Center for Health Statistics; 1989. AIDS knowledge and attitudes. Provisional data from the National Health Interview Survey. [PubMed] [Google Scholar]
- 15.Park K. Park's Textbook of Preventive and Social Medicine. 15th edition. PREM NAGAR Jabalpur, 482 001 (India): Banarsidas Bhanot Publishers 1167; 1997. Health Education and Communication; pp. 586–92. [Google Scholar]
- 16.Kelly RB, Falvo DR. Patient Education. In: Rakel RE, editor. Textbook of Family Practice. 5th edition. Philadelphia: W-B. Saunders Company. A Division of Harcourt Brace Company; 1995. pp. 278–90. [Google Scholar]