

Abstract
Objective:
To study the reported practices of knowledge about and attitude towards smoking among nursing and medical laboratory technology (MLT) students, College of Medicine, King Faisal University at Dammam and Al-Khobar.
Setting:
College of Medicine, Dammam and King Fahd Hospital of the University, Al-Khobar, Saudi Arabia
Methods:
A cross-sectional approach involving a sample of 266 students and interns (152 nursing and 114 MLT), which included all enrolled students in the academic year (1998/1999). A self-administered questionnaire was used to collect data covering knowledge, practice and attitude to smoking. SPSS was used for statistical analysis.
Results:
The overall smoking prevalence was low (5.6%), slightly higher among nursing (6.6%) versus MLT (4.4%) students. Knowledge of and attitude towards smoking was generally satisfactory in both groups, although deficient in some key areas, such as the addictive nature of smoking, some of its consequences on health, and difficulty of quitting.
Conclusion and Recommendations:
The prevalence of smoking among nursing and MLT students is generally low but their knowledge and attitude need improvement. Health education on facts, dangers and consequences of smoking should start as early as the primary school, and should continue throughout the education of future health professionals (role models for the community).
Keywords: Smoking, tobacco consumption, university students, nursing, laboratory technology, knowledge/attitudes/practice (KAP), Saudi Arabia
INTRODUCTION
Smoking is still the single greatest preventable cause of premature death and disability in modern times.1 It has been estimated that one third of the world's population, above 15 years of age, are current smokers. It is much more prevalent among males (47%) than females (12%).2 Tobacco consumption does not only pose multiple health risks (respiratory, cardiovascular, gastrointestinal, genito-urinary), but also adversely affects the lives of individuals, their families and communities, socially, economically and hence developmentally.3,4 Smoking places are the heaviest morbidity and mortality burden on people, compared to any other risk factor.1 The estimated annual death rate of about 3.5-4 million people is expected to rise to 10 millions by the 2020s - 2030s, 7 million of which will occur in developing countries.2 To compensate for the deaths, tobacco companies need to recruit 11,000 new smokers daily, especially “young adolescents”, to maintain the size of their business.5 Most smokers (78-90%) take up the habit during adolescence (10-19 years); less than 2% of them start smoking after their 22nd birthday.3,5
Students in the countries of Gulf Cooperation Council (GCC) have estimated that the prevalence of smoking among male secondary students ranges from 12-50%.6–11 Among GCC male medical students, the rate of prevalence was 13.6-33%, compared to only 2.3-8.6% among female medical students (12-16). Very few studies have been done among the students of the allied sciences. However, Saeed reported that smoking prevalence among students of the allied medical sciences in Riyadh from 12.4% among females to 46.8% among males;17 but was much lower (8-17.5%) among students of the secondary health institutes in Riyadh.18 While several studies have looked into the knowledge and practice of smoking among secondary school or medical students in the central and South-Western Saudi Arabia,7–9,12–14 to the best of our knowledge there has been no study of nursing or medical laboratory technology (MLT) university students in the Eastern Province. This work is aimed at exploring the patterns of smoking among nursing and MLT students and interns of King Faisal University College of Medicine to estimate the magnitude of the problem; assess their knowledge on smoking and find out their attitude towards the habit. This will help us make suitable recommendations for its control.
MATERIAL AND METHODS
This was a cross-sectional study of nursing and MLT students at King Faisal University, Dammam, Saudi Arabia in 1998/1999. All students and interns enrolled in the nursing and MLT Departments during the academic year were included in the study sample (overall n=266; with nursing n1=152 and MLT n2=114). All students were included in the study to ensure an adequate sample size.
A self-administered Arabic questionnaire, modified from the World Health Organization tools was used.19–20 The questionnaire was first tested in a pilot study of medical students. They were therefore, not included in the current study sample. Any ambiguous questions were adjusted accordingly. The nursing and MLT students (1998/1999) were then asked to complete the questionnaire after the objectives of the study and contents of the study tool (questionnaire) had been classified by a member of the research team. The questionnaire, which had been explained to the students, included 3 groups of questions. The first elicited demographic information, such as college year, age, sex, marital status, nationality, residence, parents’ education, parents’ occupation and smoking status. The second group of questions inquired about pattern of smoking behaviour: e.g. type, duration, frequency, age/source/cause/ where the habit began. WHO definitions of current and ex-smoking status were adopted.19 The third group included questions about attitude towards smoking and smokers. After the data collection, all the information was entered into the computer and checked. Using the SPSS/PC programme it was transferred for analysis after it had been rechecked for accuracy.21 Univariate and bivariate analyses of the reviewed data were used, as appropriate. The level of significance was set at <0.05 throughout the study.
RESULTS
Tables 1 to 3 reflect the attributes of the practice of tobacco consumption in the study sample (n=266). The mean age of students and interns studied was 19.7 ± 1.8 years (ranging from 16-30 years). As shown in Table 1, only 15 of them were smokers (5.6%), but the prevalence was higher among nursing students (6.6%), compared to MLT students (4.4%). Of the MLT group showed the highest prevalence of smoking was among the interns (27.3%), while the prevalence was highest among the second year students in the nursing group (13.8%).
Table 1.
Prevalence of smoking comparing nursing with MLT female students and interns by specialty and school year, 1998-1999
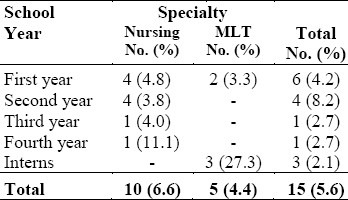
Table 3.
Distribution of smokers according to selected variables 1998-1999
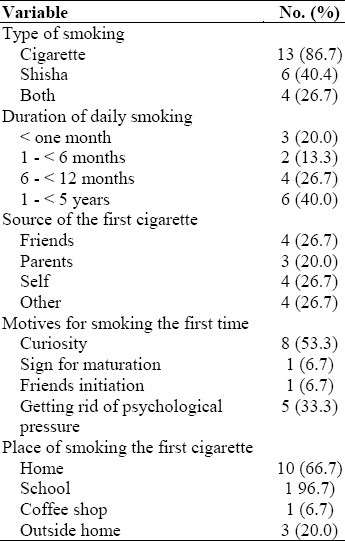
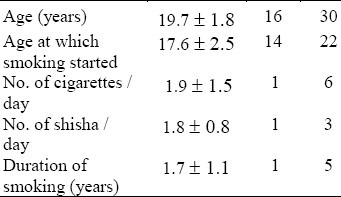
As shown on Table 2, the mean age at which smoking started was 17.6 ± 2.5 years (ranging from 14 - 22 years), with a mean duration of 1.7 ± 1.1 years. As shown on Table 3, most smokers (86.7%) smoked only cigarettes or shisha (water-pipe) as well the quantity, ranging from 1 - 6 cigarettes per day. Two thirds of the smokers (66.7%) have been smoking daily for the last 6 months - 5 years. Almost half the smokers (46.7%) indicated that friends or parents had been the source of the first cigarette. Curiosity (53.5%), and stress (33.3%) were the most important reported motives for initiating the habit. Most of the smokers (66.7%) had started the habit at home.
Table 2.
Characteristics of smokers among nursing and MLT students and interns, 1998-1999
For Tables 4 and 5, the mentioned numbers represent the percentage of students who responded with “true” to these statements (i.e., agreed to the statement, whether “true” or “false” is the correct response). Table 4 deals with a comparison between the views of MLT students and interns and nursing students on tobacco use. It also deals with those who have never smoked as against those who have. For most statements (referred to as Group A), “true” is the correct answer; except for the two (referred to as Group B “some types of cigarettes are harmless”) to which “false” is the correct response and “quitting smoking is too difficult” (74.1 - 97.7%). Except for the statement: “Smoking may lead to stomach cancer” which was wrongly responded to by more than half the participants of the study (54.1%) Group A responded to most statements correctly. Group B, generally got the two questions correct (only 13.9 - 28.9%) agreed to these false statements). There was a statistically significant difference between the nursing and MLT with regard to their percent correct responses to some statements such as: “Smoking increases the heart rate”, “smoking leads to addiction” and “Quitting smoking is too difficult”. A similar difference was observed when the response of those who had never smoked on the statement. “Most of lung cancer patients were regular smokers” were compared with those who had.
Table 4.
A comparison of the knowledge on smoking of nursing with MLT female students and interns by specialty and smoking status, 1998-1999
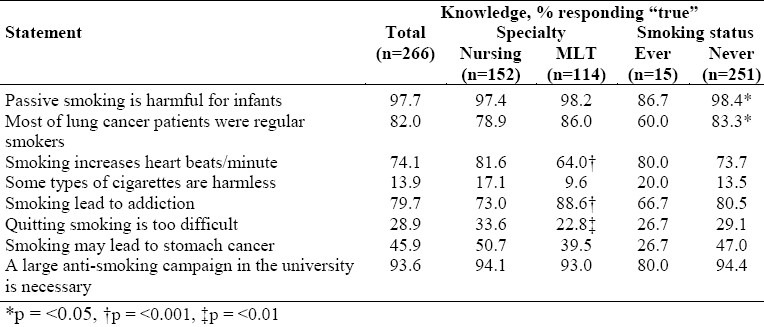
Table 5.
Smoking attitudes comparing nursing with MLT female students and interns by specialty and smoking status, 1998-1999
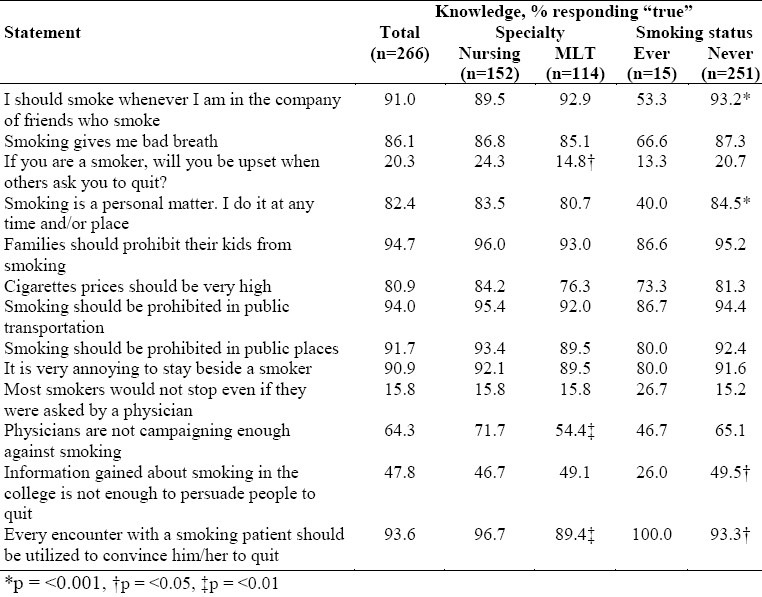
Table 5 compares the attitude of nursing and MLT students/interns; the ‘ever’ and ‘never’ smokers on statements on tobacco use. On the whole (n=266), most statements were responded to correctly, except for three statements which should have been rejected as false. The first was: “I should smoke whenever in the company of smokers”, which was wrongly agreed to by 91% of the respondents. When ‘ever’ with ‘never’ smokers were compared, a highly significant statistical difference was observed (p<0.001). The second statement: “Smoking is a personal matter. I do it in the time/place of my choice,” was wrongly agreed upon by 82.4% of respondents, but similarly when the ‘ever’ with ‘never’ smokers were compared, a highly significant statistical difference was observed (p<0.001). The third statement: “Information gained about smoking in the college is enough for to help people stop smoking”, was agreed upon by 47.8% of respondents, but a comparison of the ‘ever’ with the ‘never’ smokers, revealed a statistically significant difference (p < 0.05).
Only three statements showed a statistically significant difference when nursing and MLT students and interns were compared. These were “Physicians are not doing enough to help people stop smoking”, “If you are a smoker, will you be upset when others ask you to quit”, and “Every encounter with a smoking patient should be utilized to convince him/her to quit”.
DISCUSSION
It has been observed that tobacco consumption in this region has escalated with the rising population, increased purchasing power, especially of the youth, campaigns by tobacco companies, and the increase in the number of girls and women who smoke. Another reason to the lack of awareness of the hazards of smoking, insufficient support and inadequate funds for campaigns against the use of tobacco.22 It is unfortunate that this habit which inevitably results in smoking-related diseases and other subsequent social and economic problems is on the increase.23 This study on female university students and interns, from the nursing and MLT departments of King Faisal University indicated an overall smoking prevalence of 5.6%. In comparison with other Saudi studies on prevalence of smoking among female students, reported by Felimban (1993) as 4.7% among King Saud University medical students;13 by Saeed et al (1993) as 8% in secondary health institutes in Riyadh,18 as high as 12.4% among allied medical sciences students in 1987 was fair.17 It should be emphasized that these figures are low in comparison with female professionals, such as Saudi female physicians (15.8%) as reported in another study by Saeed et al in 1989.24 Even though these figures, ranging from 4.7 - 15.8%, are much lower than those among male students or health professionals, they are quite alarming. Women/mothers who are to be role models for their children, are in continuous contact with their offspring, should be in good health to function efficiently and fulfil their responsibilities to their families as well as their communities. The effect of this new epidemic among women on health and socio-economic conditions if allowed to continue would indeed be disastrous.
According to our study the habit of smoking began between 14-22 years of age. This is quite similar to what was reported by Saeed in two studies in which he stated that 92% of female smokers among Allied Medical Sciences students formed the habit when they were less than 18 years,17 while all female smokers in secondary health institutes started between 10-20 years.18 These figures reaffirm the importance of effective health education as early as possible in life in schools and through the mass media in order to protect children, especially girls, from adopting this dangerous habit.
In this study the most cited motives for the adoption of the habit of smoking were curiosity (53%) followed by relief of stress (33%). This is in agreement with the findings of Abolfotouh et al in 1998,14 where curiosity/ showing off were each mentioned by 52% of the smokers in King Saud University in Abha (currently known as King Khalid University).
Compared to MLT students in our study, the nurses’ knowledge about smoking and its hazards was generally more satisfactory. These results are comparable to the results of other studies on medical students done elsewhere in Saudi Arabia.12–14 The knowledge of smokers as compared to non-smokers did not yield any statistically significant difference. This was not in conformity with the report of Abolfotouh et al,14 which showed that non-smokers were more knowledgeable than smokers. The role of efforts to promote health is again emphasized here. Bridging the gap between knowledge and practice is difficult and requires intensive and collaborative effort on the part of the entire community.
Our findings were similar to those of Abolftouh et al in two studies14,25 on the attitude towards public health drives against smoking in that they were less favorable among smokers compared to non-smokers. A similar pattern was observed for statements of attitude towards time, place and company of smoking, which is again in agreement with the studies mentioned above. Differences in attitude statements between nursing and MLT students strongly reflected the background or training offered to each group. The nurses’ attitude was more inclined towards the clinical sciences and patient satisfaction whereas MLTs focus more on laboratory technology studies.
In conclusion, an effective sound education on tobacco consumption should be incorporated into our educational system, commencing as early as the primary schools. In addition, the media engagement in this drive to control tobacco use should be intensified to reach the entire community. There should be a vigorously pursuit of this objective through curricula designed for future health professionals, including nursing and MLT departments of universities. These professionals should be able to provide sound advice to the public on the one hand (as through health promotion and education activities), as well as present themselves good role models for their communities.
REFERENCES
- 1.Last J. Social and behavioral determinants of health. In: Last J, editor. Public health and human etiology. Second edition. Stanford, Connecticut: Appleton & Lange; 1998. [Google Scholar]
- 2.Geneva: WHO; 1998. WHO. Growing up without tobacco. [Google Scholar]
- 3.Novotny TE, Giovino GA. Tobacco use. In: Brownson RC, Remington PL, Davis JR, editors. Chronic disease epidemiology and control. Washington DC: American Public Health Association; 1998. pp. 117–48. [Google Scholar]
- 4.Meltzer EO. Prevalence, economic and medical impact of tobacco smoking. Ann Allergy. 1994;73:381. [PubMed] [Google Scholar]
- 5.Gezairy HA. Alexandria: WHO/EMRO; 1998. Regional Director's message. World No-Tobacco Day, 31 May 1998. [Google Scholar]
- 6.Geneva: WHO; 1997. WHO. Tobacco or health: A global status report. [Google Scholar]
- 7.Rowlands DF, Shopster PJ. Cigarette smoking amongst Saudi school boys. Saudi Med J. 1987;8:613–8. [Google Scholar]
- 8.Felimban FM, Jarallah JS. Smoking habits of secondary school boys in Riyadh, Saudi Arabia. Saudi Med J. 1994;15:438–42. [Google Scholar]
- 9.Jarallah J, Bamgboye EA, Al-Ansary LA, Kalantan KA. Predictors of smoking among male junior secondary school students in Riyadh, Saudi Arabia. Tobacco Control. 1996;5:26–9. doi: 10.1136/tc.5.1.26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Muscat, Oman: General Directorate of Health, Ministry of Health; 1997. Ministry of Health. Extent of knowledge, attitude and practice of school students with respect to nutrition, hygiene and smoking (Arabic). Preliminary report. [Google Scholar]
- 11.Haddad N. Smoking among secondary male students in Bahrain. Family Practice Residency Program. Ministry of Health, Bahrain. 1998 [Google Scholar]
- 12.Jarallah J. Smoking habits of medical students at King Saud University, Riyadh. Saudi Med J. 1992;13:510–13. [Google Scholar]
- 13.Felimban FM. The smoking practices and attitudes towards smoking of female university students in Riyadh. Saudi Med J. 1993;14:220–4. [Google Scholar]
- 14.Abolfotouh M, Adel-Aziz M, Alakija W, et al. Smoking habits of King Saud University students in Abha, Saudi Arabia. Ann Saudi Med. 1998;18:212–6. doi: 10.5144/0256-4947.1998.212. [DOI] [PubMed] [Google Scholar]
- 15.Hamadeh RR. Smoking habits of medical students in Bahrain. J Smoking-related Diseases. 1994;15:189–95. [Google Scholar]
- 16.Tessier JF, Freour PP, Nejjari C, et al. Smoking behaviour and attitudes of medical students towards smoking and anti-smoking campaigns: a survey in 10 African and middle-eastern countries. Tobacco Control. 1992;1:95–101. [Google Scholar]
- 17.Saeed AAW. Smoking habits of students in College of Allied Medical Sciences, Riyadh. J Roy Soc Health. 1987;5:187–8. doi: 10.1177/146642408710700511. [DOI] [PubMed] [Google Scholar]
- 18.Saeed AAW, Al-Johali E, Al-Shahry AH. Smoking habits of students in secondary health institutes in Riyadh city, Saudi Arabia. J Roy Soc Health. 1993;11:132–5. doi: 10.1177/146642409311300308. [DOI] [PubMed] [Google Scholar]
- 19.Geneva: WHO; 1996. WHO/Tobacco or Health Program. Guidelines for controlling and monitoring the tobacco epidemic. [Google Scholar]
- 20.Report of WHO Meeting, Winnipeg, Canada, July 7-9, 1983. Geneva: WHO; 1984. WHO. Guidelines for the conduct of tobaccosmoking surveys among health professionals. [Google Scholar]
- 21.Chicago, Illinois, USA: 1996. SPSS-PC (Statistical Package for Social Sciences). 444 N. Michigen Ave. [Google Scholar]
- 22.WHO. Plan of action for tobacco control in the Eastern Mediterranean Region. East Med Health J. 1997;3:168–75. [Google Scholar]
- 23.Bakhotmah MA. The epidemic of smoking in Saudi Arabia. Saudi Med J. 1996;17:416–7. [Google Scholar]
- 24.Saeed AAW, Taha AM, Shahri AH. Smoking habits of physicians in Riyadh, Saudi Arabia. Saudi Med J. 1989;10:508–11. [Google Scholar]
- 25.Abolfotouh MA, Abdel-Aziz M, Badawi IA, Alakija W. Smoking intervention program for male secondary-school students in south-western Saudi Arabia. East Med Health J. 1997;3:90–100. [PubMed] [Google Scholar]