

Abstract
Objective:
The objective of this study was to validate an Arabic version of the General Health Questionnaire (GHQ-28) in a primary care setting in Saudi Arabia.
Methodology:
A total of 60 Saudi patients selected by means of systematic random sampling were asked to fill out the GHQ-28 Arabic version. The psychiatrist interviewed all patients using the Arabic version of the Clinical Interview Schedule (CIS).
Results:
The best cut-off level for the GHQ-28 indicating best trade-off between sensitivity and specificity was 4/5, where the validity values were, sensitivity; 72%, specificity; 74%, positive predictive value; 72%, negative predictive value; 74% and misclassification rate; 27%. The correlation coefficient was r = +0.61 and the Spearman's Rank-difference correlation was rs = +0.57. The area under the ROC Curve was 69%. The cut-off point 4/5 in this study is the same as recommended by others in primary care settings. Although the validity parameters are relatively low, they are within the range found by other studies in USA, UK and developing countries. This supports the suggestion to develop an Arabic Screening Questionnaire based on the translated GHQ with the addition of culturally specific items.
Conclusion:
The GHQ-28 Arabic Version is a valid instrument that may be of great help to primary care doctors in improving detection of psychiatric morbidity and in epidemiological research.
Keywords: General Health Questionnaire, Primary Care, Saudi Arabia
INTRODUCTION
The General Health Questionnaire (GHQ) in its full 60-items, or abbreviated 30 and 28 items version is by far the most popular screening instrument.1 It is a self-reporting questionnaire developed by Goldberg (1970), to detect functional psychiatric disorders in the community and primary care settings.2,3 It has been extensively tested in various cultures and linguistic groups in primary care and other settings generally showing good validity results.4–9 Tarnopolsky et al suggested that the GHQ should be standardized on the population where it is to be applied, because validity coefficients obtained in one setting do not necessarily hold in another.4 Psychiatric disorders are shown to form a major part of morbidity in Saudi primary health care, and the vast majority of cases are missed.10,11 Therefore, validation of a screening instrument such as the GHQ in the patients’ language takes a little time, and is important in epidemiological research to improve detection and recognition of psychiatric morbidity.3,4 A medline and a Saudi literature search showed no study that validated the GHQ in primary health care in Saudi Arabia.
The objective of the present study was to validate an Arabic version of the GHQ-28 (see appendix) in primary care setting in Saudi Arabia against the Psychiatrist's assessment by means of the Clinical Interview Schedule (CIS).
Appendix.
METHODOLOGY
Subjects: The study was carried out in the primary care center attached to King Abdulaziz University Hospital. It is situated in the center of Riyadh and serves mostly a Saudi population of different social classes. The study population included patients of both sexes above 14 years of age attending the primary care clinics for any reason.
A total of 60 Saudi patients selected by means of systematic random sampling were asked to fill out the GHQ-28 Arabic version while waiting to be seen by their doctor. Patients who were found to be illiterate or experienced difficulty in filling out the questionnaire were helped by a trained nurse.
All patients were interviewed by the first author, a consultant psychiatrist with eleven years post-qualification experience, using the Arabic version of the CIS. Each patient was given a score on the psychiatric severity rating (0-4) as follows: 0=no psychiatric disturbance, 1=mild subclinical psychiatric disturbance, 2=clinically significant (mild) psychiatric disturbance, 3=clinically significant (moderate) psychiatric disturbance, 4=clinically significant (marked) psychiatric disturbance.
Instruments: For the present study the instruments CIS and GHQ-28 were translated into Arabic by two Arab psychiatrists. The reliability of the Arabic versions was checked with a translation into English by another psychiatrist who had no knowledge of the instrument and they were found to be in close agreement. The underlying assumption is that the psychiatrist's assessment using the CIS is the gold standard against which the GHQ-28 is compared. The CIS is divided into four sections containing ratings based on symptoms reported by the patient (arranged in ten groups), twelve items that represent the interviewer's view of the manifest abnormalities and an ICD clinical diagnosis. The scoring of the GHQ-28 depends on the response category the patient chooses for each of the 28-items and the scoring developed by Goldberg (1970) was used to count responses in codes 3 and 4 only. The GHQ-28 version was chosen for the study because it was short and was found to be more valid than both the GHQ-12 and the GHQ-30.12
Validation parameters: The validity of the GHQ-28 was estimated by the following: evaluating the sensitivity and specificity at best trade-off point; estimating the positive predictive value, the negative predictive value and the misclassification rate; determining the simple correlation coefficient (r) and the Spearman's Rank-Difference Correlation values; finding the confidence intervals between observed data values of GHQ-28 and its predicted data values in a scattergram; and using the Receiver (relative) operating characteristic (ROC) analysis. The ROC curve is a graphic representation of the relationship between sensitivity and specificity for a diagnostic instrument. It is constructed by plotting the sensitivity (true positive rate) against the false positive rate (1-specificity) for all possible GHQ-28 cut-off points. The resulting plot, which takes the shape of a curve, is known as a ROC curve (figure 1).13
Figure 1.
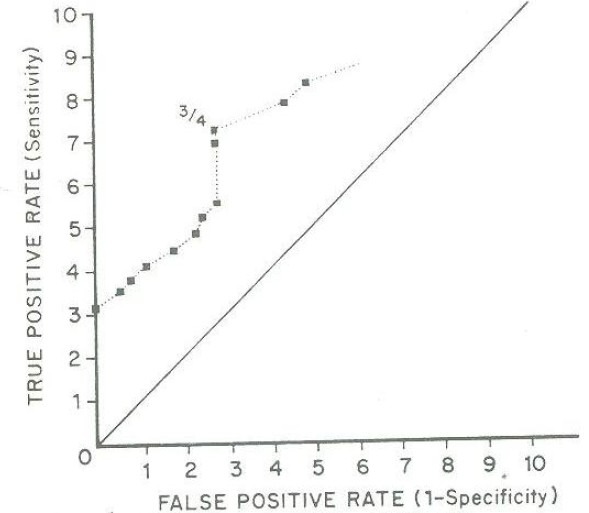
ROC curve of the GHQ-28
RESULTS
A total of sixty patients, 30 males and 30 females were included in the study. The age range was 14-70 and the mean age was 28.1± 10.77. The mean age for males was 29.17 ± 10.99 and for females was 27.1 ± 10.63.
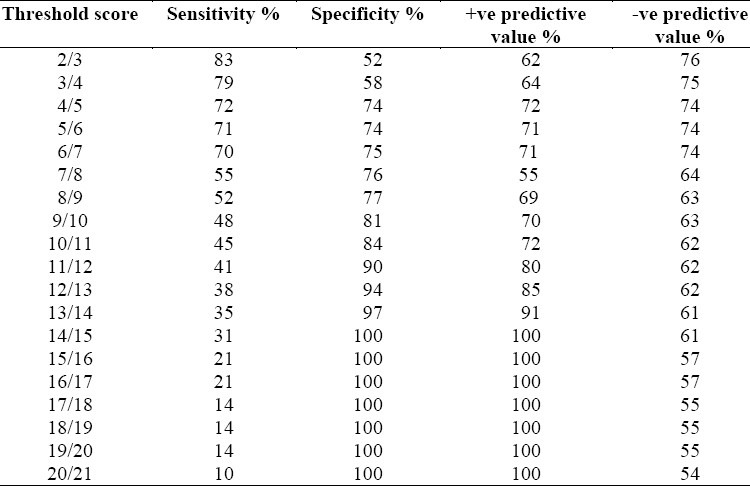
Table 1 shows different cut-off levels of the GHQ-28 (2/3) through (20/21) and their comparable sensitivity, specificity, positive predictive values and negative predictive values. Patients who scored above these threshold levels were considered as probable cases while those who scored below them were considered probable normals. The overall best cut-off level indicating the best diagnostic ability of the GHQ-28 was found to be 4/5, where the misclassification rate was 27%, the sensitivity was 72%, the specificity was 74%, the percentage of cases missed was 14%, the positive predictive value was 72% and the negative predictive value was 74%. The validity values for males and females respectively were sensitivity 64% and 80%, specificity 81% and 66.9% and misclassification rate was 26.7% for both sexes.
Table 1.
GHQ-28 threshold scores and their validity parameters
The ROC curve of the GHQ-28 (Figure 1), showed that it was a valid test and the area under the curve measured graphically was 69%. When the GHQ-28 scores were plotted against the CIS overall severity rating scores, the correlation coefficient was r=+0.61 and the p-value approached zero; the Spearman's Rank-difference correlation was rs=+0.57 andthe p-value approached zero which is highly significant (figure 2). The scattergram of data and regression line were also found to be highly significant and the confidence limit was 99.0% (figure 3).
Figure 2.
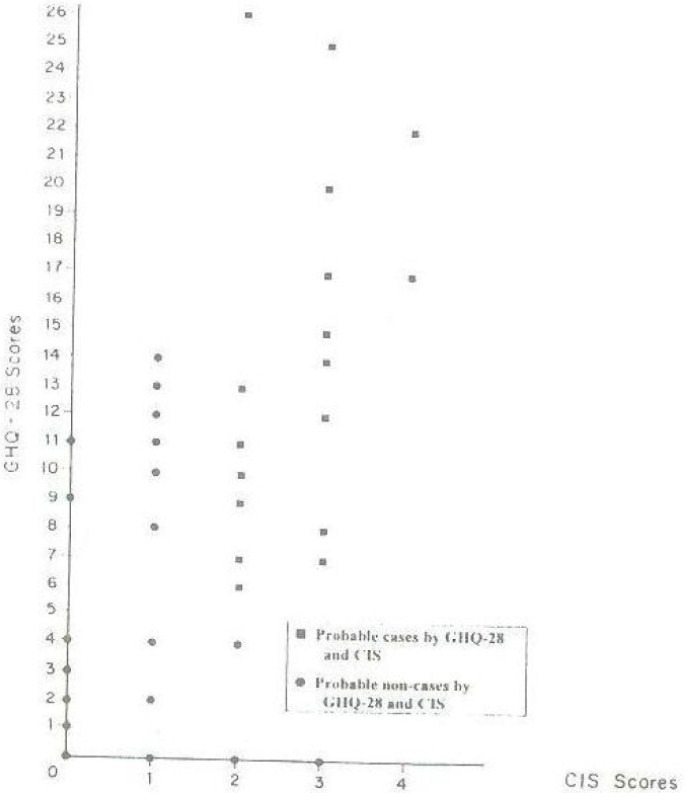
GHQ-28 and CIS scores
Figure 3.

Scattergram of data & regression line & confidence intervals
DISCUSSION
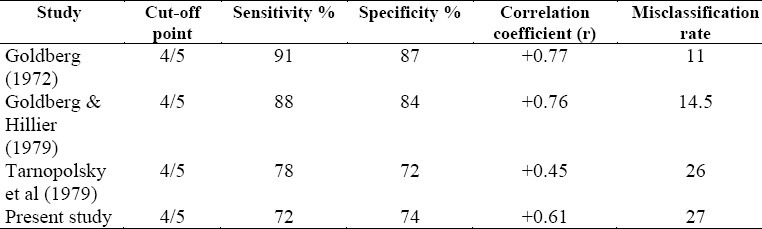
This study has shown that the GHQ-28 is a valid and useful screening instrument of psychiatric morbidity in a primary care setting in Saudi patients. The best cut-off point was found to be 4/5 which is comparable to what was recommended by Goldberg for general practice settings.3 This cut-off point represented the best trade-off between sensitivity (72%) and specificity (74%). Although, the validity of the GHQ-28 in our study was not high, it was still in the range reported in many other studies.4,9,14,15 Even though, Goldberg9 had higher sensitivity and specificity values, other studies conducted in British and United States communities had lower values for sensitivity and specificity comparable to our results.15–17 Table 2 shows data comparing different validation studies of the GHQ-28 in the primary care setting. The relatively lower value of sensitivity for males and specificity for females is consistent with other studies.18,19 On the other hand, since previous studies have not shown strong associations between sex and GHQ validity,2 our results might show that a higher cut-off level may be used for females. This may be explained by the tendency of Saudi females to somatise.13,20 Women in general tend to report more symptoms5 and score high on the GHQ, thus attaining false-positive rates, and reducing the specificity.
Table 2.
GHQ-28 different validation studies
The validity of the GHQ-28 was also shown to be very good by the ROC curve, which had been used previously in the validation of the GHQ-28.5,13,18
The use of longer GHQ versions may increase validity,2,3 but shorter ones such as the GHQ-28 are still valid and take much less time. Primary care physicians miss about 50% of psychiatric cases10,16,21 and the use of the GHQ-28 may be useful to improve detection rate. Goldberg suggests that when a patient is found to have a high score, the most natural response by the clinician is to look at the questionnaire again with the patient and ask additional probing questions suggested by particular symptoms.3,16 It is also important to note that GHQ-28 has been found to have an important role in alerting primary care doctors not to miss new episodes of psychiatric morbidity in patients with chronic physical diseases.16
Hence, GHQ-28 is useful in epidemiology.3,4,16,18 The present validation study is also important for researchers who intend to estimate the prevalence of psychiatric disorders in primary care in the Saudi communities and plan services to improve recognition and diagnosis of psychiatric morbidity in primary care.
The fairly low validity in our study conforms with other validity studies in developing countries and may strongly support the suggestion by other researches22,23 to develop and validate a new Arabic screening questionnaire that builds on the translated GHQ with the addition of specific items relevant to the Saudi culture for the identification of psychiatric morbidity.
REFERENCES
- 1.Mayou R, Hawton K. Psychiatric disorders in the General Hospital. British J Psych. 1986;149:172–90. doi: 10.1192/bjp.149.2.172. [DOI] [PubMed] [Google Scholar]
- 2.Goldberg D. Manual of the General Health Questionnaire. Windsor (UK): National Foundation for Educational Research; 1978. [Google Scholar]
- 3.Goldberg D. Use of the General Health Questionnaire in Clinical Work. BMJ. 1986;293:1188–9. doi: 10.1136/bmj.293.6556.1188. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Tarnopolsky A, Hand DJ, Mclean EK. Validity and uses of a screening questionnaire (GHQ) in the community. British J Psych. 1979;134:508–15. doi: 10.1192/bjp.134.5.508. [DOI] [PubMed] [Google Scholar]
- 5.Bridges KW, Goldberg DP. The validation of the GHQ-28 and the use of the MMSE in neurological inpatients. British J Psych. 1986;148:548–53. doi: 10.1192/bjp.148.5.548. [DOI] [PubMed] [Google Scholar]
- 6.Mari JJ, Williams P. Minor psychiatric disorder in primary care in Brazil: A pilot study. Psychological Medicine. 1984;14:223–72. doi: 10.1017/s0033291700003263. [DOI] [PubMed] [Google Scholar]
- 7.Cheng TA. A pilot study of mental disorders in Taiwan. Psychological Medicine. 1985;15:195–204. doi: 10.1017/s0033291700021061. [DOI] [PubMed] [Google Scholar]
- 8.Sato T, Takeichi M. Lifetime prevalence of specific disorders in a general medicine clinic. General Hospital Psychiatry. 1993;15:224–33. doi: 10.1016/0163-8343(93)90037-o. [DOI] [PubMed] [Google Scholar]
- 9.Goldberg DP, Blackwell B. Psychiatric illness in general practice: a detailed study using a new method of case identification. BMJ. 1970;2:439–43. doi: 10.1136/bmj.2.5707.439. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Al-Faris EA, Alhamad A, Al-Shammari S. Hidden and conspicuous psychiatric morbidity in Saudi primary health care (A pilot study) The Arab J of Psychiatry. 1995;6:162–75. [Google Scholar]
- 11.Al-Faris E, Al-Subaie A, Khoja T, Al-Ansary L, Abdul-Raheem F, Al-Hamdan N, et al. Training primary health care physicians in Saudi Arabia to recognise psychiatric illness. Acta Psychiatr Scand. 1997;96:439–44. doi: 10.1111/j.1600-0447.1997.tb09945.x. [DOI] [PubMed] [Google Scholar]
- 12.Banks MH. Validation of the General Health Questionnaire in a young community sample. Psychological Medicine. 1983;13:349–53. doi: 10.1017/s0033291700050972. [DOI] [PubMed] [Google Scholar]
- 13.Ly Kouras, Adrachta D, Kalfakis N, Oulis P, Voulgani A, Christodoulu GN, et al. GHQ-28 as an aid to detect mental disorders in neurological inpatients. Acta Psychiatr Scand. 1996;93:212–6. doi: 10.1111/j.1600-0447.1996.tb10634.x. [DOI] [PubMed] [Google Scholar]
- 14.Goldberg DP. The detection of psychiatric illness by questionnaire. London: Oxford University Press; 1972. [Google Scholar]
- 15.Goldberg D. Identifying psychiatric illness among general medical patients. BMJ. 1985;291:161–2. doi: 10.1136/bmj.291.6489.161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Wright AF, Perini AF. Hidden psychiatric illness: use of the general health questionnaire in General Practice. Journal of the Royal College of General Practitioners. 1987;37:164–7. [PMC free article] [PubMed] [Google Scholar]
- 17.Cleary PD, Goldberg ID, Kessler IG, Nyez GR. Screening for mental disorder among primary care patients. Archives of general psychiatry. 1982;39:837–40. doi: 10.1001/archpsyc.1982.04290070065012. [DOI] [PubMed] [Google Scholar]
- 18.Stanfeld SA, Marmot MG. Social class and minor psychiatric disorder in British civil servants: a validated screening survey using the GHQ. Psychological Medicine. 1992;22:739–49. doi: 10.1017/s0033291700038186. [DOI] [PubMed] [Google Scholar]
- 19.Hobbs P, Ballinger CB, Greenwood C, Martin B, McClure A. Factor analysis and validation of the General Health Questionnaire in men: A general practice survey. British J Psych. 1984;144:270–5. doi: 10.1192/bjp.144.3.270. [DOI] [PubMed] [Google Scholar]
- 20.Racy J. Somatisation in Saudi women: a therapeutic challenge. British J Psych. 1980;137:212–6. doi: 10.1192/bjp.137.3.212. [DOI] [PubMed] [Google Scholar]
- 21.Goldberg D, Steele JJ, Johnson A, Smith C. Ability of Primary Care Physicians to make accurate ratings of psychiatric symptoms. Archives of General Psychiatry. 1982;39:829–33. doi: 10.1001/archpsyc.1982.04290070059011. [DOI] [PubMed] [Google Scholar]
- 22.Fontanesi F, Gobetti C, Zumermann-Tansella CH, Tansella M. Validation of the Italian version of the GHQ in a general practice setting. Psychological Medicine. 1985;15:411–15. doi: 10.1017/s0033291700023710. [DOI] [PubMed] [Google Scholar]
- 23.Cheng T, Williams P. The design and development of a screening questionnaire (CHQ) for use in community studies of mental disorders in Taiwan. Psychological Medicine. 1986;16:415–22. doi: 10.1017/s0033291700009247. [DOI] [PubMed] [Google Scholar]