

Abstract
Alveolar soft part sarcoma (ASPS) is a rare malignant soft tissue tumor, mainly localized in the extremities, occurring principally in adolescents and young adults. ASPS is uncommon in the female genital tract , and only 37 cases have been reported so far, including 9 cases in the uterine corpus and 17 cases in the uterine cervix. We here reported a case of ASPS occurring in the lower uterine segment . The case showed typical histological and immunohistochemical features. The patient had pelvic and para-aortic lymph node metastasis. To the best of our knowledge, it is the first such case described.
Keywords: Alveolar soft part sarcoma of the uterine corpus, uterine, female genital tract
Report of case
Clinical presentation
A 57-year-old postmenoposal woman, gravida 2, para 2, with anemic for 2 years, was hospitalized because of abnormal uterine bleeding for 3 months. Ultrasonic examination and computed tomography (CT) examination revealed a mass lesion, 2.4cm in diameter, mainly located in the endometrium of lower uterine segment. Magnetic resonance imaging (MRI) and CT showed no lesions in the chest, abdomen, or extremities. Cervical Pap test showed atypical cells suggestive of malignancy. Subsequent endometrial biopsy indicated a lower-grade malignant tumor with uncertain histological type. Total hysterectomy and bilateral salpingo-oophorectomy with dissection of pelvic and para-aortic lymph nodes were performed. During the procedure enlarged paraaortic lymph nodes were noted, but no other peritoneal lesions were found. Intraoperative pelvic washing cytology was negative for malignant cells.
The patient was readmitted for further examination one month after the surgery. No abnormalities were found in both physical examination and imagine studies. No adjuvant chemotherapy was given. The patient was free of disease 9 months after the surgery.
Pathological findings
Gross examination revealed an exophytic tumor, measuring 2.4×2.0x1.8cm, located mainly in the lower uterine segment. The tumor was sharply demarcated mass and had a smooth and homogeneous, yellow-whitish surface.
The tumor was grayish, solid, with a slightly irregular border (Figure 1). The perimetrium, uterine cervix, and bilateral adnexas were unremarkable. Para-aortic lymph nodes were 1.2cm in aggregate.
Figure 1.

Tumor located mainly beneath the endometrium of lower uterine segment, measuring 2.4×2.0 cm.
Histologically, the tumor was composed of large, round, and polygonal neoplastic cells with distinct cell borders and abundant granular eosinophilic and vacuolated cytoplasm. Most of the tumor cells had vesicular nuclei with prominent nucleoli (Figure 2). The tumor grew in a nest-like or organoid pattern separated by delicate fibrovascular septa (Figure 3, 4) Mitotic figures were not identified. The mass was relatively well circumscribed, except for a peripheral group of tumor cells infiltrating the surrounding fibromuscular tissue. The tumor was confined to the subendometrium of the lower uterine segment, with no involvement of the mucosa of the endocervix, or paracervical soft tissue. The remainder of the uterus showed no evidence of tumor.
Figure 2.
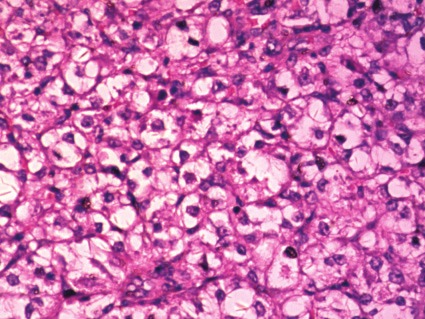
Tumor cells had vesicular nuclei with prominent nucleoli.
Figure 3.

Tumor cells arranged in a nest-like ororganoid pattern separated by delicate fibrovascularsepta.
Figure 4.

Figure 2 amplification.
Periodic acid-Schiff (PAS) stain revealed intracellular diastase-resistant granules. PAS-positive rod-like or rhomboid crystals of Some cells were identified after diastase digestion (Figure 5). The cytomorphological features of the metastatic tumor in para-aortic lymph nodes were the same as the tumor in the lower uterine segment (Figure 6).
Figure 5.

PAS-positive diastase-resistant intracytoplasmic crystals.
Figure 6.
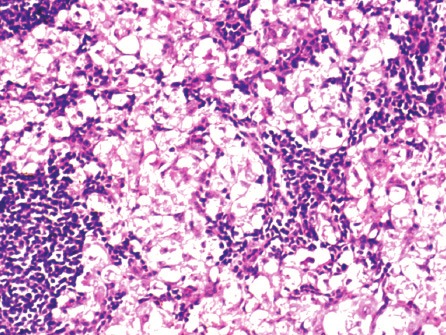
The metastatic carcinoma of paraaorticlymph nodes was the same as beneath theendometrium carcinoma of lower uterine segment.
Immunohistochemical stains were negative for AE1/AE3, EMA, SMA, desmin, S-100, HMB45, CD10, Syn, and chromogranin, CD34, VIM, 34βE12. Ki-67 was positive in 5% tumor cells. However, the tumor cell nuclei was strongly and diffusely positive for TFE3 (Figure 7), with a polyclonal anti-TFE antibody using the avidin-biotin method. Because of the fresh tissue unavailable, the chromosomal translocation, t(X; 17)(p11; q25) involving the TFE3 gene could not detected by reverse transcriptase-polymerase chain reaction.
Figure 7.
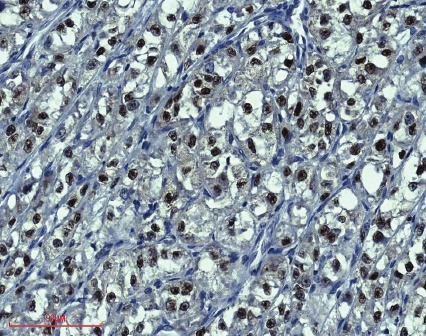
Tumor cells show diffuse nuclear positivity with TEF3.
Discussion
The first case of ASPS arising in the female genital tract was reported in 1976 by Tobon et al [1]. who described ASPS involving in the vagina in 57 year old women.Since then, 35 other cases have been reported [2-31]. Flint et al. [5] reported the first case of ASPS involving the uterine cervix and Grey [13] reported the first case of ASPS involving the uterine fondues. The largest series of ASPS involving the female genital tract (9 cases) was reported by Nielsen et al. in 1995 [19].
Of the 38 cases reported to date (including our case), the tumors involved the vulva (1 case), vagina (6 cases), cervix (17 cases), lower uterine segment/upper cervix (3 cases), uterine corpus (9 cases, including 5 in the myometrium and 4 in the endometrium), and broad ligament (1 case). One of the tumors was described as arising in the uterus, but an exact location was not established [17].
PAS stain was performed in all but two cases [3,20]; 24 of 36 (66.7%) had PAS + diastase-resistant crystals. PAS + diastase resistant granules were identified in the 12 remaining cases (including our case). Immunohistochemical staining was performed in the reported cases with variable results. The antibodies included CK, Vimentin, Desmin, SMA, HHF-35, SMKA, Myoglobin, MyoD1, S-100 HMB-45, NSE, NK1-C3, Chromo, Lu-5 and TFE3. The results were not specifically for diagnosis, but usually in an attempt to rule out other tumors in the differential diagnosis. Our case was negative for all the markers tested including AE1/AE3, EMA,SMA, desmin, S-100, HMB 45, CD10, synaptophysin, and chromogranin, except a strong nuclear expression for TFE3.
Argani et al. [31] reported strong nuclear immunoreactivity for TFE3 in tumors characterized by a chromosomal translocation involving the TFE3 gene. All 19 ASPSs and 20 of 21 pediatric renal cell carcinomas with Xp11.2 translocations stained for TFE3. Among 1,476 other tumors from 16 different organ sites, only 6 were positive (sensitivity 97.5%, specificity 99.6%). In our case, the tumor cells were strongly positive for TFE3. The result was same as the case reported by Roma [24]. To the best of our knowledge, this is the second female genital tract ASPS reported with positive immunoreactivity for TFE3.
Among 38 cases in GYN, only 3 of cases had TFE stains, all cases were positive. Among the ASPS cases with the involvement of female genital tract , ASPSs in the uterine corpus and cervix have an apparently good prognosis compared that in the female genital tract other than uterus . Majority cases (0/9) of ASPS involving the uterine corpus were not associated with recurrence. The case during the procedure enlarged para-aortic lymph nodes were noted. Of the 20 cases involving the cervix/lower uterine segment, only one patient showed tumor metastasis [5], one recurred twice after the patient was treated with cryotherapy prior to the correct diagnosis was rendered [8], and 1 case recurred 4 years after an excisional biopsy [17]. All patients with uterine ASPS with follow-up were alive and well at the time of last follow-up. In contrast, one of six patients with vaginal ASPS died as a result of the tumor. This patient had a recurrence 4 months after local excision and external radiation therapy for a 3-cm, right vaginal wall mass. The patient died of the disease with pulmonary metastases 25 months later [4,6]. Another patient had a recurrent 1.5-cm mass found 4 months after the initial diagnosis [10]. We here report the case involving the lower uterine segment with paraortic lymph node metastasis. To the best of our knowledge, this is the first case that patient had such presentation.
The relatively favorable prognosis of ASPS in the female genital tract (in contrast to other sites) might be related to the relatively small tumor size (<5 cm) of the tumors in almost all the cases. Roma reported a case with a total abdominal hysterectomy for uterine leiomyomas. a ASPS tumor with small size was identified accidently . The abnormal uterine bleeding may be the most symptom for the patients with ASPS in low female genital tract. Of the 20 cases arising in the cervix or lower uterine segment previously reported in the literature, 16 (80%) patients had abnormal uterine bleeding. Of the four remaining cases, two patients had a cervical nodule identified preoperatively and the other two had severe menstrual cramping. In our case, the patient had severe dysmenorrhea before the imaging examination revealed a tumor involving the lower uterine segment and upper endocervix. The patient was well without any evidence of recurrence for 9 months after the surgery. Larger number of cases with longer follow up will help to understand the nature of these unusual cases.
References
- 1.Tobon H, Amortegui AJ, Murphy AI. Alveolar soft part sarcoma of the vagina. Pa Med. 1976;79:55–57. [PubMed] [Google Scholar]
- 2.Kasai K, Yoshida Y, Okumura M. Alveolar soft part sarcoma in the vagina: clinical features and morphology. Gynecol Oncol. 1980;9:227–236. doi: 10.1016/0090-8258(80)90031-1. [DOI] [PubMed] [Google Scholar]
- 3.Shen JT, D’Ablaing G, Morrow CP. Alveolar soft part sarcoma of the vulva: report of first case and review of literature. Gynecol Oncol. 1982;13:120–128. doi: 10.1016/0090-8258(82)90017-8. [DOI] [PubMed] [Google Scholar]
- 4.Chapman GW, Benda J, Williams T. Alveolar soft-part sarcoma of the vagina. Gynecol Oncol. 1984;18:125–129. doi: 10.1016/0090-8258(84)90016-7. [DOI] [PubMed] [Google Scholar]
- 5.Flint A, Gikas PW, Roberts JA. Alveolar soft part sarcoma of the uterine cervix. Gynecol Oncol. 1985;22:263–267. doi: 10.1016/0090-8258(85)90037-x. [DOI] [PubMed] [Google Scholar]
- 6.Zaleski S, Setum C, Benda J. Cytologic presentation of alveolar soft-part sarcoma of the vagina. A case report. Acta Cytol. 1986;30:665–670. [PubMed] [Google Scholar]
- 7.Kopolovic J, Weiss DB, Dolberg L, Brezinsky A, Ne’eman Z, Anteby SO. Alveolar soft-part sarcoma of the female genital tract. Case report with ultrastructural findings. Arch Gynecol. 1987;240:125–129. doi: 10.1007/BF02134046. [DOI] [PubMed] [Google Scholar]
- 8.Abeler V, Nesland JM. Alveolar soft-part sarcoma in the uterine cervix. Arch Pathol Lab Med. 1989;113:1179–1183. [PubMed] [Google Scholar]
- 9.Carinelli SG, Giudici MN, Brioschi D, Cefis F. Alveolar soft part sarcoma of the vagina. Tumori. 1990;76:77–80. doi: 10.1177/030089169007600121. [DOI] [PubMed] [Google Scholar]
- 10.Chang HC, Hsueh S, Ho YS, Chang MY, Soong YK. Alveolar soft part sarcoma of the vagina. A case report. J Reprod Med. 1994;39:121–125. [PubMed] [Google Scholar]
- 11.Burch DJ, Hitchcock A, Masson GM. Alveolar soft part sarcoma of the uterus. case report and review of the literature. Gynecol Oncol. 1994;54:91–94. doi: 10.1006/gyno.1994.1172. [DOI] [PubMed] [Google Scholar]
- 12.Foschini MP, Eusebi V, Tison V. Alveolar soft part sarcoma of the cervix uteri. A case report. Pathol Res Pract. 1989;184:354–358. doi: 10.1016/S0344-0338(89)80099-8. discussion 359-360. [DOI] [PubMed] [Google Scholar]
- 13.Gray GF Jr, Glick AD, Kurtin PJ, Jones HW 3rd. Alveolar soft part sarcoma of the uterus. Hum Pathol. 1986;17:297–300. doi: 10.1016/s0046-8177(83)80223-8. [DOI] [PubMed] [Google Scholar]
- 14.Sahin AA, Silva EG, Ordonez NG. Alveolar soft part sarcoma of the uterine cervix. Mod Pathol. 1989;2:676–680. [PubMed] [Google Scholar]
- 15.Nolan NP, Gaffney EF. Alveolar soft part sarcoma of the uterus. Histopathology. 1990;16:97–99. doi: 10.1111/j.1365-2559.1990.tb01071.x. [DOI] [PubMed] [Google Scholar]
- 16.Guillou L, Lamoureux E, Masse S, Costa J. Alveolar soft-part sarcoma of the uterine corpus: histological, immunocytochemical and ultrastructural study of a case. Virchows Arch A Pathol Anat Histopathol. 1991;418:467–471. doi: 10.1007/BF01605935. [DOI] [PubMed] [Google Scholar]
- 17.Heimann P, Devalck C, Debusscher C, Sariban E, Vamos E. Alveolar soft-part sarcoma: further evidence by FISH for the involvement of chromosome band 17q25. Genes Chromosomes Cancer. 1998;23:194–197. [PubMed] [Google Scholar]
- 18.Morimitsu Y, Tanaka H, Iwanaga S, Kojiro M. Alveolar soft part sarcoma of the uterine cervix. Acta Pathol Jpn. 1993;43:204–208. doi: 10.1111/j.1440-1827.1993.tb01133.x. [DOI] [PubMed] [Google Scholar]
- 19.Nielsen GP, Oliva E, Young RH, Rosenberg AE, Dickersin GR, Scully RE. Alveolar soft-part sarcoma of the female genital tract: a report of nine cases and review of the literature. Int J Gynecol Pathol. 1995;14:283–292. doi: 10.1097/00004347-199510000-00001. [DOI] [PubMed] [Google Scholar]
- 20.Wang NP, Bacchi CE, Jiang JJ, McNutt MA, Gown AM. Does alveolar soft-part sarcoma exhibit skeletal muscle differentiation? An immunocytochemical and biochemical study of myogenic regulatory protein expression. Mod Pathol. 1996;9:496–506. [PubMed] [Google Scholar]
- 21.Radig K, Buhtz P, Roessner A. Alveolar soft part sarcoma of the uterine corpus. Report of two cases and review of the literature. Pathol Res Pract. 1998;194:59–63. doi: 10.1016/S0344-0338(98)80013-7. [DOI] [PubMed] [Google Scholar]
- 22.Zhang JK, Yan GH, Yang YB. Alveolar soft part sarcoma of the uterine cervix: a case report. J Hebei Med Coll Cont Educ (Chin) 2001;18:4–5. [Google Scholar]
- 23.Wang M, Tian YX. Alveolar soft part sarcoma of the uterine cervix: a case report. Henan J Oncol (Chin) 2002;15:91–92. [Google Scholar]
- 24.Roma AA, Yang B, Senior ME, Goldblum JR. TFE3 immunoreactivity in alveolar soft part sarcoma of the uterine cervix: case report. Int J Gynecol Pathol. 2005;24:131–135. doi: 10.1097/01.pgp.0000148343.07759.e1. [DOI] [PubMed] [Google Scholar]
- 25.Fadare O. Uncommon sarcomas of the uterine cervix: a review of selected entities. Diagn Pathol. 2006;1:30. doi: 10.1186/1746-1596-1-30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Kasashima S, Minato H, Kobayashi M, Ueda Y, Oda Y, Hashimoto S, Inoue M. Alveolar soft part sarcoma of the endometrium with expression of CD10 and hormone receptors. APMIS. 2007;115:861–865. doi: 10.1111/j.1600-0463.2007.apm_635.x. [DOI] [PubMed] [Google Scholar]
- 27.Gitau GM, Shepherd JH, Hughes G, Oriolowo A, Yiannakis D. Alveolar soft part sarcoma of the uterine cervix. Int J Gynecol Cancer. 2008;18:853–856. doi: 10.1111/j.1525-1438.2007.01073.x. [DOI] [PubMed] [Google Scholar]
- 28.Guntupalli S, Anderson ML, Bodurka DC. Alveolar soft part sarcoma of the cervix: case report and literature review. Arch Gynecol Obstet. 2009;279:263–265. doi: 10.1007/s00404-008-0700-x. [DOI] [PubMed] [Google Scholar]
- 29.Petersson F, Michal M. Minute alveolar soft part sarcoma of the endocervix: the smallest ever published case. Appl Immunohistochem Mol Morphol. 2009;17:553–556. doi: 10.1097/PAI.0b013e3181a7bc86. [DOI] [PubMed] [Google Scholar]
- 30.Mu YL, Liu M, Shi M, Zhao XB, Yin FB, Tang CS, Yelian FD. Clinical analysis of alveolar soft-tissue sarcoma of the uterine cervix: a case report. Chin Med J (Engl) 2010;123:1612–1614. [PubMed] [Google Scholar]
- 31.Argani P, Lal P, Hutchinson B, Lui MY, Reuter VE, Ladanyi M. Aberrant nuclear immunoreactivity for TFE3 in neoplasms with TFE3 gene fusions: a sensitive and specific immunohistochemical assay. Am J Surg Pathol. 2003;27:750–761. doi: 10.1097/00000478-200306000-00005. [DOI] [PubMed] [Google Scholar]