

Abstract
Purpose
The aim of this study was to determine whether biphasic calcium phosphate (BCP) bone substitute with two different concentrations of Escherichia coli-expressed recombinant human bone morphogenetic protein 2 (ErhBMP-2) enhances new bone formation in a standardized rabbit sinus model and to evaluate the concentration-dependent effect of ErhBMP-2.
Methods
Standardized, 6-mm diameter defects were made bilaterally on the maxillary sinus of 20 male New Zealand white rabbits. Following removal of the circular bony windows and reflection of the sinus membrane, BCP bone substitute without coating (control group) was applied into one defect and BCP bone substitute coated with ErhBMP-2 (experimental group) was applied into the other defect for each rabbit. The experimental group was divided into 2 subgroups according to the concentration of ErhBMP-2 (0.05 and 0.5 mg/mL). The animals were allowed to heal for either 4 or 8 weeks and sections of the augmented sinus and surrounding bone were analyzed by microcomputed tomography and histologically.
Results
Histologic analysis revealed signs of new bone formation in both the control and experimental groups with a statistically significant increase in bone formation in experimental group 1 (0.05 mg/mL ErhBMP-2 coating) after a 4-week healing period. However, no statistically significant difference was found between experimental group 1 and experimental group 2 (0.5 mg/mL ErhBMP-2 coating) in osteoinductive potential (P<0.05).
Conclusions
ErhBMP-2 administered using a BCP matrix significantly enhanced osteoinductive potential in a standardized rabbit sinus model. A concentration-dependent response was not found in the present study.
Keywords: Bone morphogenetic protein 2, Bone regeneration, Bone substitute, Maxillary sinus, Rabbits
INTRODUCTION
Recombinant human bone morphogenetic protein-2 (rhBMP-2) derived from BMP gene transfected Escherichia coli (ErhBMP-2) has been developed and considered to be a possible alternative to rhBMP-2 derived from the BMP gene transfected Chinese hamster ovary cells (CrhBMP-2) [1-4]. Recently ErhBMP-2, which showed biological activity through the post-translational refolding technique, has been reported to induce ectopic bone formation and noticeably enhanced new bone formation in a dose-dependent manner [2,5]. A supraphysiologic dose of BMP is usually applied in clinical situations to induce osteogenesis effectively [6]. However, there exist several adverse effects such as ectopic bone formation, cyst-like bone void formation, and soft tissue swelling [7-9]. Therefore, if possible, a lower dose of BMP should be applied to prevent these possible adverse effects.
Biphasic calcium phosphate (BCP) bone substitute has been widely used as a defect-filling material for periodontal and dental implant surgery and has shown favorable clinical outcomes [10]. The BCP bone substitute used in the present study is hydroxyapatite (HA) coated with β-tricalcium phosphate (β-TCP) in a 7:3 ratio that showed an ideal BCP degradation rate in previous studies [10,11]. This BCP is usually used as an osteoconductive matrix that maintains space for new bone formation. It also has osteoinductive potential which is limited but higher than than pure HA or β-TCP [11,12]. The combination of BCP as osteoconductive matrix with osteogenic cells and osteoinductive growth factors such as BMP may be even more effective in bone formation than autograft, the latter of which has, until now, been considered the gold standard of bone substitutes [13]. There exist micro- and macropores in the BCP bone substitute surface. Micropores are known to be sites of nucleation for biological apatite precipitation [14]. Macropores are potential spaces for new bone maturation, and possible sites for entrapment of BMP-2 [15].
There have been studies in which BMP-2 was applied to surgical defects in animal models. Collagen membrane, collagen block, and particulated or block type BCP bone substitute have been applied as a matrix for BMP-2 [16-18]. Collagen is the most often applied carrier. However, considering its poor structural integrity and minimal osteoconductivity, collagen cannot be an ideal matrix for BMP-2 [16,17]. BCP might be a better osteoconductive matrix for BMP-2. In addition, BCP coated with BMP-2 could be better than BCP moistened with diluted BMP-2 because of the inaccurate dosing and uncontrolled flow with the moistening method [18,19]. The purpose of this study was to evaluate the difference in bone forming ability of BCP coated with two different concentrations (0.5 mg/mL and 0.05 mg/mL) of ErhBMP-2 in rabbit sinus defects.
MATERIALS AND METHODS
Animals
Twenty male New Zealand white rabbits (40 maxillary sinus defects) weighing 2.5 to 3.0 kg were used for the experimental model (Table 1). The positioning of the window on the maxillary sinus of the rabbits followed the procedure of Asai et al. [20]: 20 mm anterior to the nasofrontal suture line and 10 mm lateral to the midline. Animal selection, management, surgical protocol, and preparation followed routines approved by the Institutional Animal Care and Use Committee of Yonsei Medical Center, Seoul, Korea.
Table 1.
Study design.

ErhBMP-2: Escherichia coli-expressed recombinant human bone morphogenetic protein 2.
Study design
Standardized, bilateral, circular, transosseous defects 6 mm in diameter were made on the maxillary sinus (Figs. 1 and 2).
Figure 1.
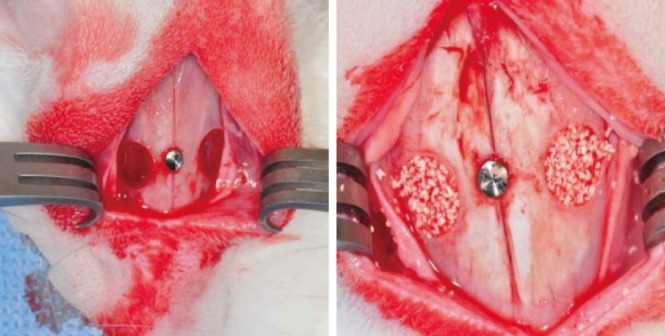
Maxillary sinus defects in the rabbit. Standardized, bilateral, circular, transosseous windows were prepared on the maxillary sinus using a 6-mm diameter trephine bur with the pin inserted.
Figure 2.

Schematic diagram of trephine bur (outer diameter 8.0 mm, inner diameter 6.0 mm, depth 1.5 mm).
Preparation of ErhBMP-2 coated BCP
Prior to the surface coating, the ErhBMP-2 was produced at the Cowell Medi Implant (Busan, Korea). Nonglycosylated rhBMP-2 was obtained in the form of inclusion bodies and was refolded in vitro into the active dimer form [11]. Surface coating was performed to combine HA, one of the constituents of BCP (Osteon, Dentium, Korea), with ErhBMP-2. Initially, the hydroxyl group of hydroxyapitite was linked with 3-aminopropyltriethoxysilane (APTES) (Sigma-Aldrich Co., St. Louis, MO, USA), a silane coupling agent, then followed by linkage with N-succinimidyl 3-maleimidopropionate (N-SMP) (Sigma-Aldrich Co.) and then ErhBMP-2. This procedure can be summarized as a three-step reaction procedure: 1) silanization with APTES, 2) cross-linking with N-SMP, 3) combining N-SMP with ErhBMP-2. Two different concentrations of ErhBMP-2 (0.5 and 0.05 mg/mL) were made after the coating procedure. ErhBMP-2-coated BCP was lyophilized. The solution was frozen cooled down to -43℃. The formulations were maintained at this temperature for 3 hours, after which they were dried in a condenser at -40℃ (primary drying) and kept in a pressure chamber at 5 mTorr for 2 hours. Secondary drying was performed on a shelf using the following sequence: -20℃ for 4 hours, -10℃ for 4 hours, 0℃ for 2 hours, and 20℃ for 20 hours. After the lyophilizing procedure, the ErhBMP-2-coated BCP was sterilized with ethylene oxide gas in a gas sterilizer (Steri-Vac 400B, 3M, St. Paul, MN, USA) at 29℃ for 5 hours, which was reported as the ideal sterilization protocol to avoid reducing osteoinductive activity [21].
Surgical procedure
For all of the surgical procedures involved in the study, the animals were first sedated with a mixture of ketamine hydrochloride (Ketalar, Yuhan, Seoul, Korea) and xylazine (Rumpun, Bayer Korea Ltd., Seoul, Korea) via an intramuscular injection. After the isolation of the surgical site by shaving and sterilizing with a povidone-iodine solution, infiltration anesthesia with 2% lidocaine (with 1:100,000 epinephrine) was also administrated to the surgical sites on the nasal bone. A straight incision along the sagittal midline on the nasal bone was then made followed by a full-thickness flap including the skin and the elevation of the periosteum laterally. Standardized, bilateral, circular, transosseous windows were prepared on the maxillary sinus using a trephine bur 6 mm in diameter under copious irrigation with saline. The pin was inserted at the point where the sagittal midline met the imaginary line that connected the right and left windows in order to indicate the reference point for micro computed tomography (CT) analysis as well as for preparation of the specimen. The trephined bony disk was carefully removed and the experimental and control treatments with grafting materials were applied to the windows accordingly.
After the grafting materials was placed, the periosteum was re-positioned over the windows on each side followed by suturing of the skin/periosteum flap with 40 Monosyn (glyconate absorbable monofilament, B-Braun, Aesculap, Center Valley, PA, USA), which was removed after 7 days. The animals were allowed a healing period of either 4 or 8 weeks postoperatively and sacrificed accordingly by euthanasia.
Radiographic analysis: Micro-CT
After obtaining block sections including the augmented sinus and the surrounding bone, each block section was fixed in 10% buffered formalin for 10 days and scanned using micro-CT (SkyScan 1076, SkyScan, Aartselaar, Belgium) at a resolution of 35 µm (100 kV and 100 µA). The scanned data set were analyzed and the area of interest was reconstructed with a CT analyzer program (SkyScan). After a 3D-reconstructed image of the maxillary sinus and supporting bone was visualized using a data viewer program, the CT volume, the maximum augmented height (MAH), and the deepest depth of the defect (DDD) [16] were measured on the coronally sectioned images; MAH was measured linearly on the cross-sectional image. The CT volume was calculated from the percentage of window closure where new bony formation or remaining grafting materials could be seen. MAH was measured linearly on the cross-sectional image whereas the DDD was measured from the imaginary line through the original bone to the bottom of the bony crater.
Histological analysis
Following decalcification in 5% formic acid for 14 days, all specimens were embedded in paraffin and sliced coronally into sections about 5 µm thick along the center of the augmented sinus. The 2 most-central sections were selected and stained with hematoxylin and eosin (H&E) for the light microscopic examination (BX50, Olympus Co., Tokyo, Japan).
Histometric analysis
Computer-assisted histometric analysis was performed using an automated image-analysis system (Image-Pro Plus, The Proven Solution, Media Cybernetics Inc., Silver Spring, MD, USA). Two parameters were measured and calculated as follows:
Newly formed bone area (NB%)=newly formed area/total augmented bone area×100
Remaining grafts area (RG%)=remaining graft area/total augmented bone area×100
Statistical analysis
The statistical analysis regarding micro-CT data and histomorphometric measurement of the samples was performed using a SPSS ver. 15.0 (SPSS Inc., Chicago, IL, USA). The Mann-Whitney U test was used to compare differences between control group and experimental group (groups 1 and 2) and differences according to time of healing. The level of statistical significance was set at P<0.05, and the data were presented as means±standard deviation values.
RESULTS
Radiographic and histometric analysis
In the 4-week healing groups, new bone formation (%) was greater in experimental group 1 than in the control group 1 (P<0.05). The remaining graft material (%) was less in experimental group 1 than in the control group 1 (P<0.05). No significant difference was found between experimental group 1 and experimental group 2 in new bone formation or remaining graft (Table 2).
Table 2.
Measurements in standardized rabbit sinus model.

Values are presented as mean±standard deviation.
CT: computed tomography, MAH: maximum augmented height, DDD: deepest depth of the defect, ErhBMP-2: Escherichia coli-expressed recombinant human bone morphogenetic protein 2.
In the 8-week healing groups, there was no statistical difference in new bone formation, remaining graft, or CT volume between experimental group 1 and experimental group 2. However, new bone formation (%) was greater in experimental group 2 than the control group 2 (P<0.05). There was no difference in the remaining graft between experimental group 1 and the control group 1. The CT volume was greater in the control group 1 than experimental group 1 (P<0.05) and the MAH was greater in experimental group 1 than in experimental group 2 (Table 2).
Histologic findings
The histologic findings revealed that both experimental group 1 and group 2 showed a mixture of newly formed bone from the surgically created defects and newly formed bone originating from bone graft materials. As shown in Figs 3-6, newly formed bone from the surgically created defect is particularly distinguishable as it is shown to be more mature in contrast to newly formed bone that originated from bone graft materials, which can be seen to be still undergoing the mineralization process.
Figure 3.

Histologic findings of experimental group 1 (0.05 mg/mL ErhBMP-2) at 4 weeks. (A) There appeared to be a mixture of newly formed bone from the surgically created defect and newly formed bone originating from bone graft materials. Newly formed bone from the surgically created defect is shown to be more mature whereas newly formed bone from the bone graft materials is still undergoing the mineralization process (×12.5). (B) Defect margin area: The arrowheads indicate the margin of the surgically created defect. The white asterisk indicates newly formed bone assumed to have originated from the defect margin (×50). (C) The Schneiderian membrane: The black asterisk indicates newly formed bone assumed to have originated from graft materials (×50). Note that immature woven bone is evident here in contrast to mature lamellar bone as indicated by the white asterisk in Fig. 3B. (D) Middle area: Immature woven bone can be seen (×50).
Figure 6.

Histologic findings of experimental group 2 (0.5 mg/mL ErhBMP-2) at 8 weeks. (A) The histologic findings were similar to those observed in experimental group 1 (0.05 mg/mL ErhBMP-2) at 8 weeks. More vascularization (arrowheads) and matured lamellar bone (black asterisk) are also evident here (×12.5). (B) Defect margin area both inflammatory cells and blood vessels can be observed, as indicated by the arrow and the arrowhead, respectively. The black asterisk indicates matured lamellar bone (×50). (C) The Schneiderian membrane (×50). (D) Middle area (×50).
In general, when compared to the 4-week healing group, more vascularization is evident in the 8-week healing group in both experimental group 1 and group 2 (Figs. 4 and 6) The Schneiderian membrane was also slightly thickened with the presence of inflammatory cells and blood vessels in the 8-week healing group. The particle size of graft materials was also dramatically reduced. Instead, mature lamellar bone was identified in between the graft materials. It was also noted that the surgically created defects were almost completely closed in the 8-week healing group.
Figure 4.

Histologic findings of experimental group 1 (0.05 mg/mL ErhBMP-2) at 8 weeks. (A) When compared to the 4 week healing group, more vascularization is evident in the 8-week healing group (arrowheads). The surgically created defect was almost completely closed. The particle size of the graft materials is dramatically reduced (white asterisk). Note that mature lamellar bone (black asterisk) is evident in the newly formed bone found in between graft materials (×12.5). (B) Defect margin area: both inflammatory cells and blood vessels can be observed, as indicated by the arrows and the arrowhead, respectively. The black asterisk indicates matured lamellar bone (×50). (C) The Schneiderian membrane: The Schneiderian membrane was also thicker than that of the 4 week healing group (×50). (D) Middle area: More mature lamellar bone is identified in newly formed bone found in between the graft materials (×50).
DISCUSSION
The effectiveness of bone substitutes and dental implants has been evaluated through various sinus models [20-23]. Asai et al. [20] introduced the rabbit sinus model to understand the mechanism of new bone formation in humans because the composition and mechanical properties of bone tissue in humans and rabbits are known to be very similar to each other [24]. Based on this study, researchers have used this rabbit sinus model to evaluate histomorphometric changes of the bone after sinus grafting, assessing the effectiveness of various bone substitute materials. The purpose of the present study was to determine whether BCP with two different concentrations of ErhBMP-2 enhances new bone formation in a standardized rabbit sinus model and to evaluate the concentration-dependent response of ErhBMP-2. In the present study, the standardized sinus model with the same shape and size of window was used, as introduced by De Souza Nunes et al. [25] to provide precisely the same conditions to the control and the experimental groups and to minimize procedural errors. The degree of anatomical variation between individuals was also smaller in the rabbit sinus model than in larger animals, thereby enabling a consistent reproduction of defects in different individuals [16], as evidenced by the present histologic findings. According to Roberts and Breznak [26], the rabbit metabolic rate is known to be three to four times faster than that of humans. Thus, the 4-week healing group and 8-week healing group were selected on the assumption that a 4-week healing period and 8-week healing period correspond to a 3 to 4 months healing period and 6 to 8 months healing period in humans, respectively. The surgical sites were exposed by an extraoral approach, which enabled good visibility and accessibility to the surgical site as well as preservation of the Schneiderian membrane through delicate drilling and careful removal of the window. Therefore, taking the aforementioned factors into account, the standardized sinus augmentation model used in this study can be considered to be a valid study model in which various bone graft materials can be evaluated.
In order to evaluate the volumetric change in new bone, 3D volumetric measurement of the augmented bone could have led to more accurate results; however, we used a two-dimensional section of the window region for the comparison of new bone formation in the control group and experimental group. To minimize the error from this procedure, linear measurements including MAH, DDD, and CT volume were performed at the two-dimensional section of the window region using micro-CT.
From histomorphometric analysis, it was found that in the 4-week healing groups, new bone formation was statistically significantly greater in experimental group 1 than control group 1. Based on this result, it can be interpreted that in experimental group 1, more graft materials were substituted with new bone. In other words, bone graft materials coated with even low concentration of ErhBMP-2 (0.05 mg/mL) showed better osteoinductive potential than bone graft materials alone. Although the difference is not statistically significant, bone graft materials coated with a high concentration of ErhBMP-2 (0.5 mg/mL) also showed better osteoinductive potential than the control group. Thus, these findings demonstrate that ErhBMP induces rapid bone formation and remodeling at an earlier stage, and this is consistent with findings of a previous study [2] that used the rat calvarial defect model. On the other hand, in the 4-week healing groups, the remaining graft was statistically significantly less in experimental group 1 than control group 1. This can be interpreted as showing that more of the bone graft material in experimental group 1 had been substituted with new bone, thereby showing less remaining graft material. Considering the fact that the amount of graft material applied to each group was the same, there might be no difference between experimental group 1 and group 2 in osteoinductive potential. This result is also supported by the results of the 8-week healing groups where MAH was statistically significantly greater in experimental group 1 than group 2, which can be interpreted as showing that the total amount of bone including new bone and graft materials increased to some extent. However, since there was no significant difference in CT volume between experimental group 1 and group 2, it is difficult to conclude that a difference in osteoinductive potential between two groups is evident.
In the 8-week healing groups, CT volume was statistically significantly greater in control group 1 than experimental group 1. However, there was not any difference between experimental group 1 and control group 1 in new bone formation and remaining graft material. This can be interpreted as showing that replacement of biomaterial with newly formed bone does not necessarily occur in a 1:1 ratio, which is in agreement with previous research [27]. In other words, the volume of bone produced in this case was greater than the volume of biomaterial absorbed. In the 8-week healing groups, the MAH in experimental group 1 was greater than experimental group 2. However, there was no significant difference in CT volume. Therefore, the greater MAH in experimental group 1 is difficult to interpret as 'more new bone formation' in experimental group 1 than group 2.
Nevertheless, as new bone formation was statistically significantly greater in experiment group 2 than control group 2, it seems that bone graft materials coated with a high concentration of ErhBMP-2 (0.5 mg/mL) show better ongoing osteoinductive potential even in that late healing period. This could lead to an assumption that, although no significant difference between the low concentration of ErhBMP-2 (0.05 mg/mL) and high concentration of ErhBMP-2 (0.5 mg/mL) in osteoinductive potential was found, the high concentration of ErhBMP-2 (0.5 mg/mL) can be more effective when long-term osteoinductive potential is needed.
In conclusion, within the limitations of this study, while BCP coated with ErhBMP-2 significantly enhanced osteoinductive potential, a concentration-dependent response to osteoinductive potential was not found.
Figure 5.

Histologic findings of experimental group 2 (0.5 mg/mL ErhBMP-2) at 4 weeks. (A) The histologic findings were similar to those observed in experimental group 1 (0.05 mg/mL ErhBMP-2) at 4 weeks. Note that surgically created defect was completely closed (×12.5). (B) Defect margin area (×50). (C) The Schneiderian membrane (×50). (D) Middle area (×50).
ACKNOWLEDGEMENTS
This research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education, Science and Technology (2010-0007829).
Footnotes
Kyung-Hee Choi who is one of co-authors works for Cowell R&D Institute as a researcher.
References
- 1.Bessho K, Konishi Y, Kaihara S, Fujimura K, Okubo Y, Iizuka T. Bone induction by Escherichia coli-derived recombinant human bone morphogenetic protein-2 compared with Chinese hamster ovary cell-derived recombinant human bone morphogenetic protein-2. Br J Oral Maxillofac Surg. 2000;38:645–649. doi: 10.1054/bjom.2000.0533. [DOI] [PubMed] [Google Scholar]
- 2.Lee JH, Kim CS, Choi KH, Jung UW, Yun JH, Choi SH, et al. The induction of bone formation in rat calvarial defects and subcutaneous tissues by recombinant human BMP-2, produced in Escherichia coli. Biomaterials. 2010;31:3512–3519. doi: 10.1016/j.biomaterials.2010.01.075. [DOI] [PubMed] [Google Scholar]
- 3.Long S, Truong L, Bennett K, Phillips A, Wong-Staal F, Ma H. Expression, purification, and renaturation of bone morphogenetic protein-2 from Escherichia coli. Protein Expr Purif. 2006;46:374–378. doi: 10.1016/j.pep.2005.09.025. [DOI] [PubMed] [Google Scholar]
- 4.Vallejo LF, Brokelmann M, Marten S, Trappe S, Cabrera-Crespo J, Hoffmann A, et al. Renaturation and purification of bone morphogenetic protein-2 produced as inclusion bodies in high-cell-density cultures of recombinant Escherichia coli. J Biotechnol. 2002;94:185–194. doi: 10.1016/s0168-1656(01)00425-4. [DOI] [PubMed] [Google Scholar]
- 5.Choi KH, Moon K, Kim SH, Yun JH, Jang KL, Cho KS. Purification and biological activity of recombinant human bone morphogenetic protein-2 produced by E. coli expression system. J Korean Acad Periodontol. 2008;38:41–50. [Google Scholar]
- 6.Walker DH, Wright NM. Bone morphogenetic proteins and spinal fusion. Neurosurg Focus. 2002;13:e3. doi: 10.3171/foc.2002.13.6.4. [DOI] [PubMed] [Google Scholar]
- 7.Wong DA, Kumar A, Jatana S, Ghiselli G, Wong K. Neurologic impairment from ectopic bone in the lumbar canal: a potential complication of off-label PLIF/TLIF use of bone morphogenetic protein-2 (BMP-2) Spine J. 2008;8:1011–1018. doi: 10.1016/j.spinee.2007.06.014. [DOI] [PubMed] [Google Scholar]
- 8.Kaneko H, Arakawa T, Mano H, Kaneda T, Ogasawara A, Nakagawa M, et al. Direct stimulation of osteoclastic bone resorption by bone morphogenetic protein (BMP)-2 and expression of BMP receptors in mature osteoclasts. Bone. 2000;27:479–486. doi: 10.1016/s8756-3282(00)00358-6. [DOI] [PubMed] [Google Scholar]
- 9.Smucker JD, Rhee JM, Singh K, Yoon ST, Heller JG. Increased swelling complications associated with off-label usage of rhBMP-2 in the anterior cervical spine. Spine (Phila Pa 1976) 2006;31:2813–2819. doi: 10.1097/01.brs.0000245863.52371.c2. [DOI] [PubMed] [Google Scholar]
- 10.Bae JH, Kim YK, Kim SG, Yun PY, Kim JS. Sinus bone graft using new alloplastic bone graft material (Osteon)-II: clinical evaluation. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;109:e14–e20. doi: 10.1016/j.tripleo.2009.10.047. [DOI] [PubMed] [Google Scholar]
- 11.Kim S, Jung UW, Lee YK, Choi SH. Effects of biphasic calcium phosphate bone substitute on circumferential bone defects around dental implants in dogs. Int J Oral Maxillofac Implants. 2011;26:265–273. [PubMed] [Google Scholar]
- 12.Zhu X, Fan H, Li D, Xiao Y, Zhang X. Protein adsorption and zeta potentials of a biphasic calcium phosphate ceramic under various conditions. J Biomed Mater Res B Appl Biomater. 2007;82:65–73. doi: 10.1002/jbm.b.30706. [DOI] [PubMed] [Google Scholar]
- 13.Truumees E, Herkowitz HN. Alternatives to autologous bone harvest in spine surgery. The University of Pennsylvania Orthopaedic Journal. 1999;12:77–88. [Google Scholar]
- 14.Le Nihouannen D, Guehennec LL, Rouillon T, Pilet P, Bilban M, Layrolle P, et al. Micro-architecture of calcium phosphate granules and fibrin glue composites for bone tissue engineering. Biomaterials. 2006;27:2716–2722. doi: 10.1016/j.biomaterials.2005.11.038. [DOI] [PubMed] [Google Scholar]
- 15.Le Nihouannen D, Saffarzadeh A, Gauthier O, Moreau F, Pilet P, Spaethe R, et al. Bone tissue formation in sheep muscles induced by a biphasic calcium phosphate ceramic and fibrin glue composite. J Mater Sci Mater Med. 2008;19:667–675. doi: 10.1007/s10856-007-3206-3. [DOI] [PubMed] [Google Scholar]
- 16.Choi Y, Yun JH, Kim CS, Choi SH, Chai JK, Jung UW. Sinus augmentation using absorbable collagen sponge loaded with Escherichia coli-expressed recombinant human bone morphogenetic protein 2 in a standardized rabbit sinus model: a radiographic and histologic analysis. Clin Oral Implants Res. 2012;23:682–689. doi: 10.1111/j.1600-0501.2011.02222.x. [DOI] [PubMed] [Google Scholar]
- 17.Jung JH, Yun JH, Um YJ, Jung UW, Kim CS, Choi SH, et al. Bone formation of Escherichia coli expressed rhBMP-2 on absorbable collagen block in rat calvarial defects. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011;111:298–305. doi: 10.1016/j.tripleo.2010.05.011. [DOI] [PubMed] [Google Scholar]
- 18.Kim JW, Choi KH, Yun JH, Jung UW, Kim CS, Choi SH, et al. Bone formation of block and particulated biphasic calcium phosphate lyophilized with Escherichia coli-derived recombinant human bone morphogenetic protein 2 in rat calvarial defects. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011;112:298–306. doi: 10.1016/j.tripleo.2010.10.025. [DOI] [PubMed] [Google Scholar]
- 19.Park JC, So SS, Jung IH, Yun JH, Choi SH, Cho KS, et al. Induction of bone formation by Escherichia coli-expressed recombinant human bone morphogenetic protein-2 using block-type macroporous biphasic calcium phosphate in orthotopic and ectopic rat models. J Periodontal Res. 2011;46:682–690. doi: 10.1111/j.1600-0765.2011.01390.x. [DOI] [PubMed] [Google Scholar]
- 20.Asai S, Shimizu Y, Ooya K. Maxillary sinus augmentation model in rabbits: effect of occluded nasal ostium on new bone formation. Clin Oral Implants Res. 2002;13:405–409. doi: 10.1034/j.1600-0501.2002.130409.x. [DOI] [PubMed] [Google Scholar]
- 21.Ijiri S, Yamamuro T, Nakamura T, Kotani S, Notoya K. Effect of sterilization on bone morphogenetic protein. J Orthop Res. 1994;12:628–636. doi: 10.1002/jor.1100120505. [DOI] [PubMed] [Google Scholar]
- 22.Bravetti P, Membre H, Marchal L, Jankowski R. Histologic changes in the sinus membrane after maxillary sinus augmentation in goats. J Oral Maxillofac Surg. 1998;56:1170–1176. doi: 10.1016/s0278-2391(98)90765-0. [DOI] [PubMed] [Google Scholar]
- 23.Scala A, Botticelli D, Rangel IG, Jr, de Oliveira JA, Okamoto R, Lang NP. Early healing after elevation of the maxillary sinus floor applying a lateral access: a histological study in monkeys. Clin Oral Implants Res. 2010;21:1320–1326. doi: 10.1111/j.1600-0501.2010.01964.x. [DOI] [PubMed] [Google Scholar]
- 24.Wang X, Mabrey JD, Agrawal CM. An interspecies comparison of bone fracture properties. Biomed Mater Eng. 1998;8:1–9. [PubMed] [Google Scholar]
- 25.De Souza Nunes LS, De Oliveira RV, Holgado LA, Nary Filho H, Ribeiro DA, Matsumoto MA. Immunoexpression of Cbfa-1/Runx2 and VEGF in sinus lift procedures using bone substitutes in rabbits. Clin Oral Implants Res. 2010;21:584–590. doi: 10.1111/j.1600-0501.2009.01858.x. [DOI] [PubMed] [Google Scholar]
- 26.Roberts EG, Breznak N. Bone Physiology and Metabolism. In: Mish CE, editor. Contemporary implant dentistry. Orlando: Mosby Year Book; 1994. pp. 557–598. [Google Scholar]
- 27.Frenken JW, Bouwman WF, Bravenboer N, Zijderveld SA, Schulten EA, ten Bruggenkate CM. The use of straumann bone ceramic in a maxillary sinus floor elevation procedure: a clinical, radiological, histological and histomorphometric evaluation with a 6-month healing period. Clin Oral Implants Res. 2010;21:201–208. doi: 10.1111/j.1600-0501.2009.01821.x. [DOI] [PubMed] [Google Scholar]