

Abstract
STUDY DESIGN
Controlled cohort repeated-measures experimental design.
OBJECTIVES
To determine if a neuromuscular training program (NMTP) focused on core stability and lower extremity strength would affect performance on the star excursion balance test (SEBT). We hypothesized that NMTP would improve SEBT performance in the experimental group and there would be no side-to-side differences in either group.
BACKGROUND
The SEBT is a functional screening tool that is used to assess dynamic stability, monitor rehabilitation progress, assess deficits following an injury, and identify athletes at high risk for lower extremity injury. The SEBT requires lower extremity coordination, balance, flexibility, and strength.
METHODS
Twenty uninjured female soccer players (13 experimental, 7 control) participated. Players trained together as a team, so group allocation was not randomized. The SEBT was administered prior to and following 8 weeks of NMTP in the experimental group and 8 weeks of no NMTP in the control group. A 3-way mixed-model ANOVA was used to determine the effect of group (experimental versus control), training (pretraining versus posttraining), and limb (right versus left).
RESULTS
After participation in a NMTP, subjects demonstrated a significant improvement in the SEBT composite score (mean ± SD) on the right limb (pretraining, 96.4% ± 11.7%; posttraining, 104.6% ± 6.1%; P = .03) and the left limb (pretraining, 96.9% ± 10.1%; posttraining, 103.4% ± 8.0%; P = .04). The control group had no change on the SEBT composite score for the right (pretraining, 95.7% ± 5.2%; posttraining, 94.4% ± 5.2%; P = .15) or the left (97.4% ± 7.2%; 93.6% ± 5.0%; P = .09) limb. Further analysis identified significant improvement for the SEBT in the posterolateral direction on both the right (P = .008) and left (P = .040) limb and the posteromedial direction of the left limb (P = .028) in the experimental group.
CONCLUSION
Female soccer players demonstrated an improved performance on the SEBT after NMTP that focused on core stability and lower extremity strength.
LEVEL OF EVIDENCE
Performance enhancement, level 2b-.
Keywords: core stability, core strengthening, injury prevention training, trunk neuromuscular control
In the United States more than 3.1 million females participate in high school sports annually.22 Soccer is ranked fifth in popularity, with over 346 000 female athletes having participated in the sport during the 2007–2008 school year.22 As the popularity of women’s soccer grows, the incidence of injury in high school sports has become more apparent. From 1995 to 1997, an estimated one quarter of female soccer athletes reported experiencing multiple injuries over a 2-year period, while over 72% sustain at least 1 injury.28
With such a high incidence of injury in female athletes, resulting in significant time lost and healthcare expense, the need to develop interventions with the potential to decrease injury risk is apparent. Several studies support the use of interventions such as neuromuscular training programs (NMTP) to reduce the incidence of lower extremity injuries.9,11,15,17,31 The most effective programs emphasize several common components, including plyometric training in combination with biomechanical feedback and technique training.9,31 Implementation of a NMTP that focuses on core stability exercises is advocated to prevent lower extremity injury, namely in female athletes who have deficits in trunk proprioception and neuromuscular control.34 Importantly, poor core stability and decreased muscular synergy of the trunk and hip stabilizers have been theorized to decrease performance in power activities and to increase the incidence of injury secondary to lack of control of the center of mass, especially in female athletes.11,33
Targeted NMTP are designed to reduce injury risk, and include interventions that focus on increased control of the center of mass. As the center of mass moves away from the base of support, there is an increased potential for biomechanical deviations to occur in the lower extremity. An improved ability to control this movement has the potential to decrease excessive forces on the lower extremity and ultimately decrease injury risk.34
The star excursion balance test (SEBT) is a functional screening tool developed to assess lower extremity dynamic stability, monitor rehabilitation progress, assess deficits following injury, and identify athletes at high risk for lower extremity injury.4,5,14,16,23,25–27 The SEBT requires neuromuscular characteristics such as lower extremity coordination, balance, flexibility, and strength.2,5,16,27 Plisky et al26,27 found that female athletes who had a composite reach distance on the SEBT of less than 94% of their limb length were 6.5 times more likely to have a lower extremity injury. As a result, the SEBT may be a useful tool to assess the efficacy of training programs designed to reduce injury risk.
The purpose of this study was to determine if an 8-week NMTP that focused on core stability and lower extremity strength could improve performance on the SEBT. We hypothesized that the neuromuscular training group would show significant improvements on the SEBT composite score that would not be seen in a control group. In addition, we hypothesized there would be no side-to-side differences in the SEBT composite score in either the experimental or the control group.
METHODS
Subjects
Twenty subjects (13 experimental, 7 control) with no prior history of lower extremity injury were recruited from 2 soccer teams to participate in this study. Data from prior work suggested that a minimum of 7 subjects in each group would be required to meet statistical power, with the alpha level set at .05 and beta at .80, assuming the mean difference would be a 10% improvement with a standard deviation of 7.5%. The subjects were allocated by team to participate in the experimental or control group. The subjects in each group were similar in terms of age, height, and body mass (TABLE 1). The subjects participated in an identical level of play and were exposed to similar soccer activity between pretraining and posttraining measurements.
TABLE 1.
Demographic Data
| Variable | Experimental Group* | Control Group* | P Value† |
|---|---|---|---|
| Age (y) | 15.4± 1.5 | 14.7± 0.8 | .26 |
| Height (cm) | 163.9 ± 5.0 | 163.6 ± 4.8 | .90 |
| Mass (kg) | 56.1 ± 6.1 | 51.5 ± 5.5 | .14 |
Values are mean ± SD.
No between-group differences.
To be included in the study, each subject had to be an active member of a soccer team at the high school or competitive level and free from injury prior to participation in the study. Subjects were excluded if they failed to complete the pretest or posttest, sustained an unrelated injury that limited their ability to complete the NMTP, or failed to participate in a minimum of 80% of the NMPT training sessions (13 of 16 sessions). Four subjects in the experimental group were excluded due to experiencing an injury unrelated to the NMTP (n = 1) or lack of training compliance (n = 3). These subjects were not retested at the 8-week follow-up. The data from 16 subjects (9 experimental, 7 controls) were used for final statistical analysis.
Procedure
Prior to testing, all subjects and their parent/guardian received and signed an informed consent approved by Cincinnati Children’s Hospital Medical Center’s Institutional Review Board, which stated how the subject’s rights would be protected. Initial testing included all demographic and anthropometric assessments of height, mass, and limb length. Subjects were interviewed to determine prior injury history. The experimental group participated in 8 weeks of biweekly neuromuscular training, while the control group did not participate in the intervention or other training outside of their normal activities. Posttraining testing occurred 8 weeks after the pretraining test session.
Star Excursion Balance Test
Each subject completed a modified SEBT modeled after the methodology described by Plisky et al27 on 2 occasions, 8 weeks apart. Subjects received verbal instruction and visual demonstration of the SEBT from the same examiner, who was not blinded to group assignment. The subjects stood on 1 lower extremity, with the most distal aspect of their great toe on the center of the grid. The subjects were then asked to reach in the anterior, posteromedial, and posterolateral direction, while maintaining their single-limb stance (FIGURE 1). Six practice trials were performed on each limb for each of the 3 reach directions prior to official testing.14 On the seventh trial, the examiner visually recorded the most distal location of the reach foot as it contacted the grid in the 3 directions. The trial was discarded and the subject repeated the testing trial if (1) the subject was unable to maintain single-limb stance, (2) the heel of the stance foot did not remain in contact with the floor, (3) weight was shifted onto the reach foot in any of the 3 directions, or (4) the reach foot did not return to the starting position prior to reaching in another direction. The process was then repeated while standing on the other lower extremity. The order of limb testing was counterbalance randomized by the tester. The subject’s limb length measurements, from the most distal end of the anterior superior iliac spine to the most distal end of the lateral malleolus on each limb, were taken and recorded. In previous work, the SEBT has demonstrated good intratester reliability, with an intraclass correlation coefficient (ICC) of 0.67 to 0.96.8,14 Intratester reliability for this study on the SEBT composite score and all 3 individual reach directions was good to excellent (TABLE 2). The SEBT composite score was calculated by dividing the sum of the maximum reach distance in the anterior (A), posteromedial (PM), and posterolateral (PL) directions by 3 times the limb length (LL) of the individual, then multiplied by 100 {[(A + PM + PL)/(LL × 3)] × 100}.
FIGURE 1.
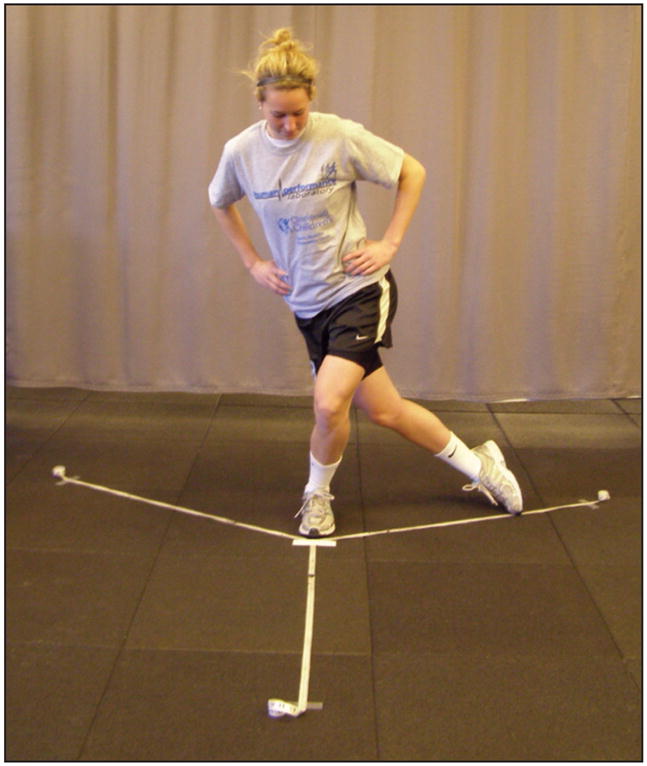
Subject performing the star excursion balance test on the left lower extremity in the posterolateral direction.
TABLE 2.
Intratester Reliability (ICC) on the Star Excursion Balance Test Composite Score and All 3 Reach Directions
| Stance Foot | Anterior | Posterolateral | Posteromedial | Composite |
|---|---|---|---|---|
| Right | 0.94 | 0.83 | 0.89 | 0.92 |
| Left | 0.96 | 0.81 | 0.90 | 0.96 |
Training Program
The NMTP was adapted from previous epidemiologic and interventional investigations that have reported reductions in lower extremity injury risk factors.17,18 The exercises in this program were selected from injury prevention research to address lower extremity strength and core stability.9,11,15,17–19,21,24 Core stability is defined as dynamic trunk control which allows for the production, transfer, and control of force and motion to distal segments of the kinetic chain.13 The goal of this NMTP was to improve the athlete’s ability to control the center of mass during dynamic activities.
The biweekly training of the experimental group was conducted by 4 physical therapists who were also certified strength and conditioning specialists, and 1 student physical therapist. The subject-therapist ratio was 4:1 for each session. The experimental group participated in biweekly training sessions for a total of 16 sessions during a competitive season. The NMTP took-place on 2 nonconsecutive days of the week over an 8-week time frame. Each session consisted of a 5-minute warm-up using an agility ladder, two 45-minute increments of lower extremity strength and core stability training, and a 5-minute cool-down that included static and dynamic stretches. The core stability component was divided into 5 phases of progressive exercises (TABLE 3). Two or 3 days were spent on each phase. The lower extremity strengthening program consisted of 2 groups of exercises which were performed on alternating training sessions (TABLE 4). These exercises were progressed using periodization techniques. This NMTP did not include exercises that emulated the SEBT.
TABLE 3.
Five Phases of the Core Stability Portion of Neuromuscular Training Program
| Reference | Phase 1 | Phase 2 | Phase 3 | Phase 4 | Phase 5 |
|---|---|---|---|---|---|
| Hewett 1999,10 Mandelbaum 200515 | Lateral jump and hold | Lateral jumps | Lateral hop and hold | Lateral hops | X-hops |
| Hewett 199910 | Step-hold | Jump single-leg hold | Hop-hold | Hop-hop-hold | Crossover-hop-hop-hold |
| Myer 200719 | BOSU (round) toe touch swimmers* | BOSU (round) swimmers with partner perturbations* | Prone bridge (elbows and knees) hip extension opposite shoulder flexion* | Prone bridge (elbows and toes) hip extension* | Prone bridge (elbows and toes) hip extension opposite shoulder flexion* |
| Myer 200719 | BOSU (round) double-knee hold | BOSU (round) single-knee hold | Swiss ball bilateral kneel (FIGURE 4) | Swiss ball bilateral kneel with partner pertubations | Swiss ball bilateral kneel with lateral ball catch |
| Myklebust 2003,21 Petersen 200524 | Single-leg lateral Airex hop-hold | Single-leg lateral BOSU (round) hop-hold | Single-leg lateral BOSU (round) hop-hold with ball catch | Single leg 4-way BOSU (round) hop-hold | Single-leg 4-way BOSU (round) hop-hold with ball catch |
| Hewett 199910 | Single-tuck jump soft landing | Double-tuck jump | Repeated-tuck jump | Side-to-side barrier tuck jumps | Side-to-side reaction barrier tuck jumps |
| Mandelbaum 200515 | Front lunges | Walking lunges | Walking lunges unilaterally weighted | Walking lunges with plate crossover | Walking lunges with unilateral shoulder press |
| Hewett 199910 | Lunge jumps* | Scissor jumps* | Lunge jumps unilaterally weighted* | Scissor jumps unilaterally weighted* | Scissor jumps with ball swivel* |
| Mandelbaum 200515 | BOSU (flat) double-leg pelvic bridges* | BOSU (flat) single-leg pelvic bridges* | BOSU (round) single-leg pelvic bridges with weight* | Supine Swiss ball hamstring curl* | Russian hamstring curl with lateral touch* |
| Myklebust 2003,21 Peterson 200524 | Single-leg 90° hop-hold | Single-leg 90° Airex hop-hold (FIGURE 3) | Single-leg 90° Airex hop-hold reaction ball catch | Single-leg 180° Airex hop-hold | Single-leg 180° Airex hop-hold reaction ball catch |
| Myer 200719 | BOSU (round) lateral crunch | Box lateral crunch | BOSU (round) lateral crunch with ball catch | Swiss ball lateral crunch | Swiss ball lateral crunch with ball catch |
| Myklebust 2003,21 Peterson 200524 | Box double-crunch | Box swivel double-crunch | BOSU (round) swivel ball touches (feet up) | BOSU (round) double-crunch | BOSU (round) swivel double-crunch |
| Myer 200719 | Swiss ball back hyperextension* | Swiss ball back hyperextension with ball reach* | Swiss ball hyperextensions with back fly* | Swiss ball hyperextensions with ball reach lateral* | Swiss ball hyperextensions with lateral ball catch* |
Online video available and www.jospt.org.
TABLE 4.
Example of Lower Extremity Strength Training Component of the Neuromuscular Training Program
| Strength training, day 1 | Strength training, day 2 |
The NMTP was designed to gradually progress lower extremity strength and core stability by incorporating exercises that increase lateral trunk perturbations. The exercise progressions were developed from previous biomechanical investigations that reported reductions in knee abduction load in female athletes.17–20 Initially, a low volume was used for the high-intensity exercises until correct technique was attained. When the athlete could perform the exercise with proper mechanics as determined by the instructor, the volume was increased. The instructors gave verbal and visual feedback with each exercise to the subjects. Athletes executed each exercise using only proper technique and were required to stop if they could not perform the exercise with correct biomechanics. The exercises were progressed from stable surfaces to dynamic surfaces such as Airex pads (Perform Better Inc, Cranston, RI), BOSU trainers (BOSU Balance Trainer [Fitness Quest Inc], Canton, OH), and Swiss balls (Perform Better Inc), to increase demands on lower extremity strength and core stability. The subjects were required to maintain proper technique, while external perturbations (ball toss, unanticipated movement to the base of support) were applied to increase difficulty of the task.
Statistical Analysis
Unpaired t tests were used to assess for differences in demographic and anthropometric data between groups. The SEBT scores were used as the dependant variables. Group comparisons were done with a 2-by-2-by-2 mixed-model analysis of variance (ANOVA) to determine the effect of training (pretraining versus post-training), group (experimental versus control), and limb (right versus left) on the outcome of the SEBT composite and individual directions scores. Statistical analyses were conducted in SPSS, Version 15.0 (SPSS Inc, Chicago, IL). Statistical significance was established a priori at P≤.05.
RESULTS
Comparison of the demographic data between the experimental and control group showed no significant difference in age, height, or mass (P>.05) (TABLE 1). Pretraining SEBT composite scores showed no significant side-to-side difference within subjects or between groups (experimental versus control) (P>.05).
There was a significant training-by-group interaction (F = 5.71, P = .024), with no effect of limb (F =0.51, P = .479) for the SEBT composite score. Subjects in the experimental group improved performance of the SEBT composite score on both limbs after 8 weeks of training, while no change was observed in the control group. Partial η2 effect size was determined to be 0.169. Partial η2 effect size statistics demonstrate the proportion of variance of the dependant variable explained by the independent variable. Values can range from 0 to 1, with small (0.01), medium (0.06), or large (0.138) effect size. The results indicate that there is a large effect size according to this classification.1 The improvement seen on the SEBT occurred despite the NMTP not replicating the SEBT. The SEBT composite score improved from a mean ± SD of 96.4% ± 11.7% to 104.6 % ± 6.1% of limb length on the right lower extremity (P = .03) and from 96.9% ± 10.1% to 103.4% ± 8.0% of limb length on the left lower extremity (P = .04), following the NMTP. Conversely, there was no significant change in the SEBT composite score of either the right (95.7% ± 5.2% to 94.4% ± 5.2%; P = .15) or the left (97.4% ± 7.2% to 93.6% ± 5.0%; P = .09) limb in the control group (FIGURE 2).
FIGURE 2.

The experimental group demonstrated a significantly higher star excursion balance test composite score on both limbs following the neuromuscular training program (P≤.05). Error bars are ±1 SD.
Analysis of change in each individual reach direction revealed a significant interaction for group (experimental versus control) by training (pretraining versus posttraining) for both the right (P = .008) and left (P = .040) limb in the posterolateral direction, and the left limb (P = .028) in the posteromedial direction, for the subjects in the experimental group. No differences were seen for the right limb (P = .226) in the posteromedial direction and for neither the right (P = .321) nor left (P = .193) limb in the anterior direction for the experimental group. A summary of data is presented in TABLE 5.
TABLE 5.
Distance on the Star Excursion Balance Test for Each Direction
| Direction/Limb/Group | Pretraining* | Posttraining* | P Value | Partial η2† |
|---|---|---|---|---|
| Anterior | ||||
| Right | .321 | 0.070 | ||
| NMTP | 68.2 ± 11.0 | 71.7 ± 5.8 | ||
| CTRL | 62.9 ± 4.4 | 61.7 ± 4.4 | ||
| Left | .193 | 0.118 | ||
| NMTP | 70.4 ± 6.6 | 70.4 ± 6.1 | ||
| CTRL | 63.7 ± 6.8 | 59.7 ± 6.5 | ||
| Posteromedial | ||||
| Right | .226 | 0.103 | ||
| NMTP | 101.4 ± 16.4 | 107.4 ± 9.6 | ||
| CTRL | 96.9 ± 8.3 | 95.0 ± 8.8 | ||
| Left | .028‡ | 0.299 | ||
| NMTP | 98.1 ± 15.6 | 105.6± 12.9 | ||
| CTRL | 102.2 ± 11.7 | 97.1 ± 9.2 | ||
| Posterolateral | ||||
| Right | .008‡ | 0.405 | ||
| NMTP | 87.6 ± 13.6 | 99.2 ± 10.0 | ||
| CTRL | 94.1 ± 10.2 | 93.7 ± 7.9 | ||
| Left | .040‡ | 0.269 | ||
| NMTP | 89.8 ± 13.0 | 99.2 ± 7.3 | ||
| CTRL | 92.4 ± 7.5 | 91.4 ± 4.9 | ||
Abbreviations: CTRL, control group; NMTP, neuromuscular training group.
Data presented as mean ± SD cm.
Effect size (>0.138, large effect).
Significant group-by-time interaction, with follow-up indicating a significant pretraining to post-training difference for the NMTP group (P<.05).
DISCUSSION
Prior to training, both the experimental and the control groups of female athletes demonstrated similar performance on the SEBT in all measured variables. Following a NMTP, the SEBT composite score significantly improved in the training group compared to the control group, who did not participate in a NMTP. Improvement in the SEBT composite score in the NMTP group appeared to be dependent on an improvement in the posterolateral and posteromedial reach, as indicated by the independent reach analysis. No differences in reach were found in the anterior direction. Improvements in the posterolateral and posteromedial direction are likely the result of improved neuromuscular control and dynamic balance, and less related to lower extremity strength, as was suggested by Thorpe and Ebersole.32
The NMTP design was based on injury prevention research.9,10,11,15,17–19,21,24,32 Each aspect of the NMTP was enhanced with verbal feedback and visual demonstration to improve the athletes biomechanical technique.9,31 Current literature supports the use of NMTP that incorporate core stability as part of treatment programs to prevent injury of the ankle or knee.16,34 Decreased neuromuscular control of the trunk appears to influence dynamic stability of the lower extremity during high-speed athletic maneuvers.34
In a systematic review by Thacker et al,31 6 prospective studies that addressed training programs that all proved to have reduced knee injuries were chosen. The 6 programs consisted of neuromuscular, proprioception, and/or acceleration training. Of the 6 studies, 4 were randomized controlled studies, but none reported blinding of the assessor or the details of the randomization of the subjects. The training programs demonstrated positive results, with significantly reduced knee injury rates compared to controls who did not participate in a training program.31 Other studies have also confirmed improved postural control and balance following rehabilitation and training programs in individuals with chronic ankle instability.5,16 The individuals in the NMTP in the current study showed improvements in the SEBT composite scores when compared to nontrained controls. However, its effect on knee or ankle injury rate was not assessed in this study. The SEBT may have the potential to be a corollary outcome measure that can be utilized to compare the efficacy of programs that reduce injury rates.27
Prior research indicates that isolated strength measures may not have an effect on the SEBT score. Thorpe and Ebersole32 compared recreational and collegiate female soccer student athletes and found no difference in isokinetic strength. They also showed that there was a low to moderate correlation between SEBT performances and lower extremity strength. Therefore, other factors, such as muscle activation and proprioception, may have a stronger relative relationship to the SEBT performance than non–weight-bearing strength testing. In addition, neither group of the above study participated in a NMTP that might have contributed to the lack of change on the SEBT.
Robinson and Gribble29 suggested that improvements in the SEBT were not due to strength or core stability but, rather, to increased knee and hip flexion on the stance limb. Their study consisted of 20 participants from a university setting who did not undergo any intervention program. Stepwise regression revealed that hip flexion and knee flexion, separately and in combination, accounted for 62% to 95% of the variance in reach distances.29 It is important to consider that Robinson and Gribble29 did not measure lower extremity strength. It is possible that participants who showed increased knee and hip flexion potentially had more lower extremity strength compared to the subjects who had less knee and hip flexion angles.
Sato and Mokha30 looked at the effects of a core strength training program on ground reaction forces, stability of the lower extremity using the SEBT, and overall running performance in recreational and competitive runners. They did not find any improvements in SEBT after implementing a 6-week core strength training program. However, there are several differences that existed between this study and the current one. These included a lack of balance training and biomechanical feedback, a different definition of core stability training, and a different testing protocol for the SEBT.
Specific thresholds have been developed to screen for injury risk using the SEBT. Plisky et al26,27 found that female athletes with less than 94% composite reach during the SEBT were upwards of 6 times more likely to experience an injury. Although the mean SEBT composite score for both groups was initially above the 94% threshold for injury risk, the NMTP focused on lower extremity strength and core stability training did improve the SEBT composite score. Individually, in the trained group, 7/18 of the limbs scored below the 94% threshold at pretraining. Posttraining, only 2/18 limbs were below 94% threshold. The 2 subjects who remained below the threshold posttraining were below 94% pretraining. Based on Myer et al,19 the results are expected to be magnified in athletes who would fall below the injury risk threshold. This infers that participation in a NMTP that focuses on lower extremity strength and core stability may reduce the risk of injury. If a NMTP could improve SEBT measures, then athletes could be evaluated for SEBT composite reach before competition and be preventatively placed in a NMTP targeted toward deficits in lower extremity strength and core stability.
The SEBT may be a sufficiently sensitive tool for trained athletes that can be used prior to competition to assess neuromuscular factors more comprehensively than strength alone.32 The SEBT has also been examined to determine the correlation between anterior cruciate ligament injury with the lack of postural control and was found to successfully demonstrate limitations in individuals who were anterior cruciate ligament deficient compared with asymptomatic individuals. Individuals who were anterior cruciate ligament deficient had significantly lower reach scores on both the involved and uninvolved extremity compared to uninjured controls.6
Following the NMTP, there was no difference in composite score between limbs in the control group or in the experimental group. This may be due to the design of the NMTP, which focused on the performance of exercises equally on each limb and likely contributed to the lack of a limb effect. Establishing limb symmetry was important because limb dominance and side-to-side imbalance in lower extremity measures have been found to be a risk factor for anterior cruciate ligament injury.3,9
The SEBT has successfully been used to demonstrate asymmetrical impairments in functional balance on the involved side in individuals with chronic ankle instability or anterior cruciate ligament deficiency compared to uninjured controls.4,6,7,23 Training and rehabilitation programs have also been reported to reduce the side-to-side asymmetry in functional balance.5,6,16
Limitations
Study limitations should be taken into consideration. Four subjects were excluded from the experimental group, resulting in a 31% drop-out rate. Although it was a higher drop-out rate, the power analysis confirmed that the sample size was sufficient. Another limitation is the small number of adolescent female soccer players, which decreases the applicability to other populations. Finally, training was performed without the benefits of random assignment and without the blinding of the investigators.
Further investigation is necessary to determine if a NMTP that improves the SEBT composite score would reduce in-season injury rates. A randomized controlled trial with longitudinal injury tracking is needed to assess cause and effect to determine if the NMTP does indeed have an effect on in-season injury rates. A longitudinal study is necessary to determine if the NMTP has lasting effects on the subject’s strength and core stability.
Other implications for future research include utilizing the SEBT for assessment and screening tools for athletes. The SEBT is an easy and practical tool that may be used as a preseason screening tool to determine which athletes may be more at risk for a lower extremity injury. It may also be important to combine the SEBT with other screening tools to better determine which athletes may be in greater jeopardy of injury.
CONCLUSION
Neuromuscular training that focused on lower extremity strength and core stability significantly improved the composite SEBT scores in female soccer players. The SEBT composite score was enhanced to 103% following participation in the NMTP.
FIGURE 3.
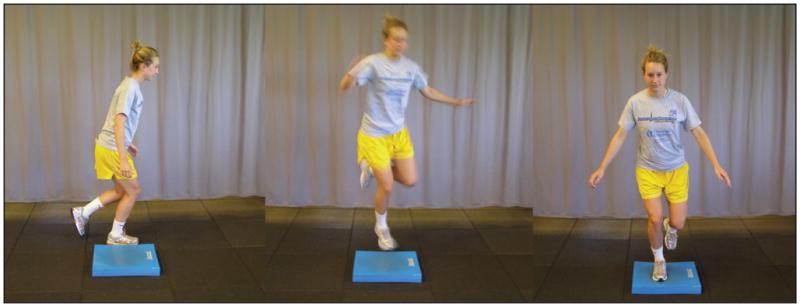
Single-limb 90° Airex hop and hold (phase 2 in exercise progression).
FIGURE 4.
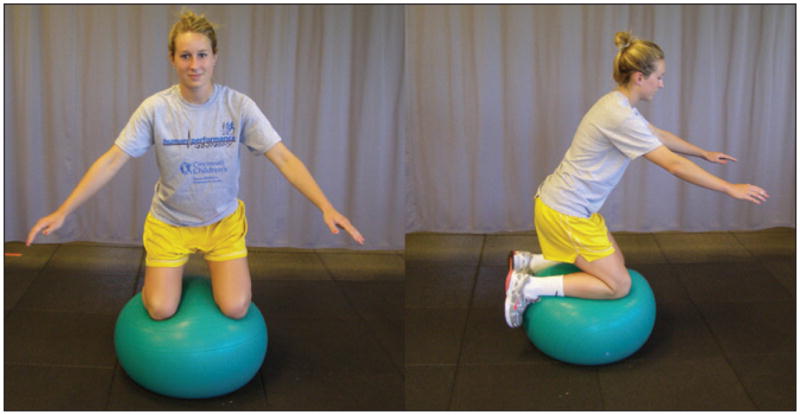
Swiss ball bilateral kneel (phase 3 in exercise progression).
KEY POINTS.
FINDINGS
An 8-week duration neuromuscular training program that focused on lower extremity strength and core stability improved performance on the SEBT in female soccer players.
IMPLICATION
Further investigation is needed to determine if neuromuscular training that improves performance on the SEBT also decreases in-season injury rates in female athletes.
CAUTION
Training was performed in a small group within a narrow age range, without the benefits of random assignment and blinding of the investigators.
Acknowledgments
The authors would like to acknowledge funding support from National Institutes of Health/NIAMS Grants R01-AR049735, R01-AR05563 and R01-AR056259. The Cincinnati Children’s Hospital Medical Center Institutional Review Board approved the protocol for this study.
The authors would like to acknowledge the following people who assisted in the training for this study: Jensen Brent, CSCS, Chad Cherny, PT, DPT, MS, CSCS, Chris Kovacs, PT, DPT, CSCS, and Rachel Martin, PT, DPT. The authors would like to also acknowledge funding support from National Institutes of Health/NIAMS Grants R01-AR049735, R01-AR05563, and R01-AR056259
References
- 1.Cohen J. Statistical Power Analysis for the Behavioural Sciences. 2. Hillsdale, NJ: Lawrence Erlbaum Associates, Inc; 1988. [Google Scholar]
- 2.Earl JE, Hertel J. Lower-extremity muscle activation during the star excursion balance tests. J Sport Rehabil. 2001;10:93–104. [Google Scholar]
- 3.Ford KR, Myer GD, Hewett TE. Valgus knee motion during landing in high school female and male basketball players. Med Sci Sports Exerc. 2003;35:1745–1750. doi: 10.1249/01.MSS.0000089346.85744.D9. [DOI] [PubMed] [Google Scholar]
- 4.Gribble PA, Hertel J, Denegar CR, Buckley WE. The effects of fatigue and chronic ankle instability on dynamic postural control. J Athl Train. 2004;39:321–329. [PMC free article] [PubMed] [Google Scholar]
- 5.Hale SA, Hertel J, Olmsted-Kramer LC. The effect of a 4-week comprehensive rehabilitation program on postural control and lower extremity function in individuals with chronic ankle instability. J Orthop Sports Phys Ther. 2007;37:303–311. doi: 10.2519/jospt.2007.2322. http://dx.doi.org/10.2519/jospt.2007.2322. [DOI] [PubMed] [Google Scholar]
- 6.Herrington L, Hatcher J, Hatcher A, McNicholas M. A comparison of Star Excursion Balance Test reach distances between ACL-deficient patients and asymptomatic controls. Knee. 2009;16:149–152. doi: 10.1016/j.knee.2008.10.004. http://dx.doi.org/10.1016/j.knee.2008.10.004. [DOI] [PubMed] [Google Scholar]
- 7.Hertel J, Braham RA, Hale SA, Olmsted-Kramer LC. Simplifying the star excursion balance test: analyses of subjects with and without chronic ankle instability. J Orthop Sports Phys Ther. 2006;36:131–137. doi: 10.2519/jospt.2006.36.3.131. http://dx.doi.org/10.2519/jospt.2006.2103. [DOI] [PubMed] [Google Scholar]
- 8.Hertel J, Miller SJ, Denegar CR. Intratester and intertester reliability during the star excursion balance tests. J Sport Rehabil. 2000;9:104–116. [Google Scholar]
- 9.Hewett TE, Ford KR, Myer GD. Anterior cruciate ligament injuries in female athletes: part 2, a meta-analysis of neuromuscular interventions aimed at injury prevention. Am J Sports Med. 2006;34:490–498. doi: 10.1177/0363546505282619. http://dx.doi.org/10.1177/0363546505282619. [DOI] [PubMed] [Google Scholar]
- 10.Hewett TE, Lindefeld TN, Riccobene JV, Noyes FR. The effect of neuromuscular training on the incidence of knee injury in female athletes. A prospective study. Am J Sports Med. 1999;27(6):699–706. doi: 10.1177/03635465990270060301. [DOI] [PubMed] [Google Scholar]
- 11.Hewett TE, Myer GD, Ford KR. Reducing knee and anterior cruciate ligament injuries among female athletes: a systematic review of neuromuscular training interventions. J Knee Surg. 2005;18:82–88. doi: 10.1055/s-0030-1248163. [DOI] [PubMed] [Google Scholar]
- 12.Ireland ML, Willson JD, Ballantyne BT, Davis IM. Hip strength in females with and without patellofemoral pain. J Orthop Sports Phys Ther. 2003;33:671–676. doi: 10.2519/jospt.2003.33.11.671. [DOI] [PubMed] [Google Scholar]
- 13.Kibler WB, Press J, Sciascia A. The role of core stability in athletic function. Sports Med. 2006;36:189–198. doi: 10.2165/00007256-200636030-00001. [DOI] [PubMed] [Google Scholar]
- 14.Kinzey SJ, Armstrong CW. The reliability of the star-excursion test in assessing dynamic balance. J Orthop Sports Phys Ther. 1998;27:356–360. doi: 10.2519/jospt.1998.27.5.356. [DOI] [PubMed] [Google Scholar]
- 15.Mandelbaum BR, Silvers HJ, Watanabe DS, et al. Effectiveness of a neuromuscular and proprioceptive training program in preventing anterior cruciate ligament injuries in female athletes: 2-year follow-up. Am J Sports Med. 2005;33:1003–1010. doi: 10.1177/0363546504272261. http://dx.doi.org/10.1177/0363546504272261. [DOI] [PubMed] [Google Scholar]
- 16.McKeon PO, Ingersoll CD, Kerrigan DC, Saliba E, Bennett BC, Hertel J. Balance training improves function and postural control in those with chronic ankle instability. Med Sci Sports Exerc. 2008;40:1810–1819. doi: 10.1249/MSS.0b013e31817e0f92. http://dx.doi.org/10.1249/MSS.0b013e31817e0f92. [DOI] [PubMed] [Google Scholar]
- 17.Myer GD, Brent JL, Ford KR, Hewett TE. A pilot study to determine the effect of trunk and hip focused neuromuscular training on hip and knee isokinetic strength. Br J Sports Med. 2008;42:614–619. doi: 10.1136/bjsm.2007.046086. http://dx.doi.org/10.1136/bjsm.2007.046086. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Myer GD, Chu DA, Brent JL, Hewett TE. Trunk and hip control neuromuscular training for the prevention of knee joint injury. Clin Sports Med. 2008;27:425–448. ix. doi: 10.1016/j.csm.2008.02.006. http://dx.doi.org/10.1016/j.csm.2008.02.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Myer GD, Ford KR, Brent JL, Hewett TE. Differential neuromuscular training effects on ACL injury risk factors in “high-risk” versus “low-risk” athletes. BMC Musculoskelet Disord. 2007;8:39. doi: 10.1186/1471-2474-8-39. http://dx.doi.org/10.1186/1471-2474-8-39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Myer GD, Ford KR, Palumbo JP, Hewett TE. Neuromuscular training improves performance and lower-extremity biomechanics in female athletes. J Strength Cond Res. 2005;19:51–60. doi: 10.1519/13643.1. http://dx.doi.org/10.1519/13643.1. [DOI] [PubMed] [Google Scholar]
- 21.Myklebust G, Engebretsen L, Braekken IH, Skjolberg A, Olsen OE, Bahr R. Prevention of anterior cruciate ligament injuries in female team handball players: a prospective intervention study over three seasons. Clin J Sport Med. 2003;13:71–78. doi: 10.1097/00042752-200303000-00002. [DOI] [PubMed] [Google Scholar]
- 22.NFHS Associations. [Accessed May 17, 2010];National Federation of State High School Associations Participation Survey. 2007–2008 Available at: www.nfhs.org.
- 23.Olmsted LC, Carcia CR, Hertel J, Shultz SJ. Efficacy of the star excursion balance tests in detecting reach deficits in subjects with chronic ankle instability. J Athl Train. 2002;37:501–506. [PMC free article] [PubMed] [Google Scholar]
- 24.Petersen W, Braun C, Bock W, et al. A controlled prospective case control study of a prevention training program in female team handball players: the German experience. Arch Orthop Trauma Surg. 2005;125:614–621. doi: 10.1007/s00402-005-0793-7. http://dx.doi.org/10.1007/s00402-005-0793-7. [DOI] [PubMed] [Google Scholar]
- 25.Plisky PJ, Gorman PP, Butler RJ, Kiesel KB, Underwood FB, Elkins B. The reliability of an instrumented device for measuring components of the star excursion balance test. NAJSPT. 2009;4:92–99. [PMC free article] [PubMed] [Google Scholar]
- 26.Plisky PJ, Gorman PP, Kiesel KB, Butler RJ, Rauh MJ. Comparison of performance on the star excursion balance test by sport, competition level, and gender [abstract] J Orthop Sports Phys Ther. 2009;39:A111. [Google Scholar]
- 27.Plisky PJ, Rauh MJ, Kaminski TW, Underwood FB. Star Excursion Balance Test as a predictor of lower extremity injury in high school basketball players. J Orthop Sports Phys Ther. 2006;36:911–919. doi: 10.2519/jospt.2006.2244. http://dx.doi.org/10.2519/jospt.2006.2244. [DOI] [PubMed] [Google Scholar]
- 28.Rauh MJ, Macera CA, Ji M, Wiksten DL. Subsequent injury patterns in girls’ high school sports. J Athl Train. 2007;42:486–494. [PMC free article] [PubMed] [Google Scholar]
- 29.Robinson R, Gribble P. Kinematic predictors of performance on the Star Excursion Balance Test. J Sport Rehabil. 2008;17:347–357. doi: 10.1123/jsr.17.4.347. [DOI] [PubMed] [Google Scholar]
- 30.Sato K, Mokha M. Does core strength training influence running kinetics, lower-extremity stability, and 5000-M performance in runners? J Strength Cond Res. 2009;23:133–140. doi: 10.1519/JSC.0b013e31818eb0c5. http://dx.doi.org/10.1519/JSC.0b013e31818eb0c5. [DOI] [PubMed] [Google Scholar]
- 31.Thacker SB, Stroup DF, Branche CM, Gilchrist J, Goodman RA, Porter Kelling E. Prevention of knee injuries in sports. A systematic review of the literature. J Sports Med Phys Fitness. 2003;43:165–179. [PubMed] [Google Scholar]
- 32.Thorpe JL, Ebersole KT. Unilateral balance performance in female collegiate soccer athletes. J Strength Cond Res. 2008;22:1429–1433. doi: 10.1519/JSC.0b013e31818202db. http://dx.doi.org/10.1519/JSC.0b013e31818202db. [DOI] [PubMed] [Google Scholar]
- 33.Zatsiorsky VM. Science and Practice of Strength Training. Champaign, IL: Human Kinetics Publishers; 1995. [Google Scholar]
- 34.Zazulak BT, Hewett TE, Reeves NP, Goldberg B, Cholewicki J. Deficits in neuromuscular control of the trunk predict knee injury risk: a prospective biomechanical-epidemiologic study. Am J Sports Med. 2007;35:1123–1130. doi: 10.1177/0363546507301585. http://dx.doi.org/10.1177/0363546507301585. [DOI] [PubMed] [Google Scholar]