

Abstract
Background:
Suicide is a preventable cause of death, inspite of which its incidence is increasing worldwide. Very few studies are done to know the perception of suicide attempters regarding prevention of their suicide attempt. Such information may be helpful in implementing preventive strategies. This study was done to find out whether those who attempted suicide and recovered perceived that their suicide attempt could have been prevented or not.
Materials and Methods:
Fifty consecutive subjects were recruited by purposive sampling method. These subjects were admitted for suicide attempt and were stable after medical management. Subjects were assessed using socio-demographic and clinical proforma, Pierce suicide intent scale and structured questionnaire to assess their perception regarding suicide. Group differences for categorical variables were examined with the chi-square test, whereas an independent ‘t’ test was used for continuous variables.
Results:
Analysis revealed that 80% of suicide attempters felt that their suicide attempt could have been prevented. 64% of the study subjects perceived that family members and near and dear ones could have helped in preventing their attempt while 16% of the study subjects perceived that society could have helped.
Conclusions:
Majority of subjects on recovery from the suicide attempt perceived that their suicide attempt could have been prevented by family members, near and dear ones and society.
Keywords: Suicide, suicide prevention, suicidal attempt, perception regarding suicide
INTRODUCTION
Suicide the most preventable cause of death is among the top 20 leading causes of mortality globally for all ages. In the last 50 years suicide rates have increased by 60% worldwide while in India there is 43% increase in suicide rate in last three decades. Currently suicide rate in India is about 10.3/100,000 general population.[1]
Every individual differs in aetiology of their suicide or suicide attempts due to diverse social and personal circumstances and biological predispositions.[2] Variations in suicide risk factors in different cultures and periods are known.[3,4] Common psychosocial causes of attempted suicide in Southeast Asia includes problems in interpersonal relationships, family conflicts, domestic violence, academic failure, disappointment in love, recent bereavement and other stressful life events.[5–12] Research reveals that 98% of those who committed suicide had suffered from some diagnosable mental disorder especially adjustment disorder, depression, substance use disorders and physical illness.[13–17]
Irrespective of aetiology of suicide or suicide attempt various methods of intervention have been proposed for prevention of suicide at different levels.[18–22] There have been several recent reviews on interventions that are considered effective in reducing suicide rates.[13,23–27] Most interventions for prevention of suicide emphasise the active role of health care provider. Suicide experts have identified the preventive interventions like providing education and awareness programs for the general public and professionals, screening methods for identifying at high-risk individuals, treatment of psychiatric disorders, restricting media reports on suicide and access to lethal means.
This study is attempts out to find out as to whether suicide attempters perceive that their attempt could have been prevented from occurring and the role of family members and society in preventing suicide attempt as perceived by the suicide attempters. This may have implication in developing strategies for future research in this area and strategies for prevention of suicide and suicide attempts.
Study objectives
To assess as to whether the subject after the index suicide attempt perceives that their suicide attempt could have been prevented.
To assess the role of family members, near and dear ones and society in the prevention of suicide attempt as perceived by the subject.
MATERIALS AND METHODS
Participants
This was a cross-sectional, hospital-based study conducted from September 2010 to march 2011 at Department of Psychiatry JSS Hospital Mysore, Karnataka (India). This hospital has a policy of routine psychosocial intervention for all patients with suicide attempt on referral basis. Fifty consecutive subjects (both male and female) who had recovered from their suicide attempt were recruited by purposive sampling method after obtaining informed consent. Exclusion criteria were presence of psychotic symptoms, inability to provide information about their suicidal behavior, severe physical illness or terminal physical illness as per treating physician. The information of each patient was collected from the patient him/herself, key relative accompanying the patient, case record file, and treating consultant.
Measures
1- Sociodemographic and clinical proforma- This consist of age, gender, marital status, occupation, socio-economic status, residence, years of education, religion, medical diagnosis, psychiatric diagnosis, family history of suicide, Interval between admission and assessment, method used, etc.
2- Pierce suicide intent scale[28] –This scale consists of 12 items to assess severity of the suicide intent. First six items are scored based on circumstances, 7-10 items are scored based on report from the subject, and 11, 12 items are about medical risk. Total of 0-3 score indicate low intent, 4-10 medium intent and a score of more than 10 indicate high intent.
3- Structured questionnaire to assess suicide attempters’ perception regarding their suicide attempt- this questionnaire was developed for the purpose of this study by two psychiatrists. Questions assessed his/ her perception regarding their suicide attempt. Questions assessed that did he/ she perceived that their suicide attempt could have been prevented and who could have helped in preventing their suicide attempt.
Descriptive statistics were used to describe various sample characteristics. Group differences for categorical variables were examined with χ2 test and independent ‘t’ test was used for continuous variables.
RESULTS
General demographic characteristics
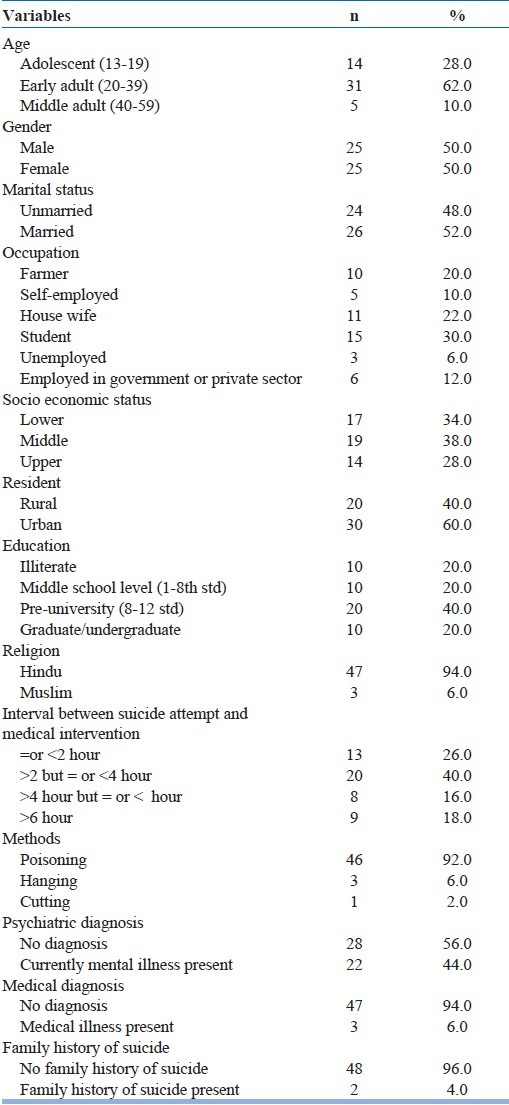
Aged between 20 and 39 (62%), student (30%), middle socioeconomic status (38%), urban back ground (60%), educated up to 8-12 std (40%), hindu (94%), brought for treatment within 2-4 hours after suicide attempt (40%), used poisoning as the method of suicide attempt (92%), without psychiatric diagnosis (56%), without medical illness (94%) and without family history of suicide (96%) [Table 1].
Table 1.
General demographic characteristics
Population characteristics
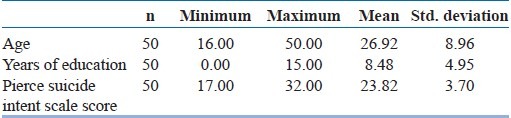
Mean age of the study sample was 26.9 years, mean years of education of the study sample was 8.4 years and mean score of the study sample on Pierce suicide intent scale score was 23.8 [Table 2].
Table 2.
Population characteristics
Perception regarding suicide prevention
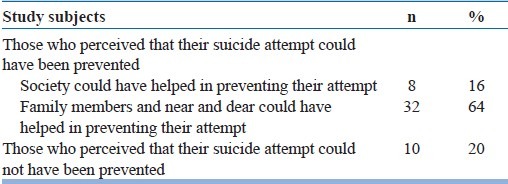
80% of the subjects in the study perceived that their suicide attempt could have been prevented. 64% of the study subjects perceived that family members and near and dear one's could have helped in preventing their attempt while 16% of the study subjects perceived that society could have helped. 20% of the study subjects perceived that their suicide attempt could not have been prevented [Table 3].
Table 3.
Perception regarding suicide prevention
Demographic characteristics of the subjects who perceived that their suicide attempt could not have been prevented with those who perceived that their suicide attempt could have been prevented [Table 4].
Table 4.
Demographic characteristics of the subjects who perceived that their suicide attempt could not have been prevented with those who perceived that their suicide attempt could have been prevented
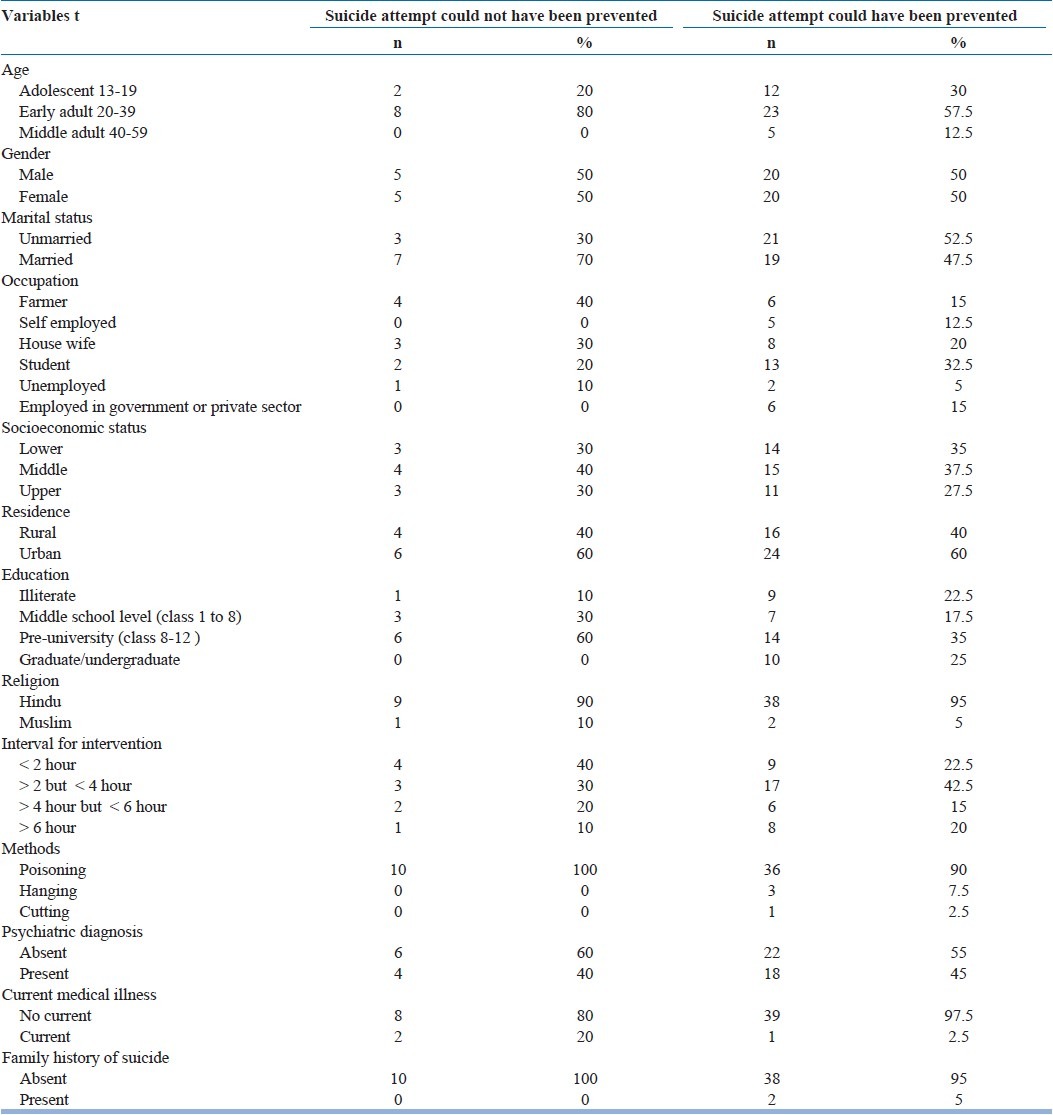
Perception that their suicide attempt could not have been prevented was perceived more by those aged 20-39 years, married, farmer by occupation. Perception that their suicide attempt could have been prevented was more by those aged 13-19 years, unmarried, students, had 8-12 years of education. No significant difference was noted between the two groups.
There was no significant correlation between perception regarding suicide prevention and Pierce suicide intent scale score.
DISCUSSION
Most of the demographic characteristics of the sample are similar to those in previous Indian studies except for some differences.[29–32] About one third of all attempters were students, 80% were literate and both males and females were equal in number.[7,31,33,34] Over the years reports of suicide attempt among students are increasing and academic related factors (e.g. failure) have been attributed to this increase.[34–38] The earlier study found higher suicide incidence among those with lower education levels but as literacy rate is increasing a change in trend has been observed.[34,36,38] Education may perpetuate the risk by increasing the dilemma of purpose of life. No gender differences were observed in our study although male suicidal attempts have been increasing in south India which may be due to changes in lifestyle trends.[39–41] 44% of the subjects in the study sample received psychiatric diagnosis and among them, majority was found to have depressive symptoms or syndromal depression. Studies have found depression to be most frequently associated with suicide attempts.[30,31,34]
Most of the suicide attempters in our study perceived that their attempt could have been prevented either by family members, near and dear ones or by society. In the Indian context, family is an important support system and determines the mental health of an individual.[30,38] Studies have shown that factors associated at interpersonal, familial and social levels like bereavement, break in steady relationship or love failure, unemployment, recent major financial crisis, family problem, fall in social reputation, marital disharmony, dowry problem, poor social and psychological support, fearful familial attachment, sense of familial noncohesiveness as risk factors for suicide attempt.[30,31,42–45] Our study results are consistent with the above research findings as all of them point towards family and society, to be playing a significant role in suicide. Also the above findings are supported by intervention studies targeting these factors such as home-based family treatment (Multisystem therapy),[46] attachment-based family therapy (ABFT)[47] and cognitive behavior therapy[48] which have shown to be helpful in reducing the rate of attempted suicide.
Suicide attempt could have been prevented was perceived that more by the unmarried than by the married. Due to the social changes the quality of emotional relationship is deteriorating and tolerance level is diminishing among Indian couples and they often take extreme step “very quickly”. Forced or unwanted marriage, social disapproval of divorce, the traditional stigmatization of widows are often found to be associated with suicide.[49] Also single status may be associated with less adjustment, social, financial and familial issues which are often the cause of suicidal attempt among married in India.[50]
However, before considering our study findings, one should also consider that this perception may also be a reflection of a different mental state than the actual state before or during the attempt.
Limitations of the study are it's a small sample sized hospital based cross-sectional study, risk factors influencing suicide attempt was not assessed, no diagnostic tools were used to assess psychiatric co-morbidities.
CONCLUSIONS
Majority of the subjects on recovery from a suicide attempt irrespective of the severity of suicide intent, perceived that their suicidal attempt could have been prevented and emphasized that family members and near and dear ones could have helped in preventing their suicide attempt. Thus, it may be beneficial to involve family and society to a greater extent in an effort to reduce the incidence of suicide by providing better education and awareness programs.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Vijayakumar L. Indian research on suicide. Indian J Psychiatry. 2010;52:291–6. doi: 10.4103/0019-5545.69255. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Prasad J, Abraham VJ, Minz S, Abraham S, Joseph A, Muliyil JP, et al. Rates and factors associated with suicide in Kaniyambadi block, Tamil Nadu, South India, 2000-2002. Int J Soc Psychiatry. 2006;52:65–71. doi: 10.1177/0020764006061253. [DOI] [PubMed] [Google Scholar]
- 3.Bhatia T, Thomas P, Semwal P, Thelma BK, Nimgaonkar VL, Deshpande SN. Differing correlates for suicide attempts among patients with schizophrenia or schizoaffective disorder in India and USA. Schizophr Res. 2006;86:208–14. doi: 10.1016/j.schres.2006.04.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Phillips M. Suicide prevention in developing countries: Where should we start? World Psychiatry. 2004;3:156–7. [PMC free article] [PubMed] [Google Scholar]
- 5.Kumar PN. Suicide in Kerala- from a Mental Health Perspective. Indian Med Assoc News Bull (Kozhikode Branch) 2000;6:3–4. [Google Scholar]
- 6.Bannerjee G, Nandi DN, Nandi S, Sarkar S, Boral GC, Ghosh A. The vulnerability of Indian women to suicide. Indian J Psychiatry. 1990;32:305–8. [PMC free article] [PubMed] [Google Scholar]
- 7.Rao VA. Attempted suicide. Indian J Psychiatry. 1965;7:253–64. [Google Scholar]
- 8.Sathyavathi K. Attempted suicide in psychiatric patients. Indian J Psychiatry. 1971;13:37–42. [Google Scholar]
- 9.Khan MM, Reza H. Attempted suicide in Karachi, Pakistan. Suicide Life Threat Behav. 1998;28:54–60. [PubMed] [Google Scholar]
- 10.Marecek J. Culture, gender and suicidal behaviour in Sri Lanka. Suicide Life Threat Behav. 1998;28:69–81. [PubMed] [Google Scholar]
- 11.Badrinarayana A. Suicide attempt in Gulberga. Indian J Psychiatry. 1977;19:69–70. [Google Scholar]
- 12.Khan FA, Anand B, Devi MG, Murthy KK. Psychological autopsy of suicide- A cross sectional study. Indian J Psychiatry. 2005;47:73–8. doi: 10.4103/0019-5545.55935. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Bertolote JM, Fleischmann A. Suicidal behavior prevention: WHO perspectives on research. Am J Med Genet C Semin Med Genet. 2005;133:8–12. doi: 10.1002/ajmg.c.30041. [DOI] [PubMed] [Google Scholar]
- 14.Subramanyan N, Kumar PN, Kunhikoyamu AM. Psycho-socio-demographic correlates of intent and lethality in attempted suicide. Thesis submitted University of Calicut in partial fulfilment of the rules and regulations for the MD Degree examinations in Psychiatry. 2011 [Google Scholar]
- 15.Kumar PN. Suicide in Perspective-With special Reference to Kerala. News Lett Indian Med Assoc (Kozhikode Branch) 2001;5:3–5. [Google Scholar]
- 16.Chia BH. Physical illness and suicide. Singapur Med J. 1984;25:30–3. [PubMed] [Google Scholar]
- 17.Hude Q, Julio A, Gordon HF, Heather LS, Edgar JL. Association between physical illness and suicide among the elderly. Soc Psychiatry Psychiatr Epidemiol. 2002;37:190–7. doi: 10.1007/s001270200014. [DOI] [PubMed] [Google Scholar]
- 18.Gordon RS. An operational classification of disease prevention. Public Health Rep. 1983;98:107–9. [PMC free article] [PubMed] [Google Scholar]
- 19.Mrazek PJ, Haggerty RJ. Reducing risks for mental disorder: Frontiers for preventive intervention research. Washington, DC: National Academy Press; 1994. [PubMed] [Google Scholar]
- 20.Brown GK, Have T, Henriques GR, Xie SX, Hollander JE, Beck AT. Cognitive therapy for the prevention of suicide attempts: A randomized controlled trial. JAMA. 2005;294:563–70. doi: 10.1001/jama.294.5.563. [DOI] [PubMed] [Google Scholar]
- 21.Kleinman M, William EB. In: Reducing Suicide: A National Imperative. Sara KG, Terry CP, editors. Washington, D.C: Joseph Henry Press (National Academies Press); 2002. p. 496. [PubMed] [Google Scholar]
- 22.Nordentoft M. Prevention of suicide and attempted suicide in Denmark. Epidemiological studies of suicide and intervention studies in selected risk groups. Dan Med Bull. 2007;54:306–69. [PubMed] [Google Scholar]
- 23.Goldney RD. Suicide prevention: A pragmatic review of recent studies. Crisis. 2005;26:128–40. doi: 10.1027/0227-5910.26.3.128. [DOI] [PubMed] [Google Scholar]
- 24.Beautrais AL. National strategies for the reduction and prevention of suicide. Crisis. 2005;26:1–3. doi: 10.1027/0227-5910.26.1.1. [DOI] [PubMed] [Google Scholar]
- 25.Mann JJ, Apter A, Bertolote J, Beautrais A, Currier D, Haas A, et al. Suicide prevention strategies: A systematic review. JAMA. 2005;294:2064–74. doi: 10.1001/jama.294.16.2064. [DOI] [PubMed] [Google Scholar]
- 26.Hawton K. A national target for reducing suicide. Br Med J. 1998;317:156–7. doi: 10.1136/bmj.317.7152.156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Hepp U, Schnyder U. Can suicidality be cured.? Suicide prevention in the G.P's practice. Praxis (Bern 1994) 2004;93:1817–23. doi: 10.1024/0369-8394.93.44.1817. [DOI] [PubMed] [Google Scholar]
- 28.Pierce DW. Suicidal intent in self injury. Br J Psychiatry. 1977;130:377–85. doi: 10.1192/bjp.130.4.377. [DOI] [PubMed] [Google Scholar]
- 29.Joseph A, Abraham S, Muliyil JP, George K, Prasad J, Minz S, et al. Evaluation of suicide rates in rural India using verbal autopsies, 1994-99. BMJ. 2003;326:1121–2. doi: 10.1136/bmj.326.7399.1121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Kar N. Profile of risk factors associated with suicide attempts: A study from Orissa, India. Indian J Psychiatry. 2010;52:48–56. doi: 10.4103/0019-5545.58895. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Nagendra Gouda M, Rao SM. Factors related to attempted suicide in Davanagere. Indian J Community Med. 2008;33:15–8. doi: 10.4103/0970-0218.39237. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Baby S, Haridas, Manju, Yesudas KF. Psychiatric diagnosis in attempted suicide. Calicut Med J. 2006;4:e2. [Google Scholar]
- 33.Lal N, Sethi BB. Demographic and socio demographic variables in attempted suicide by poisoning. Indian J Psychiatry. 1975;17:100–7. [Google Scholar]
- 34.Narang RL, Mishra BP, Mohan N. Attempted suicide in Ludhiana. Indian J Psychiatry. 2000;42:83–7. [PMC free article] [PubMed] [Google Scholar]
- 35.Rao V, Chennian R. Attempted suicide and suicide in students in Madurai. Indian J Psychiatry. 1972;14:389–96. [Google Scholar]
- 36.Sudhir Kumar CT, Chandrasekaran R. A study of psychosocial and clinical factors associated with adolescent suicide attempts. Indian J Psychiatry. 2000;42:237–42. [PMC free article] [PubMed] [Google Scholar]
- 37.Gupta SC, Singh H. Psychiatric illness in suicide attempters. Indian J Psychiatry. 1981;23:69–74. [PMC free article] [PubMed] [Google Scholar]
- 38.Manoranjitham SD, Rajkumar AP, Thangadurai P, Prasad J, Jayakaran R, Jacob KS. Risk factors for suicide in rural south India. Br J Psychiatry. 2010;196:26–30. doi: 10.1192/bjp.bp.108.063347. [DOI] [PubMed] [Google Scholar]
- 39.Sudhir Kumar CT, Mohan R, Ranjith G, Chandrasekaran R. Gender differences in medically serious suicide attempts: A study from south India. Psychiatry Res. 2006;144:79–86. doi: 10.1016/j.psychres.2005.11.012. [DOI] [PubMed] [Google Scholar]
- 40.Soman CR, Safraj S, Kutty VR, Vijayakumar K, Ajayan K. Suicide in South India: A community-based study in Kerala. Indian J Psychiatry. 2009;51:261–4. doi: 10.4103/0019-5545.58290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Mayer P, Ziaian T. Suicide, gender, and age variations in India. Are women in indian society protected from suicide? Crisis. 2002;23:98–103. doi: 10.1027//0227-5910.23.3.98. [DOI] [PubMed] [Google Scholar]
- 42.Lessard JC, Moretti MM. Suicidal ideation in an adolescent clinical sample: Attachment patterns and clinical implications. J Adolesc. 1998;21:383–95. doi: 10.1006/jado.1998.0169. [DOI] [PubMed] [Google Scholar]
- 43.Kohler BJ, Stott FM. Separation, interdependence and social relations. In: Bloom-Feschbach J, Bloom-Feschbach S, editors. The psychology of separation and loss. San Francisco: Jossey Bass Inc; 1987. pp. 187–9. [Google Scholar]
- 44.Wagner BM, Silverman MA, Martin CE. Family factors in youth suicidal behaviors. Am Behav Sci. 2003;46:1171–91. [Google Scholar]
- 45.Chioqueta AP, Stiles TC. The relationship between psychological buffers, hopelessness, and suicidal ideation: Identification of protective factors. Crisis. 2007;28:67–73. doi: 10.1027/0227-5910.28.2.67. [DOI] [PubMed] [Google Scholar]
- 46.Huey SJ, Jr, Henggeler SW, Rowland MD, Halliday-Boykins CA, Cunningham PB, Pickrel SG, et al. Multisystemic therapy effects on attempted suicide by youths presenting psychiatric emergencies. J Am Acad Child Adolesc Psychiatry. 2004;43:183–90. doi: 10.1097/00004583-200402000-00014. [DOI] [PubMed] [Google Scholar]
- 47.Diamond GS, Wintersteen MB, Brown GK, Diamond GM, Gallop R, Shelef K, et al. Attachment-based family therapy for adolescents with suicidal ideation: a randomized controlled trial. J Am Acad Child Adolesc Psychiatry. 2010;49:122–31. doi: 10.1097/00004583-201002000-00006. [DOI] [PubMed] [Google Scholar]
- 48.Stanley B, Brown G, Brent DA, Wells K, Poling K, Curry J, et al. Cognitive-behavioral therapy for suicide prevention (CBT-SP): treatment model, feasibility, and acceptability. J Am Acad Child Adolesc Psychiatry. 2009;48:1005–13. doi: 10.1097/CHI.0b013e3181b5dbfe. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Mayer P, Ziaian T. Indian suicide and marriage: A research note. J Comp Fam Stud. 2002;33:297–396. [Google Scholar]
- 50.Mohanty S, Sahu G, Mohanty MK, Patnaik M. Suicide in India: A four year retrospective study. J Forensic Leg Med. 2007;14:185–9. doi: 10.1016/j.jcfm.2006.05.007. [DOI] [PubMed] [Google Scholar]