

Abstract
The outcome of four cases of sterile endophthalmitis that developed after intravitreal injections of bevacizumab has been reported here. All four eyes received 1.25 mg/0.05 ml intravitreal bevacizumab from 0.2-ml aliquots for different etiologies. The inflammation predominantly involved the anterior chamber with mild vitreous reaction. All patients were culture negative and regained preinjection visual acuity and were culture negative following intravitreal antibiotic administration. This report highlights that intravitreal bevacizumab can cause sterile endophthalmitis and this has to be kept in mind, and clinical judgment should be used to differentiate it from infective endophthalmitis.
Keywords: Antivascular endothelial growth factor, intravitreal bevacizumab, ocular inflammation
Bevacizumab (Avastin; Basel, Switzerland) is a recombinant humanized monoclonal antibody that is directed against all isoforms of the vascular endothelial growth factor (VEGF). It is approved for intravenous administration for the treatment of metastatic colon cancer. In ophthalmology, bevacizumab has been used widely as an off-label treatment for ocular disorders like age-related macular degeneration (wet variety),[1] retinal vein occlusion, proliferative diabetic retinopathy,[2] diabetic macular edema, and retinopathy of prematurity.
Intravitreal bevacizumab (IVBe) can cause complications, including traumatic cataract, retinal detachment, and endophthalmitis, with the reported incidence of endophthalmitis ranging from 0.014% to 0.082%.[3,4] Recently, there have been a few reports of toxic anterior segment syndrome (TASS)-like culture-negative sterile endophthalmitis after IVBe injection for diverse etiologies.[5–7] We report similar cases occurring in four patients at our center. According to our knowledge, this is the first of its kind report from our country.
In our center, we routinely inject over 100 IVBe injections every month.[8] During the last 3 months we have encountered four such cases of ocular inflammation within 3-5 days of administering 1.25 mg/0.05 ml IVBe injection. The purpose of this report is to emphasize the role of intravitreal antibiotics alone in patients with suspected post-IVBe endophthalmitis. This is important because recent reports in the literature seem to suggest that these patients need vitrectomy.[5]
Routinely, bevacizumab was obtained from the manufacturer and was prepared by the authors’ hospital pharmacy by a qualified pharmacist under sterile conditions. From the commercially available 4-ml vial containing 100 mg bevacizumab (Avastin Genentech, Inc., San Francisco, CA, USA) ,0.2-ml fractions were transferred under strict aseptic conditions (class 10 environment) into 2-ml glass ampoules which subsequently were flame sealed. During the entire formulation process, cold chain (2-8°C) was maintained.[9]
Bevacizumab (1.25 mg/0.05 ml) was injected into the vitreous cavity in a surgical room maintaining standard aseptic precautions. After the injection, all patients received topical antibiotic treatment with gatifloxacin and were instructed for routine examination the next day as per the protocol followed in our hospital. On day 1 after IVBe none of the patients had any evidence of ocular inflammation.
All the four cases presented 3-5 days after IVBe with a drop in visual acuity, and mild ciliary injection with severe anterior chamber reaction accompanied by mild vitreitis (grade 1 haze).
Case Report
A 65-year-old man with recurrent choroidal neovascular membrane who had previously received IVBe injection twice [Fig. 1a] presented to us 3 days after injection with a vision hand movements associated with severe anterior chamber inflammation with mild vitreitis [Fig. 1b]. Before injection, his visual acuity was 5/200. The same day we performed vitreous tap with simultaneous intravitreal ceftazidime (2.25 mg/0.1 ml) and vancomycin (1 mg/0.1 ml) injections and started 0.5% moxifloxacin (Vigamox; Alcon Laboratories Inc.) prednisolone acetate 1% solution and homatropine 2% for cycloplegia. Gram stain and culture results were negative. One week later, he regained preinjection visual acuity and 4 weeks later, his visual acuity improved to 20/200 [Fig. 1c].
Figure 1.

(a) Fundus photograph showing the recurrent choroidal neovascular membrane with an activity at the edge in the form of retinal hemorrhage. (b) Fundus photograph 3 days after intravitreal bevacizumab injection showing vitreous haze obscuring fundus details. (c) Fundus photograph 4 weeks after the intravitreal injection showing clearing of the vitreous cavity with scarring of the neovascular membrane
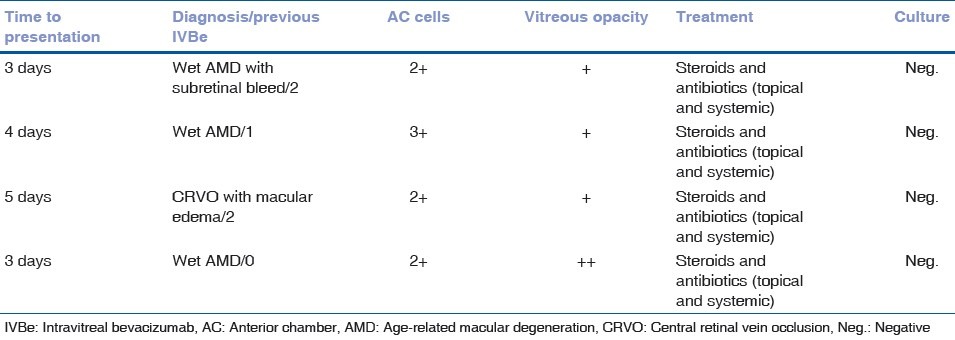
All the other three patients were managed similarly. The clinical charts of these four patients were reviewed and the details are shown in Table 1. Three of the four patients had received previous IVBe, but none had developed intraocular inflammation before.
Table 1.
Clinical findings of sterile endophthalmitis after intravitreal injection of bevacizumab
Discussion
There are two views regarding the cause of sterile endophthalmitis that have been described by some of the authors. The first view is that it is caused by some endotoxin or breakdown product due to the faulty storage of bevacizumab. The second view is that it may be an immune-mediated response to bevacizumab, following repeated injections.[7]
The reports published documenting this type of ocular inflammation after IVBe have traced the drug to the same lot of vials of bevacizumab.[5,6]
In our series of patients who developed severe intraocular inflammation after an IVBe injection, the cause remains to be determined. We believe that the cause seems to be sterile endophthalmitis similar to what is widely known to develop following intravitreal triamcinolone in some cases. Infective etiology was less likely as the culture was negative in all the cases and the reaction was more concentrated in the anterior chamber with only mild vitreitis in the form of grade 1-2 haze. Also all the four cases regained the preinjection visual acuity after intravitreal antibiotics and topical treatment.
In our center, multiple 4-ml vials of bevacizumab are usually dispensed at a time into 0.2-ml aliquoted glass ampoules containing 5 mg of the drug.[9] So it was not possible for us to attribute the causative glass ampoule to the same lot of bevacizumab. But clustering of these four cases within a short span of time can point to the same lot.
Till date the causes of this type of sterile endophthalmitis occurring soon after IVBe remain unsolved. As discussed previously, it may be either of the two causes. Regarding management options also, there are differing views. Whereas Sato et al, have performed vitrectomy in all their cases of sterile endophthalmitis,[5] Yamashiro et al, have done vitrectomy in the most severely affected eyes and managed conservatively the less severely affected eyes with topical and systemic medications.[6] It is difficult to differentiate sterile from infectious endophthalmitis, especially in the cases with severe anterior inflammation and hypopyon. There lies the importance of vitreous tap and culture for ruling out infective etiology.
We believe that the administration of intravitreal antibiotics along with topical antibiotics and steroids may be appropriate in dealing with this TASS-like picture following IVBe injection. With the rising graph of IVBe injections, the number of such cases is sure to rise, thus necessitating the need to find a prudent approach to deal with such situations.
References
- 1.Avery RL, Pieramici DJ, Rabena MD, Castellarin AA, Nasir MA, Giust MJ. Intravitreal bevacizumab (Avastin) for neovascular age-related macular degeneration. Ophthalmology. 2006;113:363–72. doi: 10.1016/j.ophtha.2005.11.019. [DOI] [PubMed] [Google Scholar]
- 2.Avery RL, Pearlman J, Pieramici DJ, Rabena MD, Castellarin AA, Nasir MA, et al. Intravitreal bevacizumab (Avastin) in the treatment of proliferative diabetic retinopathy. Ophthalmology. 2006;113:1695–705. doi: 10.1016/j.ophtha.2006.05.064. [DOI] [PubMed] [Google Scholar]
- 3.Shima C, Sakaguchi H, Gomi F, Kamei M, Ikuno Y, Oshima Y, et al. Complications in patients after intravitreal injection of bevacizumab. Acta Ophthalmol. 2008;86:372–6. doi: 10.1111/j.1600-0420.2007.01067.x. [DOI] [PubMed] [Google Scholar]
- 4.Jonas JB, Spandau UH, Rensch F, Von Baltz S, Schlichtenbrede F. Infectious and noninfectious endophthalmitis after intravitreal bevacizumab. J Ocul Pharmacol Ther. 2007;23:240–2. doi: 10.1089/jop.2006.0146. [DOI] [PubMed] [Google Scholar]
- 5.Sato T, Emi K, Ikeda T, Bando H, Sato S, Morita S, et al. Severe Intraocular Inflammation after intravitreal Injection of Bevacizumab. Ophthalmology. 2010;117:512–6. doi: 10.1016/j.ophtha.2009.07.041. [DOI] [PubMed] [Google Scholar]
- 6.Yamashiro K, Tsujikawa A, Miyamoto K, Oh H, Otani A, Tamuara H, et al. Sterile endophthalmitis after intravitreal injection of bevacizumab obtained from a single batch. Retina. 2010;30:485–90. doi: 10.1097/IAE.0b013e3181bd2d51. [DOI] [PubMed] [Google Scholar]
- 7.Wickremasinghe SS, Michalova K, Gilhotra J, Guymer RH, Harper CA, Wong TY, et al. Acute intraocular inflammation after intravitreous injections of bevacizumab for treatment of neovascular age related macular degeneration. Ophthalmology. 2008;115:1911–5. doi: 10.1016/j.ophtha.2008.05.007. [DOI] [PubMed] [Google Scholar]
- 8.Mandal S, Garg S, Venkatesh P, Mithal C, Vohra R, Mehrotra A. Intravitreal bevacizumab for subfoveal idiopathic choroidal neovascularization. Arch Ophthalmol. 2007;125:1487–92. doi: 10.1001/archopht.125.11.1487. [DOI] [PubMed] [Google Scholar]
- 9.Velpandian T, Sharma C, Garg SP, Mandal S, Ghose S. Safety and cost-effectiveness of single dose dispensing of bevacizumab for various retinal pathologies in developing countries. Indian J Ophthalmol. 2007;55:488–90. doi: 10.4103/0301-4738.36502. [DOI] [PMC free article] [PubMed] [Google Scholar]