

A 42-year-old woman with an 8-year history of unexplained macrocytosis (MCV 114) and mild thrombocytopaenia (105) presented with dry cough and dyspnea. She was noted to have fine inspiratory crepitations on auscultation of the chest and gray eyebrows and hair roots (Figure 1). The patient admitted to coloring her hair since she went completely gray at the age of 17. A thin section computed tomography scan of the chest demonstrated subpleural and basal predominant reticular changes and early honeycombing (Figure 2, arrowheads), and open lung biopsy confirmed usual interstitial pneumonia (Figure 3, hematoxylin and eosin, ×20) with fibroblastic foci (arrow, inset ×100) and early honeycomb change. Her peripheral blood mononuclear cell telomere length was well below the 1st percentile for her age, and Sanger sequencing confirmed a novel mutation resulting in a change from alanine to aspartic acid at position 678 in the TERT gene (Figure 4). There was no family history of lung disease; however, details were limited because the patient was adopted. Telomerase deficiency leads to progressive shortening of telomere length and premature cellular senescence, and is a recently identified cause of familial and sporadic pulmonary fibrosis, with which premature graying and hematologic abnormalities are often associated (1–4).
Figure 1.

Figure 2.
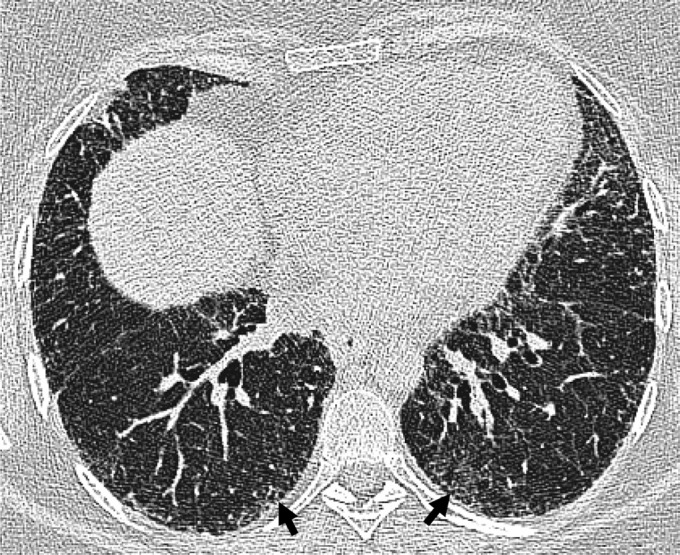
Figure 3.
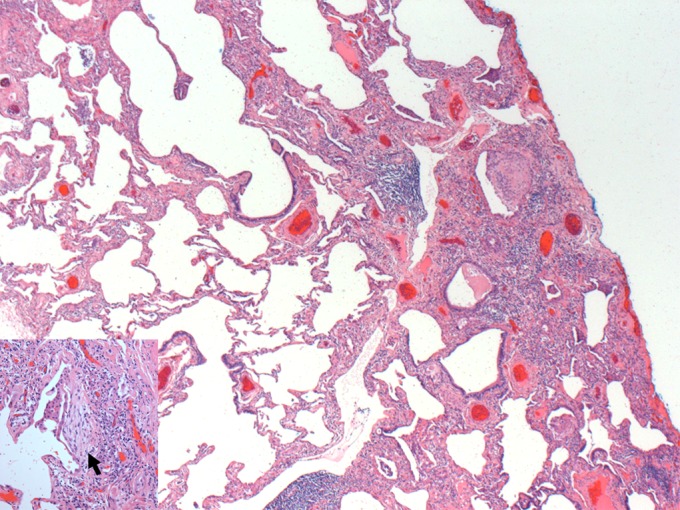
Figure 4.

Supplementary Material
Footnotes
Supported by funding from the National Institutes of Health (R01 HL093096) (to C.K.G.) and the Doris Duke Charitable Foundation (to C.K.G.).
Author Contributions: Conception and design, D.C.C., B.E.C., J.M., C.K.G.; drafting the manuscript for important intellectual content, D.C.C., B.E.C., J.M., C.K.G.
Author disclosures are available with the text of this article at www.atsjournals.org.
References
- 1.Diaz de Leon A, Cronkhite JT, Katzenstein AL, Godwin JD, Raghu G, Glazer CS, Rosenblatt RL, Girod CE, Garrity ER, Xing C, et al. Telomere lengths, pulmonary fibrosis and telomerase (TERT) mutations. PLoS ONE 2010;5:e10680. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Diaz de Leon A, Cronkhite JT, Yilmaz C, Brewington C, Wang R, Xing C, Hsia CC, Garcia CK. Subclinical lung disease, macrocytosis, and premature graying in kindreds with telomerase (TERT) mutations. Chest 2011;140:753–763 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Tsakiri KD, Cronkhite JT, Kuan PJ, Xing C, Raghu G, Weissler JC, Rosenblatt RL, Shay JW, Garcia CK. Adult-onset pulmonary fibrosis caused by mutations in telomerase. Proc Natl Acad Sci USA 2007;104:7552–7557 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Armanios MY, Chen JJ, Cogan JD, Alder JK, Ingersoll RG, Markin C, Lawson WE, Xie M, Vulto I, Phillips JA, 3rd, et al. Telomerase mutations in families with idiopathic pulmonary fibrosis. N Engl J Med 2007;356:1317–1326 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.