

Abstract
Context:
Cuboid syndrome is thought to be a common source of lateral midfoot pain in athletes.
Evidence Acquisition:
A Medline search was performed via PubMed (through June 2010) using the search terms cuboid, syndrome, subluxed, locked, fault, dropped, peroneal, lateral, plantar, and neuritis with the Boolean term AND in all possible combinations. Retrieved articles were hand searched for additional relevant references.
Results:
Cuboid syndrome is thought to arise from subtle disruption of the arthrokinematics or structural congruity of the calcaneocuboid joint, although the precise pathomechanic mechanism has not been elucidated. Fibroadipose synovial folds (or labra) within the calcaneocuboid joint may play a role in the cause of cuboid syndrome, but this is highly speculative. The symptoms of cuboid syndrome resemble those of a ligament sprain. Currently, there are no definitive diagnostic tests for this condition. Case reports suggest that cuboid syndrome often responds favorably to manipulation and/or external support.
Conclusions:
Evidence-based guidelines regarding cuboid syndrome are lacking. Consequently, the diagnosis of cuboid syndrome is often based on a constellation of signs and symptoms and a high index of suspicion. Unless contraindicated, manipulation of the cuboid should be considered as an initial treatment.
Keywords: cuboid, syndrome, subluxed, midfoot
Cuboid syndrome is an easily misdiagnosed source of lateral midfoot pain, and is believed to arise from a subtle disruption of the arthrokinematics or structural congruity of the calcaneocuboid (CC) joint.1,2,36,45 This condition is associated with several clinical terms for lateral midfoot pathology, including cuboid fault syndrome, dropped cuboid, subluxed cuboid, locked cuboid, peroneal cuboid syndrome, and lateral plantar neuritis.30,32,36,45 This presumed alteration in congruence and/or arthrokinematics can develop insidiously31 or after a traumatic event (eg, ankle sprain),2,10,31,36,43 and may be difficult to identify clinically or with imaging.2,10,31,36
Anatomy and Mechanics
The cuboid is located in the lateral midfoot, surrounded by the calcaneus posteriorly, the fourth and fifth metatarsals anteriorly, and the navicular and lateral cuneiform medially (Figures 1 and 2). CC joint function is dependent on midtarsal joint mechanics, since the navicular and cuboid bones move essentially in tandem during gait.16 The mechanics of the CC joint are highly variable.35 The principal movement at the CC joint is medial/lateral rotation about an anterior/posterior axis with the calcaneal process acting as a pivot.3,15 The rotation has been described as pronation/supination and obvolution/involution.3,15 Inversion/eversion is used herein.
Figure 1.
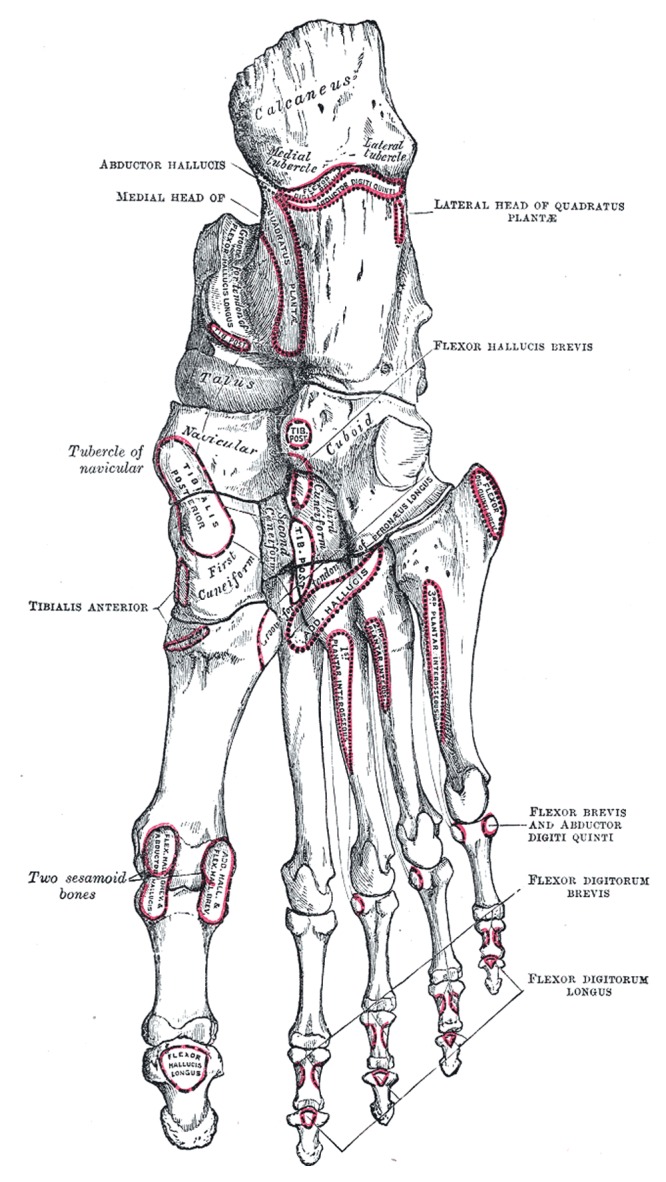
Right foot plantar view. (From Gray’s Anatomy. Used with permission from Bartleby.com)
Figure 2.
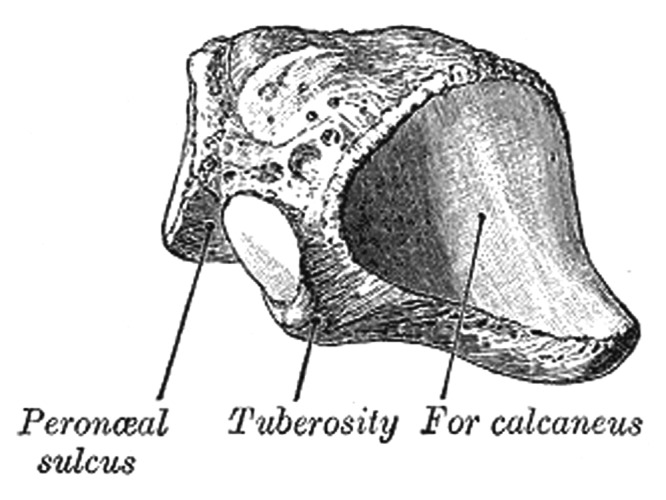
Left cuboid posterolateral view. (From Gray’s Anatomy. Used with permission from Bartleby.com)
The cuboid rotates as much as 25° during inversion/eversion about an axis that passes from posteroinferior to anterosuperior at an angle of roughly 52° (range, 43°-72°) with respect to the ground.15,42 In addition to inversion/eversion, there is some evidence that posterior-anterior distraction of the CC joint also occurs during the gait cycle.15
The CC joint is intrinsically stable due to the congruence of its articular surfaces and reinforcement from ligaments and tendon attachments (Figure 3).8,41,43 The CC joint appears to be maximally congruent radiographically when the calcaneus is placed in a vertical position.18 The dorsal and plantar cuboideonavicular and cuboideometatarsal ligaments and wedge-shaped fibroadipose labra within the CC joint and cuboid-metatarsal joints contribute to stability.3,8,9,19,27,41,42,50
Figure 3.

The ligaments of the lateral foot. (From Gray’s Anatomy. Used with permission from Bartleby.com)
The peroneus longus tendon, which forms a sling around the lateral and plantar aspects of the cuboid before inserting on the plantar aspect of the lateral first metatarsal base and medial cuneiform, also assists with CC joint stabilization (Figure 4).3,47 The cuboid is a pulley for the peroneus longus tendon; muscle contraction from midstance through the late propulsive phase exerts an eversion torque on the cuboid.2,20,22,23 Eversion of the cuboid via the peroneus longus tendon is thought to facilitate load transfer across the forefoot from lateral to medial as stance progresses.3
Figure 4.
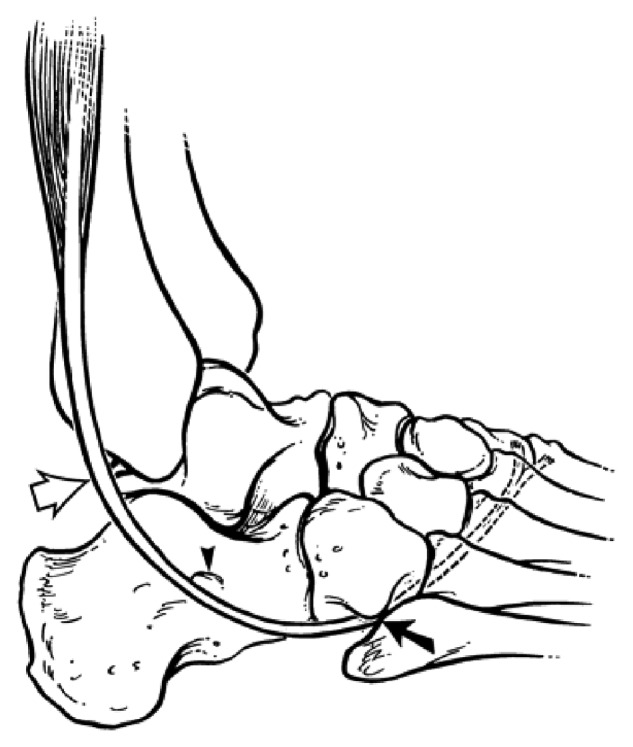
The peroneus longus tendon. (From Rademaker J, Sadka Rosenberg Z, Delfaut EM, et al. Tear of the peroneus longus tendon: MR imaging features in nine patients. Radiology 2000;214:700-704. Used with permission from The Radiological Society of North America.)
Although the normal mechanics of the midtarsal joints are not fully understood, the midtarsal joints (talonavicular and CC) are thought to play a vital role in the transition of the foot from a mobile adapter during weight acceptance to a rigid lever during push-off and in rearfoot-to-forefoot load transfer during propulsion.46 Load transfer should occur from the lateral-to-medial forefoot to facilitate an effective “windlass effect” when the metatarsophalangeal joints extend.3 During early stance when the calcaneus is everted, the forefoot tends to flex and extend more; during push-off, the calcaneus is inverted, and the forefoot is more rigid.46 This phenomenon is attributed to the orientation of the talonavicular and CC joint axes,11 which become parallel during calcaneal eversion, increasing motion in these joints and in the forefoot in general.11 Conversely, calcaneal inversion during push-off causes the midtarsal joint axes to diverge, which reduces mobility in the midtarsal joint and the forefoot. Forefoot flexion/extension may increase when the calcaneus everts, even though cuboid and navicular mobility decrease.46
Etiology
Several causes have been proposed for cuboid syndrome, including excessive pronation, overuse, and inversion ankle sprains.2,21,24,31,34,36,45 Although the precise pathomechanic mechanism is unclear, cuboid syndrome is thought to arise from forceful eversion of the cuboid while the calcaneus is inverted, with resultant disruption of CC joint congruity.2,21,31,34,36 Loss of congruence between the calcaneus and cuboid, which may be imperceptible during exam ination, may be the source of lateral foot pain. The peroneus longus may play a role in the development of cuboid syndrome, since this muscle imparts an eversion moment on the cuboid.2,5,31,34 Impaired peroneus longus function may affect CC joint stability.3,17
Several factors may increase the likelihood of cuboid syndrome, including midtarsal instability, excessive body weight, ill-fitting or poorly constructed orthoses or shoes, exercise (ie, intensity, duration, frequency), inadequate exercise recovery, training on uneven surfaces, and sprain of the foot or ankle.2,21,31,34,36,45 Cuboid syndrome may be more prevalent in individuals with pronated feet due to the increased moment arm of the peroneus longus.2,36,37 In one study, 80% of the patients with cuboid syndrome presented with pronated feet,36 but it can also occur with pes cavus (supinated) feet.31,45,48
Fibroadipose synovial folds (or labra) between the CC and cubometatarsal joints may be part of the cause of cuboid syndrome.19,27 These labra are comprised of highly vascular loose connective tissue with a thin lining of synoviocytes capable of producing synovitis.27 The labra can restrict joint motion or become impinged. In a cadaveric study on 41 human feet, the labrum between the calcaneus and cuboid occupied approximately 35% of the CC joint space, more than any other joint in the foot.27 The audible “click” or “pop” that occurs during manipulation of a “locked” cuboid may be the reduction of an obstructive labrum.
The prevalence of cuboid syndrome is unclear. Roughly 4% of 3600 athletes evaluated with foot injuries had symptoms originating from the cuboid.36 Cuboid syndrome was found in 17% of professional ballet dancers with foot or ankle injuries and 6.7% of patients with plantar flexion/inversion ankle sprains.21,31
Clinical Findings
The symptoms of cuboid syndrome resemble those of a ligament sprain. Pain is often diffuse along the lateral foot between the CC joint and the fourth and/or fifth cuboid-metatarsal joints and may radiate throughout the foot.2,5,21,31 A slight sulcus over the dorsum of the cuboid and/or a slight prominence or fullness on the plantar surface may be present with subluxation along with erythema, edema, and/or ecchymosis.2,29,31,34,36,37,44
Tenderness may be present along the peroneus longus tendon, the cuboid groove, the dorsolateral and/or plantar cuboid,2,29,31,36 or the origin of the extensor digitorum brevis muscle.2 Ankle and/or foot active and passive range of motion may be decreased due to pain.31,34 Resisted ankle/foot eversion or inversion may elicit pain.21,45
Antalgic gait is common with cuboid syndrome, with pain and/or weakness most pronounced during push-off or with side-to-side movements.2,31,36 Hopping may elicit symptoms,31 which increase with weightbearing and decrease with rest.37
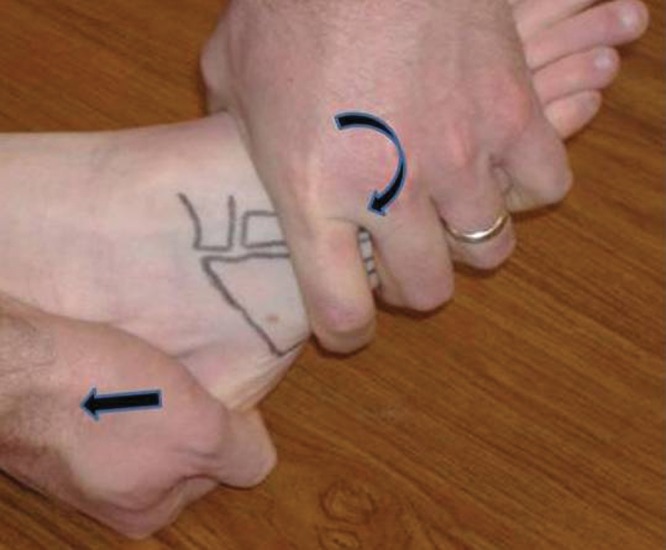
Although there are no definitive validated diagnostic tests for cuboid syndrome, two clinical maneuvers have been described—the midtarsal adduction test and the midtarsal supination test.21 During the adduction test, the midtarsal joint is manipulated passively in the transverse plane (about a superior-inferior axis) while the calcaneus is stabilized (Figure 5). This maneuver compresses the medial aspect of the CC joint and distracts the lateral side. The supination test is similar by adding inversion (frontal plane) and plantar flexion (sagittal plane) (Figure 6).21
Figure 5.

Midtarsal adduction test.
Figure 6.
Midtarsal supination test.
Pain may also be elicited when the cuboid is passively translated dorsally or plantarly (Figure 7).31 This motion is decreased when the cuboid is “locked.” The diagnostic accuracy of these maneuvers has not been determined.
Figure 7.

Dorsal-plantar cuboid shear test.
Imaging
Radiography, computerized tomography, and magnetic resonance imaging have not improved the diagnosis of cuboid syndrome,2,31,34,36 in part because nonpathologic variations in lateral foot anatomy are common.2,32 Aberrations in midtarsal joint alignment that produce symptoms in weightbearing may also be undetectable with radiography if foot radiographs are obtained nonweightbearing.13 Plain radiographs can rule out fractures or other significant bony abnormalities and help establish a differential diagnosis.
Differential Diagnosis
Because of the difficulty in diagnosing cuboid syndrome, the differential diagnosis of lateral foot pain should include fracture or dislocation of the cuboid, calcaneus, or fourth or fifth metatarsals, calcaneonavicular coalition, peroneal or extensor digitorum brevis tendinopathy, plantar fasciitis, sinus tarsi syndrome, meniscoid of the ankle, gout, tarsitis, Lisfranc injury, compression neuropathy of the sural nerve, lateral plantar nerve entrapment, and anterolateral ankle impingement.30 Approximately 90% of tarsal coalitions occur either at the calcaneonavicular joint or the talocalcaneal joint.5,6,26,30,32,37,39 Isolated fractures of the cuboid are rare33 as are cuboid dislocations, with only 13 reported cases in the literature.†
Cuboid syndrome may be misdiagnosed as a lateral ankle sprain or overlooked when it develops in conjunction with a lateral ankle injury.1,21 Persistent pain in the CC joint region after lateral ankle symptoms have subsided should raise suspicion of cuboid syndrome.21
Treatment
Multiple sources have recommended manipulation of the cuboid2,21,31,34,36 as the initial treatment for cuboid syndrome unless contraindicated (ie, bone disease, inflammatory arthritis, gout, neural or vascular compromise, or fracture).5 Two techniques have been described—the cuboid whip (Figure 8)36 and the cuboid squeeze (Figure 9).31 For the cuboid whip, the clinician cups the dorsum of the patient’s forefoot, placing thumbs on the plantomedial aspect of the cuboid. The patient’s knee is flexed 70° to 90° while the ankle is placed in 0° dorsiflexion.36 With the patient’s leg relaxed, the clinician abruptly “whips” the foot into inversion and plantarflexion while delivering a low-amplitude, high-velocity thrust (via the thumbs) to the cuboid (Figure 8). A “pop” or shift may be heard and/or felt by the clinician and/or patient during the thrust.2,31 During the cuboid squeeze, the clinician slowly stretches the ankle into maximal plantarflexion and the foot and toes into maximal flexion. When the clinician feels the dorsal soft tissues relax, the cuboid is “squeezed” (ie, forced dorsal) with the thumbs (Figure 9). The cuboid squeeze may not be appropriate for patients who have a coincident lateral ankle sprain, because the ankle is maximally plantarflexed before the manipulation. Manipulation of the cuboid should be attempted only when edema and ecchymosis have significantly diminished and when the injured ankle capsule and ligaments have healed adequately to tolerate the stress of manipulation.
Figure 8.

Cuboid whip manipulation.
Figure 9.
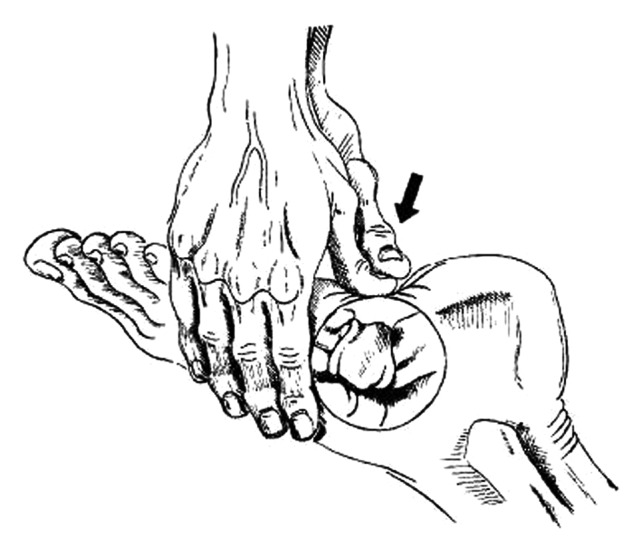
Cuboid squeeze technique. (From Marshall P, Hamilton WG. Cuboid subluxation in ballet dancers. Am J Sports Med. 20(2)169-175, 1992. Used with permission.)
Heel raise tolerance and/or reduced discomfort with passive dorsal-plantar cuboid gliding may be evidence of improvement after manipulation. Patients who experience partial or incomplete symptom resolution may benefit from additional manipulations. There appears to be an association between the duration of symptoms and the number of manipulations required for complete symptom resolution.21,36 Some patients experience mild discomfort after the manipulation and may benefit from cryotherapy, nonthermal ultrasound, pain-modulating electrical stimulation, or therapeutic massage.2,21,34 Patients should be advised to avoid vigorous weightbearing activities (eg, running) for several days after manipulation.2,31
Following successful manipulation, recurrence may be prevented by employing taping, orthoses, and/or cuboid padding.2,31,36 Various taping techniques have been suggested, with a common goal of supporting the medial longitudinal arch.2,5,31,34 Padding to support the plantar cuboid is commonly recommended for cuboid syndrome.2,29,31,36,37 The dimensions, thickness, and placement of the pad beneath the medial aspect of the cuboid are adjusted to prevent eversion of the cuboid (felt with a thickness of 1/8 or 1/4 in. [3-6 mm]).51 A lateral wedge under the calcaneus may also help reduce pain with weightbearing.
Patients who do not experience relief after manipulation should be reexamined and other diagnoses considered, including isolated sprain of the lateral midfoot ligaments. Immobilization of the foot/ankle, coupled with crutch/cane unloading, is advisable. Orthoses may reduce excessive pronation2,36,45 and may prevent a recurrence of cuboid syndrome.2,29 Stretching the gastrocnemius, soleus, hamstring, and/or peroneus longus and strengthening the intrinsic and extrinsic foot muscles may help prevent recurrence of cuboid syndrome.29,34
Summary
Cuboid syndrome is a relatively common, painful condition of the lateral midfoot that can be difficult to recognize because there are no definitive diagnostic procedures. Imaging is of little value. The diagnosis is based on the patient’s history and the presence of signs and symptoms. Cuboid syndrome may respond favorably to manipulation.
Footnotes
References
- 1. Baravarian B. Diagnostic dilemmas: a guide to understanding and treating lateral column pain. Podiatry Today. 2005;18(3):100-105 [Google Scholar]
- 2. Blakeslee TJ, Morris JL. Cuboid syndrome and the significance of midtarsal joint stability. J Am Podiatr Med Assoc. 1987;77(12):638-642 [DOI] [PubMed] [Google Scholar]
- 3. Bojsen-Moller F. Calcaneocuboid joint and stability of the longitudinal arch of the foot at high and low gear push off. J Anat. 1979;129:165-176 [PMC free article] [PubMed] [Google Scholar]
- 4. Buscemi MJ, Jr, Page BJ. Transcuneiform fracture: cuboid dislocation of the midfoot. J Trauma. 1986;26(3):290-292 [DOI] [PubMed] [Google Scholar]
- 5. Caselli MA, Pantelaras N. How to treat cuboid syndrome in an athlete. Podiatry Today. 2004;17(10):76-80 [Google Scholar]
- 6. Dewar FP, Evans DC. Occult fracture subluxation of the midtarsal joint. J Bone Joint Surg Br. 1968;50:386. [PubMed] [Google Scholar]
- 7. Dobbs MB, Crawford H, Saltzman C. Fibularis longus tendon obstructing reduction of cuboid dislocation: a report of two cases. J Bone Joint Surg Am. 2001;83:1387-1391 [DOI] [PubMed] [Google Scholar]
- 8. Dorn-Lange NV, Nauck T, Lohrer H, Arentz S, Konerding MA. Morphology of the dorsal and lateral calcaneocuboid ligaments. Foot Ankle Int. 2008;29(9):942-949 [DOI] [PubMed] [Google Scholar]
- 9. Draves DJ. Anatomy of the Lower Extremity. Baltimore, MD: Lippincott Williams & Wilkins; 1986 [Google Scholar]
- 10. Drummond DS, Hastings DE. Total dislocation of the cuboid bone: report of a case. J Bone Joint Surg Br. 1969;51:716-718 [PubMed] [Google Scholar]
- 11. Elftman H. The transverse tarsal joint and its control. Clin Orthop. 1960;16:41-45 [PubMed] [Google Scholar]
- 12. Fagel VL, Ocon E, Cantarella JC, Feldman F. Case report 183: dislocation of the cuboid bone without fracture. Skeletal Radiol. 1982;7:287-288 [DOI] [PubMed] [Google Scholar]
- 13. Gamble FO, Yale I. Clinical Foot Roentgenology. Baltimore, MD: Lippincott Williams & Wilkins; 1975 [Google Scholar]
- 14. Gough DT, Broderick DF, Kanuzik SJ, Cusak TJ. Isolated dislocation of the cuboid bone without fracture. Ann Emerg Med. 1988;17(10):1095-1096 [DOI] [PubMed] [Google Scholar]
- 15. Greiner TM, Ball KA. The calcaneocuboid joint moves with three degrees of freedom. J Foot Ankle Res. 2008;1(suppl 1):O39 [Google Scholar]
- 16. Hardy RH. Observations on the structure and properties of the plantar calcaneo-navicular ligament in man. J Anat. 1951;85(2):135-139 [PMC free article] [PubMed] [Google Scholar]
- 17. Harradine P, Bevan L, Carter N. An overview of podiatric biomechanics theory and its relation to selected gait dysfunction. Physiotherapy. 2006;92:122-127 [Google Scholar]
- 18. Hlavac HF. Differences in x-ray findings with varied positioning of the foot. J Am Podiatry Assoc. 1967;57(10):465-471 [DOI] [PubMed] [Google Scholar]
- 19. Hollander JD, Lidtke RH, Lai JY. The labrum of the calcaneocuboid joint. J Foot Ankle Surg. 1998;37(4):308-312 [DOI] [PubMed] [Google Scholar]
- 20. Houtz SJ, Walsh FP. Electromyographic analysis of the function of the muscles acting on the ankle during weight-bearing with special reference to the triceps surae. J Bone Joint Surg Am. 1959;41:1469-1481 [PubMed] [Google Scholar]
- 21. Jennings J, Davies GJ. Treatment of cuboid syndrome secondary to lateral ankle sprains a case series. J Orthop Sports Phys Ther. 2005;35(7):409-415 [DOI] [PubMed] [Google Scholar]
- 22. Johnson CH, Christensen JC. Biomechanics of the first ray: part I. The effects of peroneus longus function: a three-dimensional kinematic study on a cadaver model. J Foot Ankle Surg. 1999;38(5):313-321 [DOI] [PubMed] [Google Scholar]
- 23. Jonsson B, Rundgren A. The peroneus longus and brevis muscles: a roentgenologic and electromyographic study. Electromyography. 1971;11(1):93-103 [PubMed] [Google Scholar]
- 24. Khan K, Brown J, Vass N, et al. Overuse injuries in classical ballet. Sports Med. 1995;19(5):341-357 [DOI] [PubMed] [Google Scholar]
- 25. Kolker D, Marti CB, Gautier E. Pericuboid fracture-dislocation with cuboid subluxation. Foot Ankle Int. 2002;23(2):163-167 [DOI] [PubMed] [Google Scholar]
- 26. Leerar PJ. Differential diagnosis of tarsal coalition versus cuboid syndrome in and adolescent athlete. J Orthop Sports Phys Ther. 2001;31(12):702-707 [DOI] [PubMed] [Google Scholar]
- 27. Lidtke R, George J. Anatomy, biomechanics, and surgical approach to synovial folds within the joints of the foot. J Am Podiatr Med Assoc. 2004;94:519-527 [DOI] [PubMed] [Google Scholar]
- 28. Littlejohn SG, Line LL, Yerger LB., Jr Complete cuboid dislocation. Orthopedics. 1996;19:175-176 [DOI] [PubMed] [Google Scholar]
- 29. MacIntyre J, Joy E. The athletic woman foot and ankle injuries in dance. Clin Sports Med. 2000;1(2):351-368 [DOI] [PubMed] [Google Scholar]
- 30. Main BJ, Jowett RL. Injuries of the midtarsal joint. J Bone Joint Surg Br. 1975;57:89. [PubMed] [Google Scholar]
- 31. Marshall P, Hamilton WG. Cuboid subluxation in ballet dancers. Am J Sports Med. 1992;20(2)169-175 [DOI] [PubMed] [Google Scholar]
- 32. McDonough MW, Ganley JV. Dislocation of the cuboid. J Am Podiatr Med Assoc. 1973;63:317-318 [DOI] [PubMed] [Google Scholar]
- 33. Miller SR, Handzel C. Isolated cuboid fracture: a rare occurrence. J Am Podiatr Med Assoc. 2001;91(2):85-88 [DOI] [PubMed] [Google Scholar]
- 34. Mooney M, Maffey-Ward L. Cuboid plantar and dorsal subluxations assessment and treatment. J Orthop Sports Phys Ther. 1994;20(4):220-226 [DOI] [PubMed] [Google Scholar]
- 35. Nester CJ, Findlow AH. Clinical and experimental models of the midtarsal joint: proposed terms of reference and associated terminology. J Am Podiatr Med Assoc. 2006;96(1):24-31 [DOI] [PubMed] [Google Scholar]
- 36. Newell SG, Woodle A. Cuboid syndrome. Phys Sports Med. 1981;9(4):71-76 [DOI] [PubMed] [Google Scholar]
- 37. Omey ML, Micheli LJ. Foot and ankle problems in the young athlete. Foot Ankle. 1999;31(7):S470-S486 [DOI] [PubMed] [Google Scholar]
- 38. Penhallow DP. An unusual fracture: dislocation of the tarsal scaphoid with dislocation of the cuboid. J Bone Joint Surg Am. 1937;19:517-519 [Google Scholar]
- 39. Phillips RM. Dysfunction of the fibularis longus after fracture of the cuboid. J Foot Surg. 1985;24:99. [PubMed] [Google Scholar]
- 40. Punwar S, Madhav R. Dislocation of the calcaneocuboid joint presenting as lateral instability of the ankle. J Bone Joint Surg Br. 2007;89:1247-1248 [DOI] [PubMed] [Google Scholar]
- 41. Sammarco VJ. The talonavicular and calcaneocuboid joints: anatomy, biomechanics, and clinical management of the transverse tarsal joint. Foot Ankle Clin. 2004;9(1):127-145 [DOI] [PubMed] [Google Scholar]
- 42. Sarrafian SK. Anatomy of the Foot and Ankle. Philadelphia, PA: JB Lippincott; 1983 [Google Scholar]
- 43. Smith JS, Flemister AS. Complete cuboid dislocation in a professional baseball player. Am J Sports Med. 2006;34(1):2-3 [DOI] [PubMed] [Google Scholar]
- 44. Starkey C, Ryan JL. Evaluation of Orthopedic and Athletic Injuries. 2nd ed. Philadelphia, PA: FA Davis; 1996 [Google Scholar]
- 45. Subotnick SI. Peroneal cuboid syndrome. J Am Podiatr Med Assoc. 1989;79(8):413-414 [DOI] [PubMed] [Google Scholar]
- 46. Suckel A, Muller O, Langenstein P, Herberts T, Reize P, Wulker N. Chopart’s joint load during gait in vitro study of 10 cadaver specimen in a dynamic model. Gait Posture. 2008;27:216-222 [DOI] [PubMed] [Google Scholar]
- 47. Sutherland DH. The evolution of clinical gait analysis, part I: kinesiological EMG. Gait Posture. 2001;14:61-70 [DOI] [PubMed] [Google Scholar]
- 48. Valmassy RL. Pathomechanics of lower extremity function. In: Valmassy RL, ed. Clinical Biomechanics of the Lower Extremities. St Louis, MO: Mosby-Year Book Inc; 1996:59-84 [Google Scholar]
- 49. Wainwright AM, Parmar HV, Gregg PJ. Calcaneocuboid dislocation in a case of Ehlers-Danlos syndrome. Injury. 2003;24(4):274. [DOI] [PubMed] [Google Scholar]
- 50. Ward KA, Soames RW. Morphology of the plantar calcaneocuboid ligaments. Foot Ankle Int. 1997;18:649-653 [DOI] [PubMed] [Google Scholar]
- 51. White SC. Padding and taping techniques. In: Valmassy RL, ed. Clinical Biomechanics of the Lower Extremities. St Louis, MO: Mosby-Year Book Inc; 1996:367-390 [Google Scholar]