

Abstract
Background:
Little is known about the return to sports after anterior cruciate ligament reconstruction and whether sex differences exist regarding the level and timing at which athletes return.
Hypotheses:
Compared to school-aged girls, boys return to full sports earlier and at a higher frequency after surgery (1). Athletes who return to sports earlier will not have a higher incidence of subsequent injury to either knee after surgery (2).
Study Design:
Cohort.
Methods:
The patient population comprised 413 consecutive school-aged athletes who were injured while competing in basketball or soccer. Patients were enrolled prospectively, and activity levels were obtained through follow-up visits, surveys, phone calls, and e-mail.
Results:
Follow-up was obtained for 402 patients (basketball: 58 boys, 242 girls; soccer: 25 boys, 77 girls). Eighty-seven percent of girls and boys returned to high school basketball after surgery: the mean time to return to full participation in basketball was 5.2 ± 2.1 months for girls and 5.3 ± 2.2 months for boys (P = .92). Similarly, 93% of girls and 80% of boys returned to compete in high school soccer after surgery (P = .13); the mean time to return to full participation in soccer was 5.1 ± 1.9 months for girls and 5.1 ± 2.0 for boys (P = 1.00). About 20% of athletes went on to compete in their sport in college. The time of return to sports was not a statistically significant factor for the incidence of subsequent anterior cruciate ligament injury.
Conclusion:
Of 402 athletes competing in basketball and soccer, women and men returned at the same rate and same level of sport after surgery. Athletes who returned to sports at earlier times after surgery did not have a higher incidence of subsequent anterior cruciate ligament injury than patients who returned at later times.
Keywords: anterior cruciate ligament, adolescents, return to sports, reinjury, gender
It is generally accepted among athletes that the measure of success from the reconstruction of an anterior cruciate ligament (ACL) is whether the patient is able to return to the preinjury level of sport after surgery. The percentage of patients who return to some level of sport has been reported to be from 26% to 97%.3,5-12,14-16,18,19 Few studies examine differences between men and women regarding their ability and timing for return to sport.
Some reports state that women need more rehabilitation visits after surgery than men2 and that men have higher physical function after ACL reconstruction than women.10 Other reports find no significant differences between men and women in functional knee tests2 and no significant differences regarding return to activity.23
Limited information appears in the literature regarding the return to specific sports at specific activity levels and age groups. Seto et al16 reported that athletes who participated in sports involving cutting and twisting motions were less successful in returning to preinjury activity level after ACL reconstruction. Others suggest that competitive athletes return to preinjury level of activity and sport-related function more quickly and successfully than nonathletes.9,23 A widely accepted guideline is that return to full activity should not be permitted until 6 months postoperatively; however, a range of 4.1 to 8.1 months for return to sports has been reported.11,12,18,22
Although these reports provide some parameters for patients asking questions about their ability to return to sports, most young competitive athletes want specific information relating to the return to their specific sports and the chance of reinjury after surgery. In our experience, school-aged athletes have a specific time frame of when they want to return to sports. The time is usually related to the next competitive season. Most athletes in basketball and soccer compete year-round, with 1 competitive season committed to their local school and with the other dedicated to a highly competitive team that travels regionally and nationally. These athletes ask specific questions, such as “When will I be able to start practicing my sport?” “When will I be able to return to full sports?” “Will I be able to play as well as I do now?” and “What is my chance of reinjury?” We want to answer all these questions as accurately as we can. The question of subsequent injury is an important question because these athletes are young and have several years of competitive sports available to them. Knowing the subsequent rates specific to the sport may be helpful for counseling patients preoperatively.
Therefore, the purpose of our study was to determine whether male and female school-aged athletes in basketball and soccer returned to their sports at the same level and at the same time after ACL reconstruction and whether the time of return to sports affected subsequent ACL injury rates in those sports. We hypothesized the following:
Hypothesis 1: Compared to school-aged girls, boys return to full sports earlier and at a higher frequency after surgery.
Hypothesis 2: Athletes who return to sports earlier will not have a higher incidence of subsequent injury to either knee after surgery.
Materials and Methods
From September 1992 to June 2005, the senior author performed 2999 ACL reconstructions with patellar tendon autografts using the surgical technique previously described.17 For our purposes, 353 patients were excluded from the study because they had suffered ACL injuries to both knees before the ACL reconstruction. From the remaining 2646 patients, 413 had competed in and were injured in the high-risk, competitive sports of basketball or soccer (middle school or high school). Participation in competitive basketball or soccer, either for the school that they attended or for an organized travel team, was criterion for inclusion and was considered to be an activity level of 9, per the activity rating scale previously published21; this level includes all sports that involve pivoting, cutting, or jumping. We included only those patients who were 17 years old or younger to ensure that the athlete had the opportunity to return to the same level of competition for a minimum of 1 more athletic season after surgery (Figure 1). Parents signed an informed consent form, and patients signed an informed assent form to participate in the study, which was approved by the institutional review board at the hospital where the senior author performed surgery.
Figure 1.
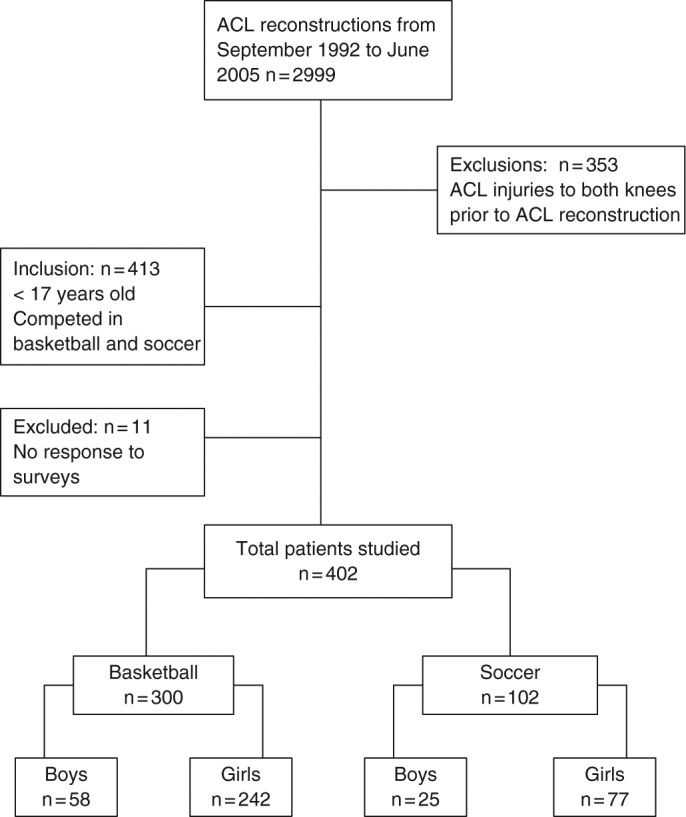
Patient population.
Prospective data were collected for each patient as a part of an ongoing and long term follow-up study. For the purposes of this study, relevant data included the age, sex, and preoperative and postoperative sport played. Patients were asked to complete the activity rating survey21 postoperatively at 6 months, 1 year, and yearly thereafter as a measure to evaluate (1) the athletes’ abilities to return to basketball and soccer at level 9 and (2) whether they went on to play their sports in college.
Return-to-Activity Surveys
Postoperatively, patients were asked to fill out a questionnaire regarding their return to functional low-level activities related to their primary sport. In the study population, this included shooting baskets or kicking a soccer ball, in addition to other individual sport-specific drills. Patients recorded the amount of time (in weeks) that it took to reach this low level of activity. The survey was administered during regular follow-up visits at 1, 2, 3, and 4 months after surgery, until the patient reported that he or she returned to that low level.
In addition, the patients completed a questionnaire that asked them how long it took (in months) to return to “full activity level at full capability including team competition.” The patients had an option on the questionnaire to answer, “I have not returned to full capability yet.” The questionnaire was administered to patients at 2-month intervals, beginning 2 months postoperatively. Patients who answered that they had returned to full activities did not continue to receive the survey; patients who had not yet returned to full activities received the survey again 2 months later. Those patients who did not respond to the questionnaire in a timely fashion were contacted via e-mail or telephone to obtain the completed questionnaires.
Guidelines for Return to Sport
Patients were not given a specific time frame for return to the different activities; that is, they were allowed to return when they felt comfortable. However, specific guidelines were prescribed for the progression for return. The initial goals of rehabilitation were to minimize swelling and obtain full knee range of motion equal to that of the noninvolved knee. Then, leg-strengthening exercises were introduced. Patients were allowed to begin low-level agility drills and functional sports drills, alone at first and then progressing to 1-on-1 and team drills as able. Patients were advised to go through the progression comfortably while monitoring range of motion, swelling, and soreness. They were instructed to decrease their activities if they lost any knee motion or had increased swelling or pain. The goal prescribed for patients was that when they obtained 85% quadriceps muscle strength in the involved knee (compared with the other knee), they could return to team competition. During this progression, athletes would typically participate in the drills and competition every other day at first, to keep adverse symptoms to a minimum. Again, no time frame was outlined for the athletes. The final outcome measure for performance was as follows: “When did you return to full activity level at full capability including team competition?” This question was distinctly different from asking when they returned to play their sport at any level.
Subsequent Injury Data
As part of a yearly survey, patients were able to report any subsequent injury to either knee. Most patients who had another injury returned to our clinic for care. When patients sought treatment elsewhere, records were obtained. For the purposes of this study, any ACL injury reported at any time after surgery was counted. Patients who had surgery earlier in the study period were followed longer for a possible injury. We did not set a time limit for follow-up, because the average age of patients was that of high school sophomore. We wanted to capture any ACL injury in an athlete who went on to compete in college.
Statistical Analysis
Two-tailed t test analysis of parametric data was performed to determine whether there was a statistically significant difference between groups for time to return to full participation in sports at full capability. To determine if an equal number of boys and girls returned to full sports, a chi-square analysis was performed. Logistic regression using likelihood ratio chi-square analysis was performed to determine whether the time of return to full sports (recorded in months as a continuous variable) affected the injury rates to either knee. Fisher’s exact test was used to determine whether the time of return to full sports was significant for the incidence of subsequent ACL graft tear or ACL tear to the opposite normal knee. Statistical significance was set at P < .05.
Results
Patient Population
Of the 413 patients who met the criteria for the study, 402 responded to the questionnaires. The patient population consisted of 83 boys (21%) and 319 girls (79%) aged 12 to 17 years. The mean age of girls was 15.6 years (± 1.0 years), whereas the mean age of boys was 15.7 years (± 0.9 years). Of the total 402 patients, 102 were injured playing soccer (77 girls and 25 boys) and 300 were injured in basketball (242 girls and 58 boys). The mean age of the patients in the soccer group was 15.7 years (15.7 for girls and 15.8 for males) and the mean age of the basketball group was 15.6 years (15.5 for girls and 15.7 for boys).
Return to Activity
The mean follow-up time regarding the athletes’ abilities to return to sports and any subsequent injury rates was 9.8 ± 5.2 years (range, 2.1-15.2). Eighteen of the 402 athletes (2 boys in basketball, 12 girls in basketball, and 4 girls in soccer) had surgery at a young enough age that they were not yet in college at the latest follow-up time. We were not able to determine whether they could compete at that level.
The mean time after surgery that patients returned to low-level functional sport activity was 6.0 ± 3.8 weeks. In the soccer group, the mean time was 5.3 ± 2.2 weeks for girls and 5.8 ± 2.1 weeks for boys (P = .69). In the basketball group, the mean time was 6.1 ± 4.2 weeks for girls and 6.7 ± 4.4 weeks for boys (P = .53).
For basketball, 87% of girls and boys returned to compete in high school basketball after surgery, and 21% of girls and 17% of boys went on to compete in basketball in college (Figure 2). The mean time to return to full participation in basketball was 5.2 ± 2.1 months for girls and 5.3 ± 2.2 months for boys (P = .92) (Figure 3).
Figure 2.
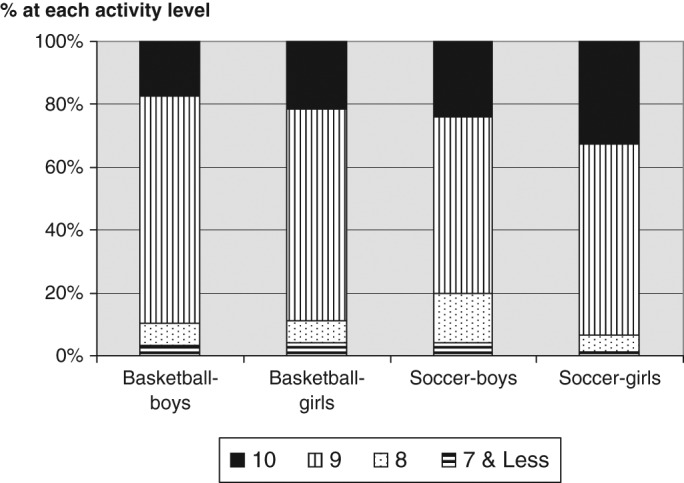
Highest activity level obtained after surgery. Level 10 indicates that athletes are competing at the professional, elite, or college level in sports involving jumping, pivoting, or twisting. Levels 8 and 9 include the same sports as level 10, but level 9 is competition at the school or club level and level 8 is at the recreational level.
Figure 3.
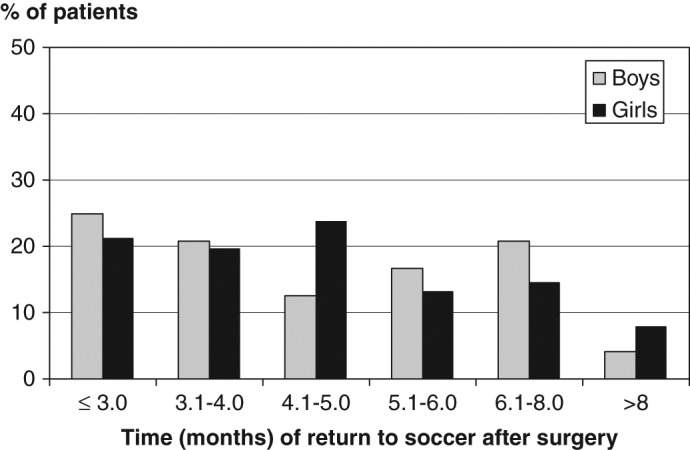
Percentage of athletes who returned to full competitive soccer, postoperatively: 40% before 4 months, 35% between 4 and 6 months, and 25% after 6 months. The mean time of return was 5.1 months for boys and girls (P = 1.00).
For soccer, 93% of girls and 80% of boys returned to compete in high school soccer after surgery (P = .13), and 33% of girls and 24% of boys went on to compete in soccer in college (P = .47). The mean time to return to full participation in soccer was 5.1 ± 1.9 months for girls and 5.1 ± 2.0 for boys (P = 1.00) (Figure 4).
Figure 4.
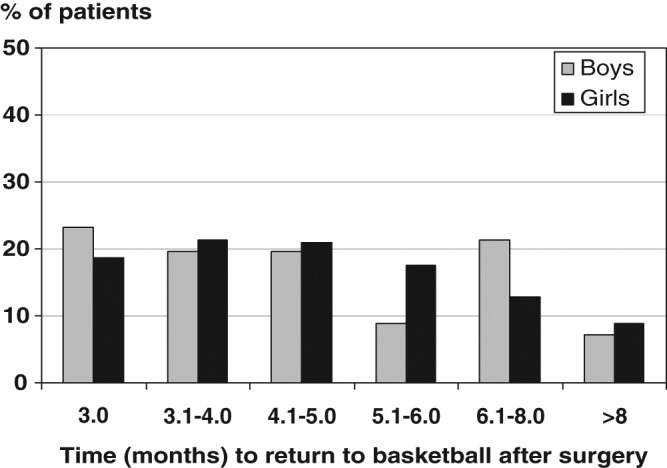
Percentage of athletes who returned to full competitive basketball, postoperatively: 40% before 4 months, 35% between 4 and 6 months, and 25% after 6 months. The mean time of return was 5.2 months for girls and 5.3 months for boys (P = .92).
Subsequent ACL injury
There was no statistically significant difference for the incidence of ACL injury to either the ACL-reconstructed knee or the contralateral knee between boys and girls for either sport. The time to return to sport at full capability was not a statistically significant factor related to subsequent injury to either knee for boys or girls within each sport (Table 1).
Table 1.
Subsequent injury to ACL-reconstructed knee (graft tear) or to the contralateral normal knee (contralateral tear).
| Sport (n) | Time of Return to Full Sports at Full Capability, MoMean ± SD | Graft tear N (%) | Time of Reinjury, Mo Mean ± SD | P Valuea | Contralateral Tear N (%) | Time of Contralateral Injury, Mo Mean ± SD | P Valueb |
|---|---|---|---|---|---|---|---|
| Basketball | |||||||
| Girls (242) | 5.2 ± 2.1 | 17 (7.0) | 24.6 ± 23.8 | .23 | 39 (16.1) | 30.2 ± 22.7 | .40 |
| Boys (58) | 5.3 ± 2.2 | 8 (13.8) | 22.9 ± 14.3 | .36 | 7 (12.1) | 34.3 ± 30.1 | .88 |
| P Valuec | .11 | .44 | |||||
| Soccer | |||||||
| Girls (77) | 5.1 ± 1.9 | 10 (13.0) | 18.3 ± 16.0 | .41 | 15 (19.5) | 32.0 ± 24.4 | .24 |
| Boys (25) | 5.1 ± 2.0 | 6 (24.0) | 18.7 ± 9.4 | .27 | 2 (8.0) | 36.4 ± 23.6 | .80 |
| P Valuec | .21 | .18 | |||||
Statistical significant difference between time of return to full participation in sports and the time of subsequent ACL graft tear.
Statistical significant difference between time of return to full participation in sports and the time of contralateral injury.
Statistical significant difference for the incidence of injury between boys and girls.
Discussion
This study evaluated the ability to return to sport for school-aged athletes competing in basketball and soccer. The results showed no statistically significant difference between the sexes for the time that it took to return to sport or for the final level of competition possible. Furthermore, the data showed that the time of return to full sport did not affect the incidence of subsequent ACL injury to either knee; there was also no difference in the injury rates between boys and girls.
The ability to return to the preinjury activity level varies greatly between studies.3,5-12,14-16,18 The difference is mostly likely due to the large variance between studies in the mean surgery age of the patients, between 21 and 35 years, which indicates that many patients were recreational athletes at the time of surgery. Young competitive athletes are highly motivated to return to competition, whereas older recreational athletes may be satisfied with playing sports at a lower level than before surgery.
In a study of 50 competitive athletes who participated in mostly basketball, volleyball, and soccer, Nakayama et al12 found that 92% were able to return to sports at the preinjury level. The mean age of the patients in that study was 24.3 years (range, 19-39), which was higher than the mean age of the adolescent patient population of our study. In a study of 77 competitive athletes with a mean age of 21 years, Smith et al23 reported that 62 were able to return to sports by 12 months postoperatively; of those athletes, 55 were able to return to competitive sports at the preinjury level or higher. Compared to the current study, these 2 studies have similar, high percentages of patients who returned to their preinjury levels of sport.
The results of our study showed that of 402 ACL-reconstructed middle school and high school patients, about 20% went on to compete at the collegiate level in their sport. This is significant because, as the National Collegiate Athletic Association reports, about only 3% of high school basketball players, boys or girls, go on to play at the collegiate level.13 High school soccer players have slightly higher odds, with 5% going on to compete in college. We can only theorize why our patient population went on to compete in their sport in college at such a higher rate than that of the national average. We believe that ACL injuries occur in athletes who compete at a high level of intensity and who have a high number of exposure hours in their sport. Almost all athletes in the study competed in their sport year-round, and many competed in 2 sports. Perhaps the patient population in our study was biased toward the higher-level athlete with the highest number of exposure hours.
Other studies have addressed the differences between male and female athletes for their abilities to return to preinjury level and with the timing of the return to sports after surgery.2,4,8,23 Barber-Westin et al2 reported the results of ACL reconstruction between men and women with an average surgery age of 29 years. The researchers found that women required an average of 6 more rehabilitation visits after surgery, but no major differences were reported between men and women for the types of sport activities played or with the frequency of participation after surgery.
Glasgow et al4 found a difference in recovery time between men and women after ACL reconstruction. Although all the patients were encouraged to progress as quickly as possible, they were separated into 2 groups based on when they returned to sports. The first group, which returned in 6 months or less, was predominately male (84%), whereas the second group, which returned to sports after 6 months, was more evenly distributed between the sexes (45% female, 55% male). Glasgow et al4 noted the difference between the sexes and thought that it was probably a consequence of the men being more motivated and aggressive in return to sports. This study was different from ours because the mean age of the patients was 27 years (range, 18-37) and the population was a small cohort of 84 subjects of various preinjury activity levels. The larger-size, homogeneous patient population in our study (ie, 402 competitive school-aged athletes) is the factor that differentiates our study from these and the one that probably led to the differing results.
Smith et al23 studied return to competitive sports after ACL reconstruction and determined that there was no statistically significant difference between men and women; however, they did find that men had overall sports function scores significantly higher than women’s. Kvist et al8 reported that 50% of men and 57% of women returned to their preinjury activity levels with no significant differences between the sexes.
The mean period for competitive athletes to return to basketball or soccer in our study was 5.2 ± 2.1 months, which was slightly earlier than what other investigators have reported. In competitive athletes, Nakayama et al12 found that the mean time to return to sports was 8.1 months. Mastrokalos et al11 found that patients returned to sports at an average of 7.4 and 7.8 months after ACL reconstruction with a contralateral or ipsilateral patellar tendon graft, respectively. They also found that less than 32% of the ipsilateral and contralateral groups were able to return to preinjury activity levels. The difference in time to return to sports may again be related to the difference in the patients’ ages between studies: Younger patients have a more definite time frame and a desire to return to sports sooner.
Most important, athletes who returned to sports early (ie, 3 to 4 months after surgery) did not have a higher incidence of subsequent ACL injury to either knee when compared to those who returned later (ie, 6 months or more after surgery). This was true for both boys and girls. Young competitive athletes are eager to return to sports quickly, and the goal should be to allow them to return as soon as safely possible. Experience has shown us that patients will resume activities when they feel comfortable, although they may become sore or swollen. The results of this study did not demonstrate that the subsequent ACL injuries occurred at the time of return. If quick return to full sports was a factor for reinjury, then we would expect to see a high rate of ACL graft tears soon after the return to sports. However, the mean time of subsequent ACL graft tear was 17 months for soccer (range, 4.0-68.0) and 23 months for basketball (range, 3.5-87.0).
The incidence rate for subsequent ACL injury in this study is similar to what has been reported for school-aged athletes: there is no difference between boys and girls.20 Just as ACL injury rates are highest among competitive athletes in basketball and soccer with high exposure rates,1 the subsequent injury rate is expected to be relatively high as well. The mean age at the time of surgery in this study was 15 years, which is when young athletes are competing at the highest level and with a high number of exposure hours. Furthermore, 20% of these patients went on to compete in college, where they experienced many years of high-intensity competition and many exposure hours after surgery.
Conclusion
Of 402 middle school and high school athletes who tore an ACL and competed in basketball and soccer, boys and girls returned at the same rate and at the same level of sports after surgery, with about 20% continuing competition in college. Athletes who returned to sports earlier (ie, 3 to 4 months after surgery) did not have a higher incidence of subsequent ACL injury than did those who returned later (ie, 6 months after surgery or more).
Footnotes
No potential conflict of interest declared.
References
- 1. Arendt E, Dick R. Knee injury patterns among men and women in collegiate basketball and soccer: NCAA data and review of the literature. Am J Sports Med. 1995;23:694-701 [DOI] [PubMed] [Google Scholar]
- 2. Barber-Westin SD, Noyes FR, Andrews M. A rigorous comparison between the sexes of results and complications after anterior cruciate ligament reconstruction. Am J Sports Med. 1997;25:514-526 [DOI] [PubMed] [Google Scholar]
- 3. Casteleyn PP. Management of anterior cruciate ligament lesions: surgical fashion, personal whim or scientific evidence? Study of medium- and long-term results. Acta Orthop Belg. 1998;64:327-332 [PubMed] [Google Scholar]
- 4. Glasgow SG, Gabriel JP, Sapega AA, Glasgow MT, Torg JS. The effect of early versus late return to vigorous activities on the outcome of anterior cruciate ligament reconstruction. Am J Sports Med. 1993;21:243-248 [DOI] [PubMed] [Google Scholar]
- 5. Gobbi A, Diara A, Mahajan S, Zanazzo M, Tuy B. Patellar tendon anterior cruciate ligament reconstruction with conical press-fit femoral fixation: 5-year results in athletes population. Knee Surg Sports Traumatol Arthrosc. 2002;10:73-79 [DOI] [PubMed] [Google Scholar]
- 6. Howell SM, Taylor MA. Brace-free rehabilitation, with early return to activity, for knees reconstructed with a double-looped semitendinosus and gracilis graft. J Bone Joint Surg Am. 1996;78:814-825 [DOI] [PubMed] [Google Scholar]
- 7. Keays SL, Bullock-Saxton JE, Keays AC, Newcombe PA, Bullock MI. A 6-year follow-up of the effect of graft site on strength, stability, range of motion, function, and joint degeneration after anterior cruciate ligament reconstruction: patellar tendon versus semitendinosus and gracilis tendon graft. Am J Sports Med. 2007;35:729-739 [DOI] [PubMed] [Google Scholar]
- 8. Kvist J, Ek A, Sporrstedt K, Good L. Fear of re-injury: a hindrance for returning to sports after anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 2005;13:393-397 [DOI] [PubMed] [Google Scholar]
- 9. Lee DYH, Karim SA, Chang HC. Return to sports after anterior cruciate ligament reconstruction: a review of patients with minimum 5-year follow-up. Ann Acad Med Singapore. 2008;37:273-278 [PubMed] [Google Scholar]
- 10. Maletis GB, Cameron SL, Tengan JJ, Burchette RJ. A prospective randomized study of anterior cruciate ligament reconstruction: a comparison of patellar tendon and quadruple-strand semitendinosus/gracilis tendons fixed with bioabsorbable interference screws. Am J Sports Med. 2007;35:384-394 [DOI] [PubMed] [Google Scholar]
- 11. Mastrokalos DS, Springer J, Siebold R, Paessler HH. Donor site morbidity and return to the preinjury activity level after anterior cruciate ligament reconstruction using ipsilateral patellar tendon autograft: a retrospective, nonrandomized study. Am J Sports Med. 2005;33:85-93 [DOI] [PubMed] [Google Scholar]
- 12. Nakayama Y, Shirai Y, Narita T, Mori A, Kobayashi K. Knee functions and a return to sports activity in competitive athletes following anterior cruciate ligament reconstruction. J Nippon Med Sch. 2000;67:172-176 [DOI] [PubMed] [Google Scholar]
- 13. National Collegiate Athletic Association Estimated probability of competing in athletics beyond the high school interscholastic level. http://www.ncaa.org/research/prob_of_competing/probability_of_competing2.html. Updated February 16, 2007 Accessed June 25, 2008
- 14. Noyes FR, Barber-Westin SD. Reconstruction of the anterior cruciate ligament with human allograft: comparison of early and later results. J Bone Joint Surg Am. 1996;78:524-537 [DOI] [PubMed] [Google Scholar]
- 15. Pinczewski LA, Deehan DJ, Slamon LJ, Russell VJ, Clingeleffer A. A five-year comparison of patellar tendon versus four-strand hamstring tendon autograft for arthroscopic reconstruction of the anterior cruciate ligament. Am J Sports Med. 2002;30:523-536 [DOI] [PubMed] [Google Scholar]
- 16. Seto JL, Orofino AS, Morrissey MC, Medeiros JM, Mason WJ. Assessment of quadriceps/hamstring strength, knee ligament stability, functional and sports activity levels five years after anterior cruciate ligament reconstruction. Am J Sports Med. 1988;16:170-180 [DOI] [PubMed] [Google Scholar]
- 17. Shelbourne KD. Anterior cruciate ligament reconstruction using mini-arthrotomy technique with either an ipsilateral or a contralateral autogenous patellar tendon graft. In: Prodromos CC, ed. The Anterior Cruciate Ligament Reconstruction and Basic Science. Philadelphia, PA: Saunders; 2008:364-372 [Google Scholar]
- 18. Shelbourne KD, Gray T. Anterior cruciate ligament reconstruction with autogenous patellar tendon graft followed by accelerated rehabilitation: a two- to nine-year followup. Am J Sports Med. 1997;25:786-795 [DOI] [PubMed] [Google Scholar]
- 19. Shelbourne KD, Gray T. Results of anterior cruciate ligament reconstruction based on meniscus and articular cartilage status at the time of surgery: five- to fifteen-year evaluations. Am J Sports Med. 2000;28:446-452 [DOI] [PubMed] [Google Scholar]
- 20. Shelbourne KD, Gray T, Haro M. Incidence of subsequent injury to either knee within 5 years after anterior cruciate ligament reconstruction with patellar tendon autograft. Am J Sports Med. 2009;37:246-251 [DOI] [PubMed] [Google Scholar]
- 21. Shelbourne KDS, Jari S, Gray T. Outcome of untreated traumatic articular cartilage defects of the knee: a natural history study. J Bone Joint Surg Am. 2003;85(suppl 2):8-16 [DOI] [PubMed] [Google Scholar]
- 22. Shelbourne KD, Urch SE. Primary anterior cruciate ligament reconstruction using contralateral autogenous patellar tendon. Am J Sports Med. 2000;28:651-658 [DOI] [PubMed] [Google Scholar]
- 23. Smith FW, Rosenlund EA, Aune AK, MacLean JA, Hillis SW. Subjective functional assessments and the return to competitive sport after anterior cruciate ligament reconstruction. Br J Sports Med. 2004;38:279-284 [DOI] [PMC free article] [PubMed] [Google Scholar]