

Abstract
Background:
There have been no large-scale epidemiologic studies designed to determine the risk factors related to medical withdrawal in United States Tennis Association junior national tennis tournaments.
Hypothesis:
Risk of medical withdrawal will increase on the basis of cumulative match volume within a tournament.
Methods:
A retrospective, cross-sectional analysis was performed of data collected for every match of all 4 United States Tennis Association supernational tournaments (spring, summer, fall, winter) for the boys and girls divisions and for all age divisions (12, 14, 16, 18) during a single year (2005). Logistic regression analysis was performed to determine relative risk of all risk factors. Additional analysis was performed to determine the threshold (ie, match number) at which a player would substantially increase his or her risk of medical withdrawal.
Results:
A total of 28336 match exposures were analyzed, with an even distribution with respect to sex and age. The total medical withdrawal rate was 15.6 per 1000 match exposures. Every factor of interest was highly significant in predicting a higher rate of medical withdrawal per 1000 match exposures. The medical withdrawal rate was significantly higher in the fifth match or greater (26.3/1000) versus the first 4 matches (12.7/1000; P < .0001), even when analyzing main draw and singles matches.
Conclusion:
In United States Tennis Association national junior tennis tournaments, there is a significant increase in risk of medical withdrawals directly related to older age divisions, boys, singles matches, and main draw matches. Specifically, there is a significant increase in medical withdrawal rate beyond the fourth match in the tournament regardless of whether it is a main draw, consolation, or singles match.
Clinical Relevance:
Recommendations can be made to exercise caution in tournaments that involve boys, older age divisions, and singles. In addition, there may be sufficient evidence to suggest intervention within a tournament when players play beyond their fourth match.
Keywords: tennis, tournaments, injury rates, risk factors, junior players
Although not well quantified, US junior national tennis tournament players have rigorous tournament schedules, with numerous matches per tournament as well as numerous tournaments per year. Aside from intense practice schedules and the local and sectional tournaments in which competitive junior tennis players participate, there are between 48 to 64 national-level tournaments conducted throughout the year. During each tournament, a junior player can participate in up to 10 matches, depending on his or her progress in the main versus consolation draw and doubles matches. The heavy match volume takes its toll as the tournament progresses, and a relatively high number of these young tennis players not only sustain injury but are unable to compete any further.
Unfortunately, we cannot determine whether injuries sustained in United States Tennis Association (USTA) national tournaments were minor or significant enough to force a player to withdraw or retire from competition. In addition, the relationship to match volume within each tournament has not been determined, thereby making it challenging to formulate recommendations.
In this retrospective cross-sectional study of all 4 USTA supernational junior tournaments during a single year (2005), we investigated the association between medical withdrawals and age, sex, match volume, and match type. We anticipated that junior tennis players would have higher medical withdrawal rates as match volume increased within a tournament. Differences in age, sex, and match type were examined.
Materials and Methods
Before initiating the study, we obtained appropriate approval from the Institutional Review Board at Loyola University Chicago. To use resources most efficiently and to capture the largest volume of matches and athletic exposures, we analyzed match results through the publicly available Internet site for all tournaments (http://www.usta.com). Data were collected from the Web site for the 4 supernational tournaments, resulting in a total of 64 tournaments (boys and girls; age division 12, 14, 16, 18; singles and doubles, main draw and consolation draw). Each player was followed through the tournament in singles and/or doubles. As such, we recorded the division (age/sex), tournament site and location, number of matches in each round, total number of matches, and reason for ending tournament (coded as loss, medical withdrawal, nonmedical reasons). We recorded the total number of main draw matches, consolation matches, singles and doubles matches, and subsequent medical withdrawal rates (per 1000 match exposures).
Any medical reason for withdrawal (injury or illness) that occurred before a scheduled match (walkover) or during a scheduled match (retirement) was considered a medical withdrawal. A player that withdrew in singles would count as a single medical withdrawal unless his or her doubles match resulted in a medical withdrawal. An individual player could have a medical withdrawal in singles as well as doubles, given that they are mutually exclusive exposures. Exposures were counted as 2 for each singles match (ie, 2 players exposed to match) and 4 for each doubles match (ie, 4 players exposed to match).
Statistical Analysis
All data were analyzed using SAS 8 (SAS Institute Inc, Cary, North Carolina). Descriptive statistics were used for sample and tournament characteristics. The incidence of medical withdrawals (walkovers and retirements) was calculated: number of defaults/number of exposures. Relative risks were calculated as the incidence among the exposed versus the unexposed. Multivariate logistic regression analysis was also performed to estimate associations between factors of interest and risk of withdrawal while controlling for potential confounding variables. Statistical significance was defined as P < .05.
Results
A total of 28336 match exposures (14108, male; 14105, female; 123, data unavailable) were analyzed with a similar distribution with respect to age (7056 in 12; 7184 in 14; 7002 in 16; 7094 in 18). The overall medical withdrawal rate was 15.6 per 1000 match exposures. Every factor of interest was significant in predicting a higher rate of medical withdrawal (match volume, age, sex, singles versus doubles, main draw versus consolation). The medical withdrawal rate was 16.9 per 1000 for boys versus 14.0 per 1000 for girls (P < .01) (Figure 1). Medical withdrawals increased as age increased (P < .0001) (Figure 2). In addition, medical withdrawals were significantly higher in consolation matches (28.9/1000) versus main draw matches (8.1/1000; P < .0001) (Figure 3), as well as in singles (17.9/1000) versus doubles (9.8/1000; P < .0001) (Figure 4). The medical withdrawal rate in the first 4 matches of a tournament was 12.7 per 1000, whereas in the fifth match and beyond, it was 26.3 per 1000 (P < .0001) (Figure 5). These results were significant for all main draw matches (Figure 6).
Figure 1.
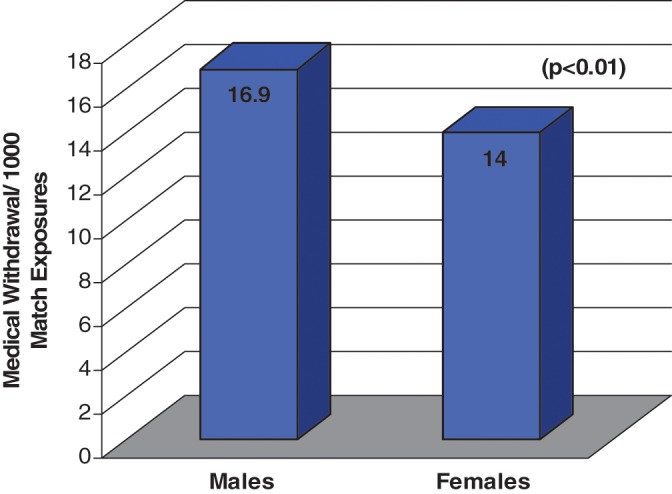
Medical withdrawal incidence of male versus female athletes.
Figure 2.
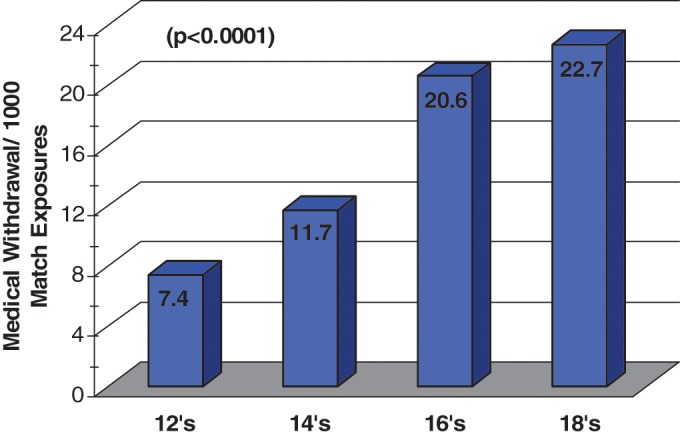
Medical withdrawal incidence by age division.
Figure 3.
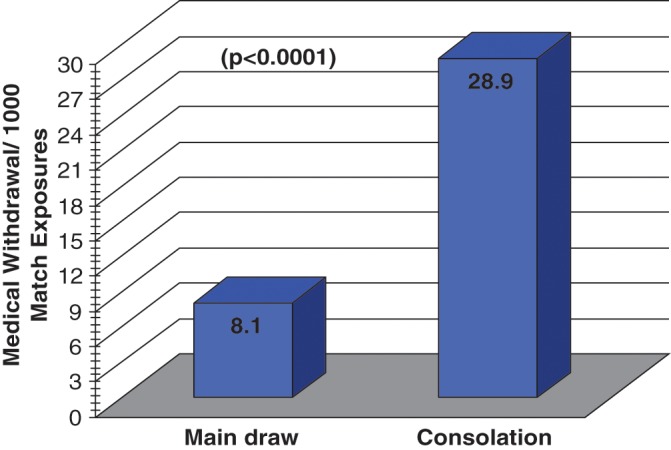
Medical withdrawal incidence of main draw versus consolation matches.
Figure 4.
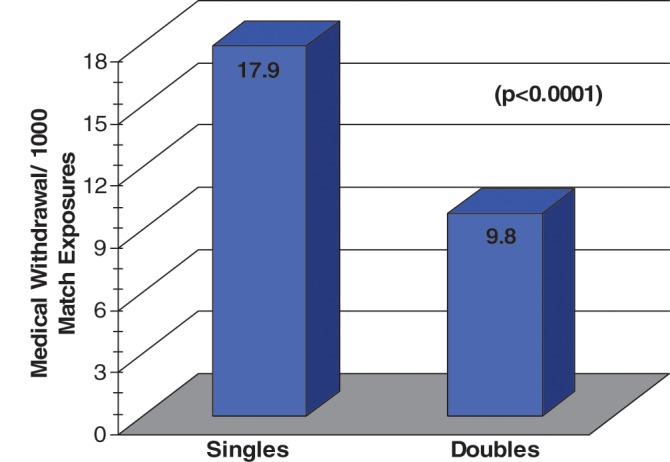
Medical withdrawal incidence of singles versus doubles matches.
Figure 5.
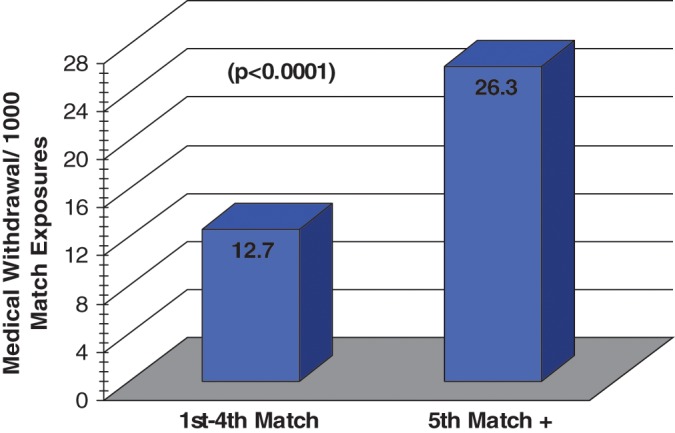
Medical withdrawal incidence of first 4 matches versus fifth match and beyond
Figure 6.
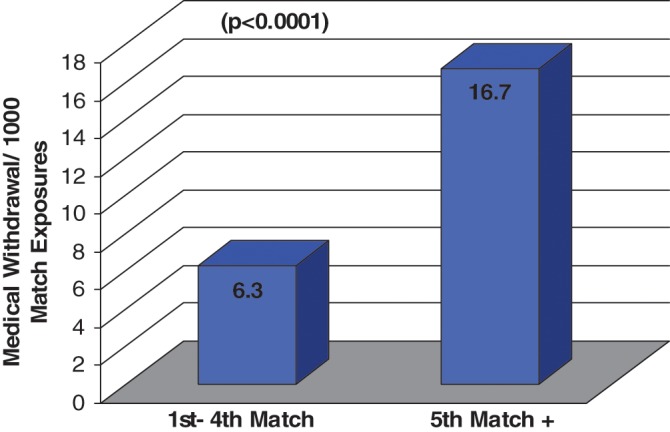
Medical withdrawal incidence in main draw singles: first 4 matches versus fifth match and beyond.
Discussion
This study suggests that numerous factors are related to an increased risk of medical withdrawal in USTA national junior tennis tournaments. Before this study, little evidence was available to indicate whether a specific number of matches increased the risk of injury or medical withdrawal. These data illustrate a statistically higher rate of medical withdrawal after the fourth match in a single tournament (Figures 5 and 6). This includes doubles and consolation matches, which often result in multiple matches played in a single day.
With injury defined as a medical evaluation by an on-site athletic trainer, the incidence and prevalence were 21.5 per 1000 athletic exposures and 21.1 per 100 athletes at the USTA nationals (boys, 16 and 18) over a 6-year period.5 Lower extremity injuries were most common, whereas heat-related issues composed only a minority of these injuries (ie, there were only 11 cases of heat-related illness in 2 years). Safran prospectively followed USTA National Hardcourt Championships (girls and boys, 14 and 16) over a 4-year period.11 He found no difference in the overall rate of injury between boys and girls; however, boys seemed to sustain more new injuries. Overall, girls reported 19.0 injuries per 100 athletes, with boys reporting 18.4 per 100. These numbers corroborate Hutchinson’s prevalence rates5 confirming that musculoskeletal injuries form the majority of injuries. Adult USTA recreational tennis players have injury prevalence rates as high as 52.9 injuries per 100 players, in a population with a mean age of 46.9 years6 (based on self-reported surveys) and where upper extremity injuries predominate.
In this study, the overall rate of medical withdrawal was 15.6 per 1000 athletic exposures, which is similar to the injury rate at the USTA summer nationals5 (boys, 21.5/1000) and USTA spring nationals2 (boys, 19.0/1000; girls, 18.4/1000). The medical withdrawal rates in the older age divisions are strikingly similar in the present study (16, 20.6/1000; 18, 22.7/1000). We would not expect every medical consultation within a tournament to result in a medical withdrawal and, conversely, not every medical withdrawal to result in a medical consultation (ie, it is not required). However, there is a likely underestimation of injuries resulting in medical consultation and an overestimation of medical withdrawals that truly resulted in an injury or illness that required medical consultation. These factors may effectively negate each other and so result in a reasonable approximation of the true medical withdrawal risk when evaluating all matches.
Countries such as Brazil, Denmark, and Australia have prospectively followed a smaller number of elite and junior national players over at least a year to identify injury rates.4,10,12,14 In Brazil, 151 junior national tennis players from age divisions 12 to 18 were prospectively followed for injury trends in 2001. The incidence of injury was lower than that observed in previous studies, with 6.9 treatments per 1000 games (ie, athletic exposures).12 Musculoskeletal injuries were the major cause of athletes’ seeking medical assistance. Winge et al prospectively followed 104 randomly chosen elite Danish tennis players and found an incidence of 2.3 injuries per 1000 tennis hours.14 The majority of injuries were from overuse. The average duration for each injury was longer than expected in this adult population (44.5 days). At the Australian Institute of Sport, 45 elite tennis players aged 16 to 20 years were followed prospectively over a 4-year period. Injury rates were not determined, but 176 injuries occurred.4,10
Medical withdrawal rates are significantly higher in consolation and singles matches (Figures 3 and 4). Junior tennis players may often consider medically withdrawing from a tournament for nonmedical reasons to “save their ranking” or because of disinterest, external pressures, or other uncontrollable personal reasons. With a higher number of medical withdrawals for consolation matches (28.9 versus 8.1, P < .00001), some of these players may have withdrawn for nonmedical or personal reasons.
Main draw and singles matches, especially at supernational tournaments (ie, top tier tournaments), would be unlikely settings for withdrawal based on nonmedical reasons. Medical withdrawal rates for main draw and singles matches indicate a significant increase beyond the fourth match (16.7 versus 6.3 per 1000).
If exposure is a strong predictor of increased risk, then increased caution should be exercised in these populations. Adequate rest periods, especially after completing the fourth match of any kind in these tournaments, may be a reasonable consideration.
Determination of acceptable risk within a sport can be challenging. USA Baseball has made national recommendations regarding sport-specific pitch counts in young players. A subset of youth pitchers (n = 298) of varying ages were prospectively followed for shoulder-related symptoms.8 Age-related recommendations regarding pitch count were established as a result. Subsequent research on the total number of pitches during an entire season was aimed at cumulative risk relating to the volume of pitches and pitch type.7
The NCAA’s (National Collegiate Athletic Association’s) Injury Surveillance System provides data on a number of sports. Softball had the lowest overall injury incidence (including game and practice exposures) at 4.3 injuries per 1000 athletic exposures, whereas baseball had the lowest rate of game injuries at 1.9 per 1000.3 These injury rates are considerably lower than those of many of the previously referenced tennis studies. Contact sports had injury rates similar to those of tennis. NCAA women’s soccer had a game risk of 16.44 injuries per 1000 athletic exposures,2 whereas men’s soccer had a game risk of 18.75 per 1000,1 of which 18% to 23% were considered severe. It appears, however, that injury and medical withdrawal rates in USTA national junior tournaments are higher than those of other overhand noncontact sports, such as baseball and softball, and approach the rates of other intercollegiate contact sports.
Despite the relatively high injury rates reported in some of these studies, there was little information about whether the athlete could play through the injury and continue. The majority of the studies limited their definition of injury to seeking medical assistance during the tournament or year, without a time loss component. The severity of an injury may considerably vary, from a minor nuisance that does not affect performance to more severe trauma requiring withdrawal from a tournament. The ATP World Tour records medical withdrawals in injury statistics during their tournaments.13 Medically withdrawing from a tournament is an important indicator of a player’s inherent risk, as well as an indicator of a player’s willingness to play through injury (which also incorporates important psychological factors).
In addition to the potential legitimacy concern of medical withdrawals in our study, there were other limitations. Injury or illness type was not available, thus making severity judgements impossible. The cumulative number of tournament matches per year, practice and training patterns, and even participation in other sports was unknown. Weather conditions, heat, and hydration status were also not available. The retrospective nature of the data collection was another limiting factor, but it was not practical to prospectively analyze 64 tournaments throughout the country. However, with a prospective analysis, the outcome of a medical withdrawal would not have likely been altered in this study.
Conclusion
The risk of medical withdrawal in USTA national junior tournaments is significantly increased in matches involving older age divisions, boys, singles, and consolation matches. There is a significant increase in risk of medical withdrawal beyond the fourth match played within a tournament. Tournament organizers should exercise caution when scheduling tournaments and so consider allocating an appropriate rest period for players after completion of the fourth match.

Footnotes
No potential conflict of interest declared.
References
- 1. Agel J, Evans T, Dick R, Putukian M, Marshall SW. Descriptive epidemiology of collegiate men’s soccer injuries: National Collegiate Athletic Association Injury Surveillance System, 1988-1989 through 2002-2003. J Athl Train. 2007;42:270-277 [PMC free article] [PubMed] [Google Scholar]
- 2. Dick R, Putukian M, Agel J, Evans TA, Marshall SW. Descriptive epidemiology of collegiate woman’s soccer injuries: National Collegiate Athletic Association Injury Surveillance System, 1988-1989 through 2002-2003. J Athl Train. 2007;42:278-285 [PMC free article] [PubMed] [Google Scholar]
- 3. Dick R, Sauers E, Agel J, et al. Descriptive epidemiology of collegiate men’s baseball injuries: National Collegiate Athletic Association Injury Surveillance System, 1988-1989 through 2003-2004. J Athl Train. 2007;42:183-193 [PMC free article] [PubMed] [Google Scholar]
- 4. Fricker P, Maguire K. The prevalence of leg injuries in elite tennis players. Excel. 1986;3(2):2-5 [Google Scholar]
- 5. Hutchinson MR, Laprade RF, Quinter MB, II, Moss R, Terpstra J. Injury surveillance at the USTA boys’ tennis championships: a 6-yr study. Med Sci Sports Exerc. 1994;27:826-830 [PubMed] [Google Scholar]
- 6. Jayanthi N, Sallay PI, Hunker P, Przybylski M. Skill-level related injuries in recreational competition tennis players. Med Sci Tennis. 2005;10(1): 12-15 [Google Scholar]
- 7. Lyman D, Fleisig G, Andrews J, Osinski DE. Effect of pitch type, pitch count, and pitching mechanics on risk of elbow and shoulder pain in youth baseball pitchers. Am J Sports Med. 2002;30:463-468 [DOI] [PubMed] [Google Scholar]
- 8. Lyman S, Fleisig GS, Waterbor JW, et al. Longitudinal study of elbow and shoulder pain in youth baseball pitchers. Med Sci Sports Exerc. 2001;33:1803-1810 [DOI] [PubMed] [Google Scholar]
- 9. Marshall SW, Hamstra-Wright KL, Dick R, Grove KA, Angel JA. Descriptive epidemiology of collegiate woman’s softball injuries: National Collegiate Athletic Association Injury Surveillance System, 1988-1989 through 2003-2004. J Athl Train. 2007;42:286-294 [PMC free article] [PubMed] [Google Scholar]
- 10. Reece LA, Fricker PA, Maguire KF. Injuries to elite young tennis players at the Australian institute of sport. Aust J Sci Med Sport. 1986;18(4):11-15 [Google Scholar]
- 11. Safran MR. Tennis injuries and strategies for prevention: gender differences in the American junior elite tennis player. Med Sci Tennis. 2000;5(2). http://www.stms.nl Accessed January 8, 2009 [Google Scholar]
- 12. Silva RT, Berra B, Cohen M, Matsumoto MH. Medical assistance at the Brazilian junior tennis circuit-a one-year prospective study. J Sci Med Sport. 2003;6(1):14-18 [DOI] [PubMed] [Google Scholar]
- 13. Spreen D. Injury statistics and trends of ATP players. Med Sci Tennis. 2001;6(1). http://www.stms.nl Accessed January 8, 2009 [Google Scholar]
- 14. Winge S, Jergensen U, Neilsen L. Epidemiology of injuries in Danish championship tennis. Int J of Sports Med. 1989;10:368-371 [DOI] [PubMed] [Google Scholar]