

Abstract
Objective:
Maternal mortality is a major public health problem in low-income countries, such as Bangladesh. Women's empowerment in relation to enhanced utilization of delivery care is underexplored. This study investigates the associations between women's economic empowerment and their utilization of maternal health care services in Bangladesh.
Methods:
In total, 4925 women (15–49 years of age) with at least one child from whole Bangladesh constituted the study sample. Home delivery without skilled birth attendant and use of institutional delivery services were the main outcome variables used for the analyses. Economic empowerment, neighborhood socioeconomic status, household economic status, and demographic factors were considered as explanatory variables. The chi square test and unadjusted and adjusted logistic regression analyses were applied at the collected data.
Results:
In the adjusted model, respondent's and husband's education, household economic status, and residency emerged as important predictors for utilization of delivery care services. In the unadjusted model, economically empowered working and microfinanced women displayed more home delivery.
Conclusion:
The current study shows that use of delivery care services is associated with socioeconomic development and can be enhanced by societies that focus on general issues such as schooling, economic wellbeing, and gender-based discrimination.
Keywords: Empowerment, home delivery, maternal mortality, neighborhood socioeconomic status
INTRODUCTION
Every year more than half a million women die from preventable complications caused by childbirth or from pregnancy-related issues. The large majority (99%) of these maternal deaths occur in low-income countries.[1,2] In Bangladesh, with a population among the poorest in the world, maternal mortality, as well as associated maternal morbidity, is a serious public health concern. Currently, the maternal mortality ratio is one per 350 births.[3] Along with the United Nations, the government of Bangladesh is committed to achieving the Millennium Development Goal (MDG) 5, i.e., to reduce the maternal mortality ratio by 75% between 1990 and 2015.[4]
Circumstances acquiescent to intervention by skilled health providers are engaged in the casual mechanisms for about 80% of maternal deaths, and currently, the main strategy for reducing maternal mortality has been to scale up access to delivery care during the time of delivery.[1] While skilled birth attendance and emergency obstetric care are essential to securing significant reductions in maternal mortality, health service extension by itself is not sufficient. In most home deliveries in Bangladesh, such services are not utilized.[5,6] The reasons for this under-utilization have not been satisfactorily investigated. The relationships between economic empowerment and improved health status in terms of child mortality, nutrition, immunization coverage, and contraceptive use have been documented in Bangladesh.[7–10] However, women's economic situation and utilization of child delivery care services is a salient problem that has received less attention.
Present evidence suggests that the available maternal health services are not utilized appropriately in regions where the need for such services is most prevalent, such as areas with deprived populations.[11] Due to gender inequalities, women in poor populations often discover themselves even further disadvantaged within the deprived population, as a result of being the poorest among the poor and the least educated within the insufficiently educated.[12] However, economic empowerment of women in relation to health care utilization is not well explored. The aim of the study is to investigate the associations between women's economic empowerment and their utilization of maternal health services in Bangladesh.
METHODS
The study was based on a cross-sectional design, implemented in Bangladesh through a nationally representative household survey during January–August 2007. Data were collected from 10,996 women aged 15–49 surveyed from 10,400 households through a nationally representative household survey using a structured questionnaire.
The survey involved multistage cluster sampling and was based on the 2001 population census enumeration areas (EAs) with population and household information. EAs were used as primary sampling units (PSUs) for the whole survey. Each PSU had 100 households with locational maps and geographical boundaries. In total, 361 PSUs (227 in rural areas and 134 in urban areas) were randomly selected from the six divisions – Barisal, Chittagong, Dhaka, Khulna, Rajshahi, and Sylhet.
During January to March 2007, a household listing operation was carried out in all PSUs before the main survey, and the resulting lists of households served as the sampling frame for the selection of households in the second stage.
In the next stage, 30 households were selected from each PSU, using an equal probability systematic sampling technique in relation to the 2001 population census. Finally, 10,819 households were initially selected from the sample clusters for the survey.
All ever-married women of reproductive age (15–49 years) who slept in the chosen households the night before the survey were eligible to participate in the survey. At the next stage 10,400 households were occupied and selected for the study. From these selected households, 11,178 eligible women aged 15–49 years were identified and 10,996 were interviewed with a response rate of 98%.
Women with a history of delivery of at least one child were included in the current study (N = 4925) constituting 45% of the total 10,996 women respondents of the whole survey.
Description of the variables of interest
Dependent variable
The utilization of health facilities during the last delivery was assessed by the place of delivery: delivery at home mainly without utilizing the delivery care services and delivery at health care facilities. For this study, health facilities include government hospitals, private hospitals/clinics, NGOs, and other health facilities.
Independent variables
The variables were age (groups divided in to seven categories 15–19, 20–24, 25–29, 30–34, 35–39, 40–44, and 45–49), residency (urban or rural), the level of education of the women and the partner (no education, primary education, secondary education, and higher education), religion (Muslim or non-Muslim), and divisional residence within Bangladesh (Dhaka, Barisal, Sylhet, Rajshahi, Chittagong, and Khulna).
In patriarchal societies like Bangladesh, sex of the household head is important as it often decides the kind of health care the house members receive. Therefore, the current study also considered sex of household head.
Economic status of the respondents was defined in five quintiles: poorest, poorer, middle, richer, and richest. The economic status of the respondents were measured based on the wealth index. Wealth index is a widely used measurement of economic status used to ascertain the equity of health programs in publicly or privately provided services. The main objectives of wealth index are to measure ability to pay for health services and the distribution of services among the poor. Wealth index was validated and used in several demographic and health surveys in different countries.[13–15] The wealth index is a composite measure of the cumulative living standard of a household. It is calculated by using data on a household's ownership of selected assets, e.g., radio, televisions, and bicycles, materials used for construction of house, types of water-access, and use of sanitation facilities. Wealth index uses a generated statistical procedure known as the principal components analysis and places individual households on a continuous scale of relative wealth. The scale is standardized in relation to a standard normal distribution with a mean of zero and a standard deviation of one. These standardized scores are then used to create the groups that define wealth quintiles as: poorest, poorer, middle, richer, and richest. The wealth index used in Bangladesh was introduced by Rutstein and Johnson (2004) and includes any item that may reflect economic status, specifically most household assets and utility services, including country-specific items.[16]
Neighborhood socioeconomic (NSE) status was measured by whether the respondent lived in a less or more disadvantaged socioeconomic neighborhood. The NSE index comprised four variables: proportion of respondents living in rural areas, proportion of respondents living in slum areas, proportion of respondents living below the poverty level (below the 20% quintile), and the proportion of respondents who are uneducated. This methodology has been used by many others studying the effect of neighborhood socioeconomic status on health.[15,17] The scores generated from the continuous index were used to classified neighborhoods into two categories: (i) more disadvantaged and (ii) less disadvantaged socioeconomic neighborhood status.
Economic empowerment indicators assessed included respondent's working status, employment status, association with any microfinance program, and decision making on spending money.[13] Working status was assessed by whether the respondent was employed or not. Association with microfinance program was assessed by whether the respondents had a microfinance loan or not. Employment status had three alternatives: whether respondent worked year around, worked seasonally, or worked occasionally. Seasonal work is say for example paddy filed work during monsoon season to cultivate rice. To assess the decision-making ability of the respondent in the household, respondents were asked who decides how to spend money. The alternatives were respondent alone, shared with husband and other member of the household.
Ethical issues
The survey procedure (e.g., organization and sampling methods) and instruments used in the study received ethical permission from the Institutional Review Board of ORC Macro Inc, who provided the main scientific support for the whole survey. The permission to use these data was obtained from Measure Demographic and Health Survey, the legal owner of the survey data under the main donor agency, USAID through proper project applications.
This study is based on an analysis of existing survey data with all information that could be used to identify the respondents being removed. The field interviewers for the survey obtained informed consent from the respondents in this study and all questions were asked in close confidentiality. The respondents had the autonomy to leave the study at any stage.
Ethical recommendations: The study has received ethical permission from the Institutional Review Board of ORC Macro Inc.
Statistical analysis
Descriptive statistics were used to display differences in proportions of home delivery between population strata. Unadjusted logistic regressions were thereafter used to assess the independent contribution of demographics (individual and family level) and economic variables (individual and group level) in predicting home delivery. For assessing confounding effects, multivariate logistic regression analysis was employed in the adjusted model. The magnitude and direction of association were expressed through odds ratios and significant levels expressed as P values. Statistical significance was considered at P < 0.05. The SPSS version 18.0 was used for all analyses.
RESULTS
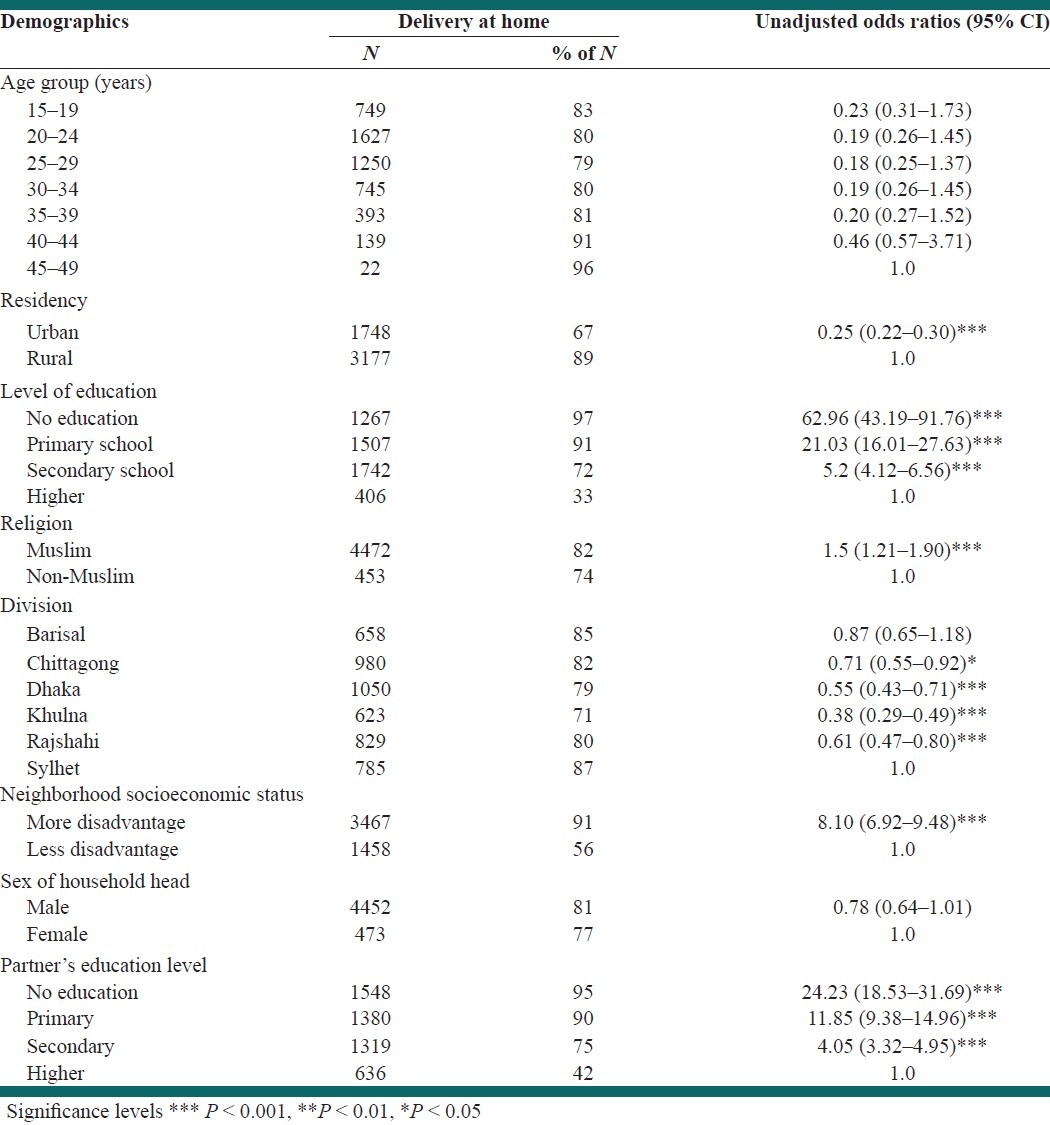
In general 81% women deliver at home without help of any health care services, even without help of trained birth attendant. More than half of the women (62%) resided at rural areas and one out of three were uneducated (32%). Ninety percent of the respondents were Muslims.
The majority (97%) of women without formal education reported home delivery, while the proportion among women with higher education was only about one out of three women (33%). Women living in rural areas (OR 0.25, CI 0.22–0.30) displayed higher likelihood of home delivery than women living in urban areas. Also, women from the Khulna division, of non-Muslim religion, and from less disadvantaged neighborhoods demonstrated lower proportions of home delivery [Table 1]. Muslim women were more likely (OR 1.5, CI 1.21–1.90) to deliver at home compared to non-Muslim women. Women from more disadvantage areas were eight times more likely to deliver at home compared to less disadvantaged areas.
Table 1.
Proportions of women having chosen home delivery without utilizing delivery care displayed by demographic characteristics. Differences in distribution are expressed as unadjusted odds ratios
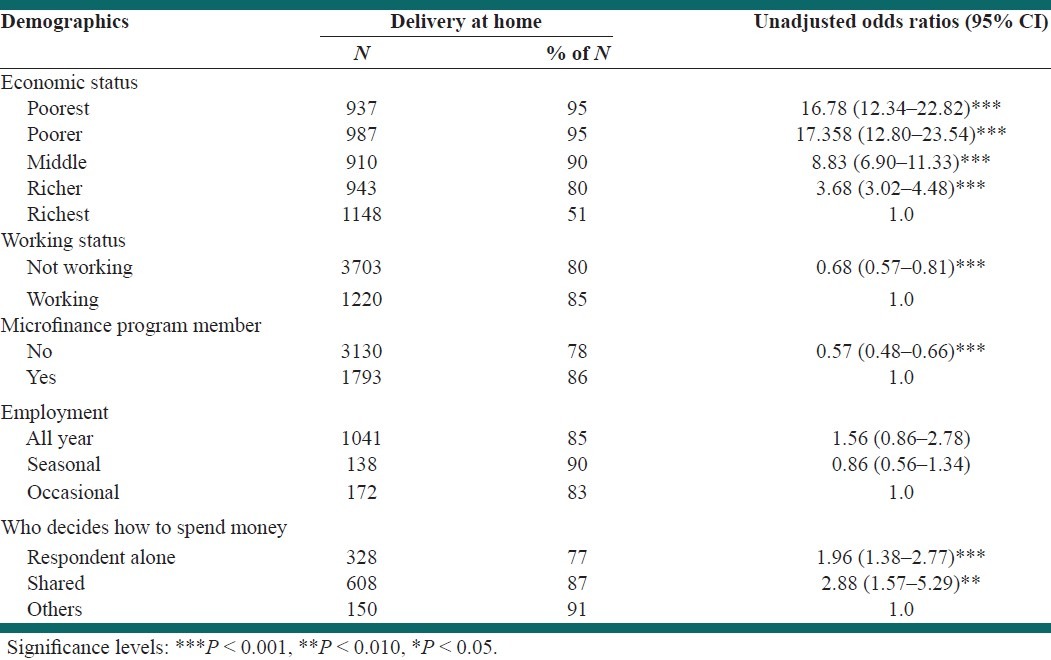
Economic characteristics
A high proportion of home delivery was reported by the poorest women (95%), while the proportion of home delivery among the richest group was about one out of two women (51%). For both working and nonworking women, proportions of home delivery were high (85% and 80%, respectively). Women belonging to microfinance programs displayed a lower proportion of home delivery than those not associated with such programs. Finally, women who decided how to spend money had a lower proportion of home deliveries than women without any decision-making power regarding family finances [Table 2].
Table 2.
Proportions of women having chosen home delivery without utilizing delivery care displayed by economic characteristics. Differences in distribution are expressed as unadjusted odds ratios
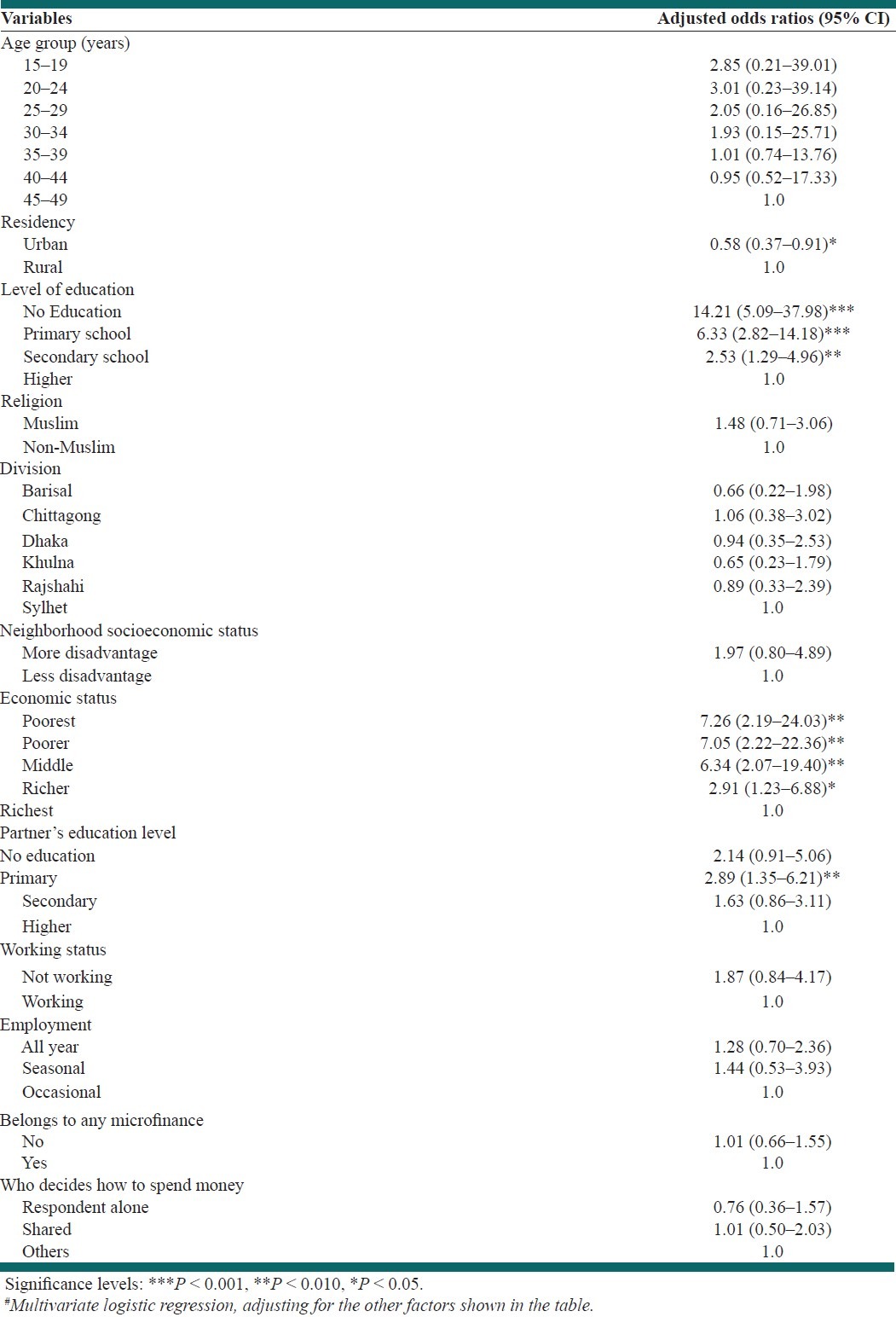
Adjusted relative risks
In the adjusted model, the respondent's residency, education, economic status, and husband's education emerged as strong predictors of delivery care utilization. However, the economic empowerment variables were not significantly associated to utilization of delivery care facilities in the adjusted model [Table 3].
Table 3.
Adjusted# odds ratios (OR) and 95% confidence intervals of reporting home delivery without utilizing delivery care by individual, family level, and economic empowerment factors
DISCUSSION
The current study shows a consistently strong relationship between the type of delivery and the education of both the respondent and her partner, their residency, and economic status of the family. Economic empowerment showed no association with the delivery type when all other variables are adjusted. There is a lack of studies exploring the association between women's economic empowerment and the use of reproductive health services. While a study in Nairobi, Kenya, revealed household wealth and the mother's education as strong correlates for place of delivery, the relationship with women's autonomy was relatively weaker.[18] The current study revealed that uneducated women delivered at home three times more (97%) than their higher educated peers (33%). Also women below poverty line delivered at home almost two times more (95%) than their richest peers (51%). Compared to the efforts made to improve the quality of and access to health care services, the role of socioeconomic position of women on maternal health has gained less attention. Studies have shown that women's educational achievement, socioeconomic status, household economic status, and decision-making ability are linked with care seeking behavior for maternal health care and thus a reduction in maternal mortality.[12,19,20]
The analysis of the current study supports Hart's inverse care law.[21] The law states that the more disadvantaged a population is, the less likely they are to have access health services. Our findings in the unadjusted model support this law as women from lower economic status and from more disadvantage areas used less delivery care services. In order to better achieve the fifth MDG, it is worth providing basic maternal health care services. However, it must be noted that these services need to address and include current and future poverty-reducing policies.[22]
Economic empowered (working and microfinanced) women are more likely to deliver at home as indicated by bivariate and unadjusted logistic regression analyses. Therefore, the findings surprisingly indicated an inverse relation between economic empowerment and utilization of delivery care facilities. However, once confounding socioeconomic effects are included in the model, that inverse relation no longer remained. Family economic status is more significant in the analysis. Therefore, rather than individual empowerment, family level up-liftmen for economic status is more important.
It is logical to expect that an extension of high-quality maternal health services may raise women's enthusiasm to use these services.[23] If so, women with higher education, independence in decision-making and right to use to economic resources, are more likely to handle successfully with the challenges exist in maternal health systems.
The United Nations’ MDG 3 is to promote gender equality and empower women.[12] The empowerment of women is inevitably linked with education, employment, and mobility.[24] Women with economic power have better control over their own lives and can directly take part in decision making in the household. By ignoring the importance of economic empowerment of women, it will be more difficult to achieve gender equality, eliminate poverty, and access to health care overall the UN's mentioned Millennium Development Goals.[25]
The current study demonstrated that Muslim women were more likely to have home deliveries, which is due to misconceptions regarding religion.[26] In rural Bangladesh, many religious leaders believe that a Muslim woman should not be allowed to seen by a male other than her husband, her father, and close relatives. This belief can result in seeking less reproductive care for the pregnant household member.[27]
In summary, the findings of the current study show that a considerable increase in the use of maternal health services during delivery can be accomplished by extending socioeconomic development and by focusing on issues such as schooling, economic wellbeing, and gender-based discrimination. We assume from the study findings that better systemic benefits can be gained in maternal delivery care with improvisation in socioeconomic status. These benefits are preventive in nature, receiving maternal delivery care, and thus, lessening the risk of maternal delivery complications and death. The government of Bangladesh is committed to achieving the fifth Millennium Development Goal, to reduce the maternal mortality ratio by 75% between 1990 and 2015. To achieve the target of MDG 5, the Bangladeshi government will need not only to address and expand maternal health services, but at the same time it needs to focus programs on poverty eradication (MDG 1), universal primary education (MDG 2), and empowerment of women (MDG 3).
Gender inequality, low social status, and disempowerment of women have a major impact on their health, maternal health, and overall access to maternal health care services.[28] A study in Bangladesh showed that the probability of seeking any type of health care was almost twice as high among men than women.[29] In Bangladesh, often childbirth is considered a concern for the women, not the men. Women may find it difficult to get the money to pay for health care services or to obtain transportation to get to medical care. Often access to preventative and curative care by most women is low; women are economically dependent on their husbands who may be unwilling to pay for care.[30]
Women who can themselves handle their microfinance loans and themselves make contributions to their family's income may experience greater levels of empowerment than women who do not control their own finances.[7] At the same time, women are empowered when they make money themselves, and when they are able to decide how to spend the earned money.[10] Paid employment empowers poor women in different areas of their lives, influencing sexual and reproductive health preferences, decision-making ability, education, and healthy behavior. Approximately, 600,000 women worldwide die each year due to a lack of emergency obstetric care and access to skilled birth attendants.[12] Yanda et al. stated that poor women have more maternal mortality and morbidity and suffer from continuous violence due to lack of access to adequate reproductive health services.[31] The current study supports the findings from another low-income country setting. However, the current findings in Bangladesh demonstrate that education and economic status of the family are more important elements for utilizing delivery care. Researchers have emphasized the need to narrow the gaps between practice and policy in order to achieve reduced maternal mortality.[32,33] The current study has provided some important practical information for the policy makers. The policy makers should emphasize on family-level economic up-liftment as well as education program. Microfinance firms can also initiate social responsibilities by emphasizing utilizing delivery care services beside their money lending program.
The current study is a cross-sectional study. Therefore, assigning causality is problem which warrants a longitudinal study. The study has considered only delivery of last child. The situations for deliveries of other children are unknown. At the same time, the study can recommend for a qualitative study to better understand the empowerment and delivery care utilization.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Ronsmans C, Graham WJ. Maternal Mortality: Who, When, Where, and Why. Lancet. 2006;368:1189–200. doi: 10.1016/S0140-6736(06)69380-X. [DOI] [PubMed] [Google Scholar]
- 2.Campbell OM, Graham WJ. Strategies for reducing maternal mortality: Getting on with what works. Lancet. 2006;368:1284–99. doi: 10.1016/S0140-6736(06)69381-1. [DOI] [PubMed] [Google Scholar]
- 3.Bangladesh, Statistics. UNICEF. 2010. [Last cited on 2011 Jul 07]. Available from: http://www.unicef.org/infobycountry/bangladesh_bangladesh_statistics.html .
- 4.Bangladesh, UNDP. 2010. [Last cited on 2011 Jul 07]. Available from: http://www.undp.org.bd/mdgs.php .
- 5.Dhaka, Bangladesh and Calverton, Maryland, USA: National Institute of Population Research and Training, Mitra and Associates, and Macro International; 2007. Bangladesh Demographic and Health Survey. [Google Scholar]
- 6.Andrews JY, Dalal K. Umbilical cord-cutting practices and place of delivery in Bangladesh. Int J Gynaecol Obstet. 2011;114:43–6. doi: 10.1016/j.ijgo.2011.01.025. [DOI] [PubMed] [Google Scholar]
- 7.Hashemi SM, Schuler SR, Riley AP. Rural credit programmes and women's empowerment in Bangladesh. World Dev. 1996;24:635–53. [Google Scholar]
- 8.Khandker SR. Fighting Poverty With Microcredit: Experience in Bangladesh. New York, NY: Oxford University Press; 1988. [Google Scholar]
- 9.Schuler SR, Hashemi SM. Credit programmes women's empowerment and contraceptive use in rural Bangladesh. Stud Fam Plan. 1994;25:65–76. [PubMed] [Google Scholar]
- 10.Schuler S, Hashemi S, Riley A. The influence of women's changing roles and status in Bangladesh's fertility transition: Evidence from a study of credit programmes and contraceptive use. World Dev. 1997;25:563–75. [Google Scholar]
- 11.Sarin AR. Underutilization of maternal health services. World Health Forum. 1997;18:67–8. [PubMed] [Google Scholar]
- 12.Kaur A. Women's Economic Empowerment: Meeting the Needs of Impoverished Women. New York: UNFPA; 2007. [Google Scholar]
- 13.Dalal K. Does economic empowerment protect women from intimate partner violence? J Inj Violence Res. 2011;3:35–44. doi: 10.5249/jivr.v3i1.76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Dalal K, Dawad S. Non-utilization of public health care facilities: Examining the reasons through a national study of women in India. Rural Remote Health. 2009;9:1178. [PubMed] [Google Scholar]
- 15.Aremu O, Lawoko S, Dalal K. Neighborhood socioeconomic disadvantage, individual wealth status and patterns of delivery care utilization in Nigeria: A multilevel discrete choice analysis. Int J Womens Health. 2011;3:167–74. doi: 10.2147/IJWH.S21783. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Rutstein SO, Johnson K. DHS Comparative Reports no. 6. Calverton, MD: ORC Macro; 2004. The DHS wealth index. [Google Scholar]
- 17.Wight RG, Cummings JR, Miller-Martinez D, Karlamangla AS, Seeman TE, Aneshensel CS. A multilevel analysis of urban neighborhood socioeconomic disadvantage and health in late life. Soc Sci Med. 2008;66:862–72. doi: 10.1016/j.socscimed.2007.11.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Fotso JC, Ezeh AC, Essendi H. Maternal health in resource-poor urban settings: How does women's autonomy influence the utilization of obstetric care services? Reprod Health. 2009;16:6–9. doi: 10.1186/1742-4755-6-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Chowdhury ME, Ronsmans C, Killewo J, Anwar I, Gausia K, Das-Gupta S, et al. Equity in use of home-based or facility-based skilled obstetric care in rural Bangladesh: An observational study. Lancet. 2006;367:327–32. doi: 10.1016/S0140-6736(06)68070-7. [DOI] [PubMed] [Google Scholar]
- 20.Al RA, Afifi M, Mabry RM. Women's autonomy, education and employment in Oman and their influence on contraceptive use. Reprod Health Matters. 2004;12:144–54. doi: 10.1016/s0968-8080(04)23113-5. [DOI] [PubMed] [Google Scholar]
- 21.Hart JT. The inverse care law. Lancet. 1971;1:405–12. doi: 10.1016/s0140-6736(71)92410-x. [DOI] [PubMed] [Google Scholar]
- 22.Gwatkin DR. How much would poor people gain from faster progress towards the Millennium Development Goals for health? Lancet. 2005;365:813–7. doi: 10.1016/S0140-6736(05)17992-6. [DOI] [PubMed] [Google Scholar]
- 23.Rahman MH, Mosley WH, Ahmed S, Akhter HH. Does service accessibility reduce socioeconomic differentials in maternity care seeking? Evidence from rural Bangladesh. J Biosoc Sci. 2008;40:19–33. doi: 10.1017/S0021932007002258. [DOI] [PubMed] [Google Scholar]
- 24.Paruzzolo S, Mehra R, Kes A, Ashbaugh C. Targeting poverty and gender inequality to improve maternal health Solutions for girls and women, 2nd Global Conference. Washington, DC: Women deliver; 2010. [Google Scholar]
- 25.Negash A. Economic empowerment of women, Markkula Center for Applied Ethics. California: Santa Clara University; 2006. [Google Scholar]
- 26.Gyimah SO, Takyi BK, Addai I. Challenges to the reproductive-health needs of African women: On religion and maternal health utilization in Ghana. Soc Sci Med. 2006;62:2930–44. doi: 10.1016/j.socscimed.2005.11.034. [DOI] [PubMed] [Google Scholar]
- 27.Hosssain MI. HEDG working paper 10/08. York, UK: University of York; 2010. Inequality in the Utilization of Maternal Care and the Impact of a Macroeconomic Policy: Evidence from Bangladesh. [Google Scholar]
- 28.Shen C, Williamson JB. Maternal mortality, women's status, and economic dependency in less developed countries: A cross-national analysis. Soc Sci Med. 1999;49:197–214. doi: 10.1016/s0277-9536(99)00112-4. [DOI] [PubMed] [Google Scholar]
- 29.Ahmed SM, Adams AM, Chowdhury M, Bhuiya A. Gender, socioeconomic development and health-seeking behavior in Bangladesh. Soc Sci Med. 2000;51:361–71. doi: 10.1016/s0277-9536(99)00461-x. [DOI] [PubMed] [Google Scholar]
- 30.Schuler SR, Bates LM, Islam MDK. ‘Paying for reproductive health services in Bangladesh: Intersections between cost, quality and culture’. Health Policy Plan. 2002;17:273–80. doi: 10.1093/heapol/17.3.273. [DOI] [PubMed] [Google Scholar]
- 31.Yanda K, Smith SV, Rosenfield A. Reproductive Health and Human Rights’. Int J Gynaecol Obstet. 2003;82:275–83. doi: 10.1016/s0020-7292(03)00226-1. [DOI] [PubMed] [Google Scholar]
- 32.Zolala F, Haghdoost AA. A gap between policy and practice: A case study on materal mortality reports, Kerman, Iran. Int J Prev Med. 2011;2:88–93. [PMC free article] [PubMed] [Google Scholar]
- 33.Aremu O, Lawoko S, Dalal K. The influence of individual and contextual socioeconomic status on obstetric care utilization in the democratic republic of Congo: A Population-based Study. Int J Prev Med. 2012;3:278–85. [PMC free article] [PubMed] [Google Scholar]