

To the Editor: Cutaneous leukemia typically presents as solitary or multiple papules, nodules or plaques.1,2 We report a patient with an atypical presentation of leukemia cutis as localized lip ulcers. To our knowledge, this is the first report of leukemia cutis presenting solely as ulcerative leukemia labialis. This unusual presentation led to a delay in diagnosis, and dermatologists should be aware of the possibility of isolated lip leukemic infiltration.
A 52-year-old African American women with a past medical history of recurrent non-M3 acute myeloid leukemia (AML), status post allogenic stem cell transplant 7 months previously, presented with severe left lower quadrant abdominal pain and vomiting. During her hospitalization she developed painful, swollen lips, and dermatology was consulted to evaluate lesions on the upper and lower lips.
On physical examination, she was found to have grossly enlarged lips with multiple areas of crusted hemorrhagic ulceration (Figure 1). No similar lesions were present elsewhere in the oral cavity or on comprehensive cutaneous examination. The initial clinical differential diagnosis included mucocutaneous herpes simplex virus (HSV), cytomegalovirus, Sweet’s syndrome, leukemia cutis, or an atypical presentation of a viral, bacterial, or fungal infection.
Fig 1.

Leukemia Labialis. Symmetric lip swelling and hemorrhagic ulceration on upper and lower lips.
The patient was treated empirically with acyclovir, and direct fluorescent antigen (DFA) analysis for HSV and viral cultures were performed. DFA and viral cultures were negative, and the patient’s symptoms had not improved. Her treatment was changed to a trial of foscarnet to cover potentially resistant strains of HSV. As ulcers failed to resolve and patient complained of persistent pain, a 4mm punch biopsy of the upper lip was performed. Histopathologic examination revealed ulcerated and hemorrhagic skin with focally dense, interstitial infiltrates of large mononuclear cells with oval nuclei, vesicular chromatin, prominent nucleoli, and scant cytoplasm, morphologically consistent with blasts. These findings were confirmed by diffuse myeloperoxidase immunohistochemical staining of the infiltrate, mirroring the original immunophenotype of the patient’s leukemia. GMS and gram stains were negative for fungal and bacterial organisms, and no viral cytopathic changes were seen (Figure 2).
Fig 2.
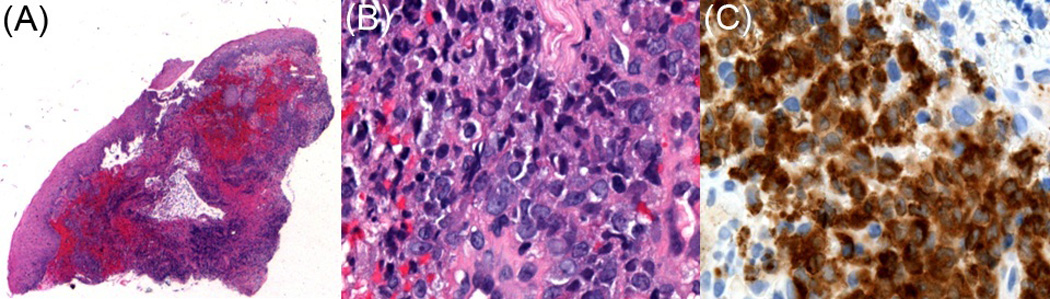
A, Leukemia Labialis. Low magnification view of punch biopsy (25x, Hematoxylin-eosin stain). B, Atypical mononuclear cells consistent with blasts (400x, Hematoxylin-eosin stain). C, Myeloperoxidase immunohistochemical staining is diffusely positive in the blast population.
The patient’s presentation of swollen and ulcerated lips was interpreted as cutaneous involvement of her recurrent AML consistent with limited leukemia cutis localized to the lips. Total body skin examination failed to reveal any other cutaneous or subcutaneous lesions. Radiation therapy was instituted for symptomatic relief.
Leukemia cutis can occur in all forms of leukemia. Clinical features are variable and include solitary or multiple reddish to violaceous papules, plaques and nodules, generalized maculopapular eruptions.1, 2 This case report demonstrates that it is important to consider atypical presentations of leukemia cutis. In addition to the morphologic forms of orofacial leukemia cutis mentioned in the literature3,4,5, ulcerative leukemia labialis should be added to the catalog of clinical manifestations of facial lesions in patients with acute myeloid leukemia. In an immunocompromised patient it is critical to distinguish leukemia cutis from other ulcerative skin diseases such as acute herpes simplex, bacterial infection, or neutrophilic dermatoses.
Acknowledgments
Funding sources: This vignette has no funding support.
ABBREVIATIONS AND ACRONYM LIST
- AML
acute myelogenous leukemia
- HSV
herpes simplex virus
- DFA
direct fluorescent antigen
Footnotes
Conflicts of interest: None declared.
This case was accepted for poster presentation at the American Society of Dermatopathology (ASDP) Annual Meeting 2011.
Contributor Information
C Obi, Email: chrystal.obi@gmail.com.
P Holler, Email: phillip.holler@uphs.upenn.edu.
D Pugliese, Email: douglas.pugliese@uphs.upenn.edu.
R Abraham, Email: ronnie.braham@uphs.upenn.edu.
X Xu, Email: xug@mail.med.upenn.edu.
J Sobanko, Email: joseph.sobanko@uphs.upenn.edu.
M Rosenbach, Email: misha.rosenbach@uphs.upenn.edu.
REFERENCES
- 1.Kaddu S, Zenahlik P, Beham-Schmid C, Kerl H, Cerroni L. Specific cutaneous infiltrates in patients with myelogenous leukemia: A clinicopathologic study of 26 patients with assessment of diagnostic criteria. J Am Acad Dermatol. 1999;40:996–978. doi: 10.1016/s0190-9622(99)70086-1. [DOI] [PubMed] [Google Scholar]
- 2.Watson KMT, Mufti G, du Vivier AWP, Creamer D. Spectrum of clinical presentation, treatment and prognosis in a series of eight patients with leukemia cutis. Clinical and Experimental Dermatology. 2006;31:218–221. doi: 10.1111/j.1365-2230.2005.02022.x. [DOI] [PubMed] [Google Scholar]
- 3.Weckx LLM, Hidal LBT, Marucci G. Oral manifestations of leukemia. Ear Nose Throat J. 1990;69:345–346. [PubMed] [Google Scholar]
- 4.Aguilera S, Zarraga M, Rosen L. Leukemia Cutis in a Patient With Acute Myelogenous Leukemia: A Case Report and Review of the Literature. Cutis. 2010;85:31–36. [PubMed] [Google Scholar]
- 5.Baer M, Barcos M, Farrell H, Raza A, Preisler HD. Acute Myelogenous Leukemia with Leukemia Cutis: Eighteen Cases Seen Between 1969 and 1986. Cancer. 1989;63:2192–2200. doi: 10.1002/1097-0142(19890601)63:11<2192::aid-cncr2820631122>3.0.co;2-r. [DOI] [PubMed] [Google Scholar]