

Abstract
Stroke is an important disease, because it is usually devastating and often fatal. Left atrial appendage (LAA) thrombi are well known as a cause for cerebral infarction, but pulmonary vein thrombi remain unknown. To detect LAA thrombi, transoesophageal echocardiography (TOE) is usually used. More recently, a 64-slice multidetector CT (64-MDCT) has proved to be an option for identifying them. The patient was 77-year-old male, and had a lacuna infarction in pons. A 64-MDCT demonstrated a 3 to 4 mm thrombus at the proximal side of right upper pulmonary vein. After 2 months warfarin therapy, the thrombus disappeared. When assessing the possible cause for cerebral infarction, it is important to identify thrombi within the LAA, and in the left pulmonary vein. 64-MDCT seems to be more suitable and reliable than TOE to detect thrombi of the pulmonary vein, because of no influence of pulmonary air.
Background
Atrial fibrillation (AF) causes approximately 15% of ischaemic stroke.1 One important cause for stroke is left atrial appendage (LAA) thrombi of the patients with AF. Warfarin is an option for the prevention of thromboembolic events in subjects with AF. Dabigatran, rivaroxaban and apixaban are other possible options for anticoagulant treatment.2 Before cardioversion, the patients are examined by transoesophageal echocardiography (TOE) to check whether they have LAA thrombi or not.3 Although TOE is the routine and semi-invasive clinical tool to detect LAA and atrial thrombi, TOE is technically difficult to some extent, so it relies on an experienced operator. Moreover, TOE is unpleasant for the patients. In addition, TOE cannot describe LAA from side to side, especially the enlarged LAA of patients with AF. Shortly after restoration of sinus rhythm, 2 to 3% of patients seemingly without LAA thrombi on TOE have an embolic event.4 Although the cause is elusive, there should exist unidentified thrombi in undetectable LAA or pulmonary vein. One of the causes might be pulmonary vein thrombi, but little is known about pulmonary vein thrombi, presently.
It is difficult to visualise pulmonary vein thrombi by TOE because of being averted by pulmonary air. So, alternative imaging modalities to rule out pulmonary vein thrombi are needed. Therefore we evaluated the ability of the contrast-enhanced 64-slice multidetector CT (64-MDCT), the cardiac CT scan, to visualise pulmonary vein thrombi in patients with AF.
Case presentation
The patient was a 77-year-old male and had a lacuna infarction in the pons. He was referred to our hospital for the evaluation of the source of cerebral infarction. He was treated with aspirin (82 mg id) only. No previous treatment with warfarin had been performed. A 64-MDCT scan demonstrated that 3 to 4 mm thrombus was situated at the proximal side of right upper pulmonary vein (figure 1; axial, figure 2; sagittal). After 2 months warfarin therapy, the thrombus disappeared (figure 3; axial).
Figure 1.
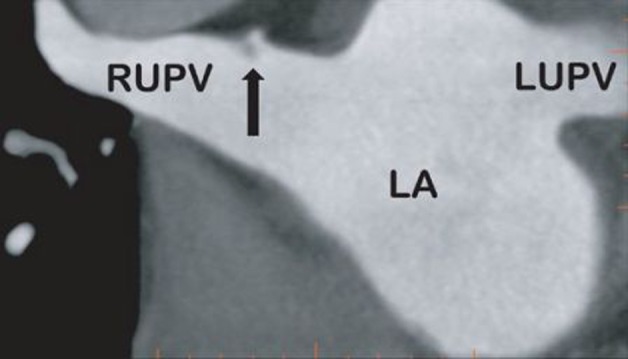
Axial image showing a thrombus (3 to 4 mm) within the right upper pulmonary vein (arrow) before warfarin therapy. LUPV, left upper pulmonary vein, RUPV, right upper pulmonary vein, LA, left atrium.
Figure 2.
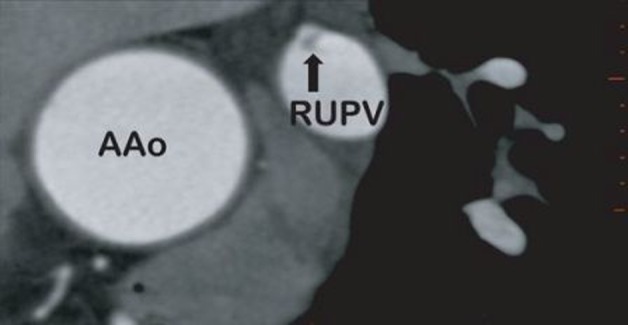
Sagittal image showing a thrombus (3 to 4 mm) within the right upper pulmonary vein (arrow) before warfarin therapy. AAo, ascending aorta, RUPV, right upper pulmonary vein.
Figure 3.
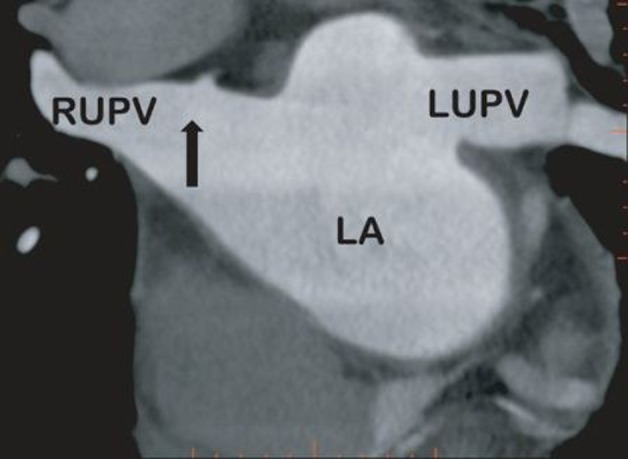
Axial image showing the distinguished thrombus within the right upper pulmonary vein (arrow) after 2-month warfarin therapy. LUPV, left upper pulmonary vein, RUPV, right upper pulmonary vein, LA, left atrium.
Treatment
Warfarin (1) 2T.
Discussion
As far as we know, this is the first reported case to show a thrombus of the pulmonary vein. Shortly after AF is restored to sinus rhythm, 2 to 3% of patients seemingly without LAA thrombi on TOE before cardioversion have an embolic event.4 Little is known about the cause. Although TOE is the usual tool to visualise the left atrium, a part of LAA and thoracic aorta including the thoracic arch, pulmonary vein thrombi were not always detected because of pulmonary air. A 64-MDCT scan has appeared as a non-invasive tool that enables us to evaluate vascular stenosis and the status of plaque. Additionally, a 64-MDCT scan can more easily and completely assess the LAA5 and the pulmonary vein thorombi. In patients with AF, LAA becomes large and strange shapes, so a 64-MDCT has the strength in demonstrating 3D reconstruction of LAA. Disadvantages of the use of a 64-MDCT scan are the necessity to use iodinated contrast medium as well as an increase in patient radiation exposure.
In conclusion, pulmonary vein thrombi as well as LAA thrombi could be detected by a 64-MDCT scan. We should anticoagulate patients with pulmonary vein thrombi to prevent an embolic event such as cerebral infarction.
Learning points.
-
▶
Thrombus within the pulmonary vein may be one of the causes for cerebral infarction, which may be a largely underdiagnosed entity.
-
▶
64-MDCT has been useful to identify thrombi of the pulmonary vein.
-
▶
Although TOE is the routine and compromised clinical tool to detect the LAA thrombi, 64-MDCT may be better than TOE for the detection of thrombi in pulmonary veins.
Footnotes
Competing interests None.
Patient consent Obtained.
References
- 1.Kannel W, Wolf PA. Epidemiology of atrial fibrillation. In: Falk RH, Podrid PJ, eds. Atrial Fibrillation: Mechanisms and Management. New York: Raven Press; 1992:81–92 [Google Scholar]
- 2.Camm AJ, Kirchhof P, Lip GY, et al. ; European Heart Rhythm Association; European Association for Cardio-Thoracic Surgery; ESC Committee for Practice Guidelines; Document Reviewers Guidelines for the management of atrial fibrillation: the Task Force for the Management of Atrial Fibrillation of the European Society of Cardiology (ESC). Europace 2010;12:1360–420 [DOI] [PubMed] [Google Scholar]
- 3.Klein AL, Murray RD, Grimm RA. Role of transesophageal echocardiography-guided cardioversion of patients with atrial fibrillation. J Am Coll Cardiol 2001;37:691–704 [DOI] [PubMed] [Google Scholar]
- 4.Black IW, Fatkin D, Sagar KB, et al. Exclusion of atrial thrombus by transesophageal echocardiography does not preclude embolism after cardioversion of atrial fibrillation. A multicenter study. Circulation 1994;89:2509–13 [DOI] [PubMed] [Google Scholar]
- 5.Takeuchi H. A 64-slice multi-detector CT scan could evaluate the change of the left atrial appendage thrombi of the atrial fibrillation patient, which was reduced by warfarin therapy. BMJ Case Rep 2011:doi:10.1136/bcr.11.2009.2491 [DOI] [PMC free article] [PubMed] [Google Scholar]