

Abstract
Objective. The aim of this study was to find out the prevalence of overweight and obesity among adolescents in seven Arab countries using similar reference standard. Methods. A school-based cross-sectional study was carried out in seven cities in Arab countries, namely, Algeria, Jordan, Kuwait, Libya, Palestine, Syria, and United Arab Emirates. A multistage stratified random sampling technique was used. The total sample included was 4698 adolescents aged from 15 to 18 years (2240 males, 2458 females). The International Obesity Task Force (IOTF) reference standard was used to classify the adolescents as nonobese, overweight, and obese. Results. Among males, overweight was highest among Kuwaiti adolescents (25.6%), followed by Jordanian (21.6%), and Syrian (19.7%) adolescents. Among females, the highest prevalence of overweight was reported in Libyan adolescents (26.6%), followed by Kuwaiti (20.8%), and Syrian (19.7%) adolescents. As for obesity, Kuwaiti adolescents showed the highest prevalence of obesity for both males (34.8%) and females (20.6%). Conclusion. There is an urgent need to establish a plan of action to combat obesity in schoolchildren in these countries.
1. Introduction
The proportion of adolescents who are overweight or obese is rapidly increasing worldwide. Adolescence is a vulnerable period for the development of obesity and also appears to be a critical period for establishing risk factors for some chronic diseases in adulthood [1]. Available statistics indicate that an alarming proportion of people in most Arab countries suffer from obesity. Studies have revealed that the prevalence of overweight and obesity among adolescents in Arab countries ranges from 18% to 44% [2]. In general, overweight has been found to be more prevalent than obesity in both boys and girls. However, the prevalence of obesity by gender at the adolescent stage (10–18 years) does not indicate the same trend. In countries such as Bahrain, Egypt, Tunisia, Kuwait, and Qatar, the prevalence of overweight is higher among girls than boys. Obesity is also higher among adolescent girls than boys in Bahrain, Egypt, and Kuwait. In some countries such as Lebanon and the United Arab Emirates (UAE), the percentage of overweight and obesity is higher in boys than girls [3].
Obesity management is an important step in the prevention and control of chronic noncommunicable diseases, such as cardiovascular disease, diabetes, hypertension, and some kinds of cancer [4]. These diseases contribute to 60% of overall morbidity and mortality in most Arab countries [5]. Therefore, understanding the prevalence of obesity among schoolchildren is essential to any strategy for combating obesity in the community [6]. Although, there is information about obesity among schoolchildren in some Arab countries, there is a lack of such data for other countries such as Algeria, Djibouti, Libya, Somalia, Sudan, Palestine, and Yemen [3]. However, there are two main reservations about using the available data on obesity among schoolchildren: (a) the use of such a wide age range (6–18 years) does not take into consideration the prepuberty and puberty stages which have a significant effect on weight gain [7]; (b) the use of different reference standards and cutoffs to determine obesity in turn provide different rates of overweight and obesity. In Bahrain, for example, Al-Sendi and colleagues [8] used three different sets of criteria to determine the prevalence of obesity among adolescents aged 12–17 years, (IOTF, WHO, and CDC references). They found that there was a considerable variation in the prevalence of obesity between these standards. In general, the WHO reference standard gave a higher prevalence of obesity, but a lower prevalence of overweight than other standards.
The objectives of this study, therefore, were to provide the prevalence of overweight and obesity among adolescents within a narrower age range of 15–18 years using the IOTF reference standard, and to find out the cross-cultural differences in the prevalence of obesity in seven Arab countries, namely, Algeria, Jordan, Kuwait, Libya, Palestine, Syria, and UAE.
2. Methods
This is a school-based, cross-sectional, multicentre collaborative study. It is a part of the ARAB-EAT Project, which aims to study obesity and eating disorders, and barriers to healthy eating and physical activity in large cities in Arab countries. The target population of this study was adolescents in secondary schools (15–18 years). Seven Arab countries participated in this study.
The minimum sample size in each city calculated as the sample size within ±0.05 of the population proportion with a 95% confidence level. A multistage stratified random sampling procedure was used to select the subjects. At the first stage, each city was divided into administrative regions, which varied from two to five regions, depending on the countries. Then, the schools were selected proportionally from each administrative region. The schools were grouped into boys and girls secondary schools. Only governmental schools were included, due to the difficulty in obtaining permission from private schools and the lack of data regarding these schools. At the second stage, classes were selected for each secondary level (levels 10, 11, and 12) in each school using a simple random method. Therefore, the number of adolescents selected varied, based on the number of students in each class and the number of selected schools, which in turn depended on the total secondary school population in each city.
To assure the accuracy and consistency of the methodology (sampling procedure, measurements, and collection of the data), a standardized protocol was prepared and distributed to all the participating centres in the seven countries. Each centre was responsible for training its research team and obtaining ethical authorization and approval from the governmental institutes (generally the Ministry of Education). The total sample size in the seven Arab countries was 4698 adolescents (2240 boys, 2458 girls), ranging from a total of 459 students in Algeria to 1062 in Syria. It is worth noting that due to the difficulty in obtaining permission from one administrative region in an Algiers city, the number of selected schools in that case represented two geographical regions instead of three. This may affect the total prevalence of overweight and obesity in this city. All the data were collected between March 2010 and January 2011.
Weight and height were taken using a standard procedure. All measurements were performed by trained nutritionists or physical education teachers. Body weight was measured to the nearest 100 grams using calibrated portable scales. Height was measured to the nearest centimeter with the subject in full standing position, using a calibrated measuring rod. All measurements were taken with minimal clothing and without shoes.
Data were first entered in an Excel file, the entered data were then sent to the central processing station (Bahrain), along with the questionnaires for cleaning the data and carrying out the analysis, using the SPSS statistical package. The International Obesity Task Force (IOTF) reference standard was used to classify the adolescents into three categories: nonobese, overweight, and obese [9]. Data for age, weight, height, and BMI were presented as means and standard deviations. One way ANOVA was used to determine the differences in anthropometric measurements between countries, and between males and females.
3. Results
The sample sizes, means, and standard deviations for age, weight, height, and body mass index of adolescents (15–18 years) according to gender in seven Arab cities are presented in Table 1. The mean age is very close among the seven countries, ranging from 16.15 years in Libya to 16.96 years in Algeria. Significant differences in age, between sexes and among countries were revealed using one way ANOVA. In general, males were significantly heavier than females in all countries. Kuwaiti adolescents showed the highest mean weight among both males (82.7 ± 23.1 kg) and females (65.1 ± 20.5 kg); whereas, the lowest mean weight for males was observed in Algeria (64.0 ± 10.9 kg), and for females was found in UAE (54.6 ± 14.2 kg). Algerian adolescent males showed the highest mean height (173.4 ± 7.2 cm), while the highest mean for females was observed in Jordan (162.1 ± 5.7 cm). The lowest mean height was found in Libya for both males (167.4 ± 7.4 cm) and females (157.9 ± 5.5 cm). As for BMI, the highest mean was found in Kuwait for both males (28.1 ± 7.5 kg/m2) and females (25.6 ± 7.7 kg/m2). The differences in weight, height, and BMI were analysed using one way ANOVA and were statistically significant between the seven countries for both genders (P < 0.000).
Table 1.
Sample size, means, and standard deviations (SD) for age, weight, height, and BMI of adolescents (15–18 years) in seven Arab countriesa.
| Variables | Sex | Algeria (Algiers city) |
Jordan (Amman) |
Kuwait (Kuwait city) |
Libya (Tripoli) |
Palestine (Al-Khalil) |
Syria (Damascus) |
UAE (Sharjah) |
|---|---|---|---|---|---|---|---|---|
| Sample size | M | 194 | 462 | 273 | 280 | 220 | 549 | 262 |
| F | 265 | 475 | 355 | 350 | 257 | 513 | 243 | |
| Age (years) (Mean ± SD) |
M | 16.90 ± 0.83 | 16.45 ± 0.58 | 16.70 ± 1.0 | 16.15 ± 0.94 | 16.40 ± 0.92 | 16.21 ± 0.85 | 16.41 ± 0.93 |
| F | 16.96 ± 0.79 | 16.54 ± 0.84 | 16.52 ± .095 | 16.17 ± 0.95 | 16.31 ± 0.93 | 16.41 ± 0.95 | 16.54 ± 0.99 | |
| Weight (kg) (Mean ± SD) |
M | 64.0 ± 10.9 | 67.7 ± 16.5 | 82.7 ± 23.1 | 64.2 ± 14.7 | 61.9 ± 13.0 | 66.8 ± 14.2 | 70.0 ± 21.4 |
| F | 58.8 ± 10.5 | 58.9 ± 10.9 | 65.1 ± 20.5 | 59.9 ± 13.3 | 56.1 ± 9.8 | 58.1 ± 10.0 | 54.6 ± 14.2 | |
| Height (CM) (Mean ± SD) |
M | 173.4 ± 7.2 | 170.8 ± 7.1 | 171.2 ± 7.0 | 167.4 ± 7.4 | 169.3 ± 7.0 | 172.4 ± 15.4 | 169.4 ± 12.0 |
| F | 161.7 ± 5.7 | 162.1 ± 5.7 | 159.3 ± 6.6 | 157.9 ± 5.5 | 160.3 ± 5.8 | 160.0 ± 5.8 | 157.9 ± 7.2 | |
| BMI (kg/m2) (Mean ± SD) |
M | 21.3 ± 3.7 | 23.1 ± 5.1 | 28.1 ± 7.5 | 22.8 ± 4.5 | 21.5 ± 4.0 | 22.5 ± 4.4 | 26.9 ± 36.1 |
| F | 22.5 ± 3.6 | 22.4 ± 3.9 | 25.6 ± 7.7 | 24.0 ± 5.0 | 21.8 ± 3.4 | 22.7 ± 3.7 | 21.9 ± 5.7 |
aOne way ANOVA tests were significantly different between countries (P < 0.000) for both males and females.
The prevalence of overweight and obesity among adolescents in seven Arab cities using the IOTF standard according to gender is shown in Table 2. Among males, overweight was most prevalent among Kuwaiti adolescents (25.6%), followed by Jordanian (21.6%), and Syrian (19.7%) adolescents; while among females, the highest prevalence was found in Libya (26.6%), followed by Kuwait (20.8%), and Syria (19.7%). Regarding obesity, Kuwaiti adolescents showed the highest prevalence among both males (34.8%) and females (20.6%). In general, obesity was more prevalent among males than females in all countries included in this study. However, the prevalence of overweight was inconsistent between sexes.
Table 2.
Prevalence of overweight and obesity among adolescents (15–18 years) in seven Arab countries based on IOTF reference.
| Obesity status | ||||||||
|---|---|---|---|---|---|---|---|---|
| Country (city) |
Sex | Nonobese | Overweight | Obese | P value* | |||
| No. | (%) | No. | (%) | No. | (%) | |||
| Algeria (Algiers city) |
M | 168 | (86.6) | 18 | (9.3) | 8 | (4.1) | <0.1372 |
| F | 212 | (80.0) | 41 | (15.5) | 12 | (4.5) | ||
| Jordan (Amman) |
M | 315 | (68.2) | 100 | (21.6) | 47 | (10.2) | <0.0005 |
| F | 370 | (77.9) | 83 | (17.5) | 22 | (4.6) | ||
| Kuwait (Kuwait city) |
M | 108 | (39.6) | 70 | (25.6) | 95 | (34.8) | <0.0000 |
| F | 208 | (58.6) | 74 | (20.8) | 73 | (20.6) | ||
| Libya (Tripoli) |
M | 207 | (74.0) | 46 | (16.4) | 27 | (9.6) | <0.007 |
| F | 222 | (63.4) | 93 | (26.6) | 35 | (10.0) | ||
| Palestine (Al-Khalil) |
M | 181 | (82.3) | 28 | (12.7) | 11 | (5.0) | <0.7095 |
| F | 216 | (84.0) | 32 | (12.5) | 9 | (3.5) | ||
| Syria (Damascus) |
M | 401 | (73.0) | 111 | (20.3) | 37 | (6.7) | <0.5898 |
| F | 383 | (74.7) | 103 | (20.1) | 27 | (5.3) | ||
| UAE (Sharjah city) |
M | 168 | (64.1) | 44 | (16.8) | 50 | (19.1) | <0.0000 |
| F | 194 | (79.8) | 33 | (13.6) | 16 | (6.6) | ||
*Difference between male and female.
Figures 1 and 2 illustrate the comparison of the prevalence of overweight and obesity among adolescent males and females in the seven Arab countries, respectively. Kuwaiti males showed the highest prevalence of overweight and obesity (60.4%), while the lowest prevalence was reported in Algeria (13.4%). As for females, the highest prevalence was also found in Kuwaiti females (41.4%) and the lowest prevalence was in Palestinian females (16%).
Figure 1.
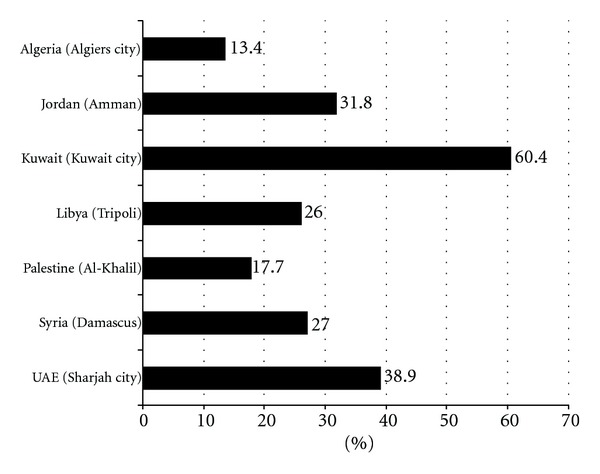
Comparison in prevalence of overweight and obesity among male adolescents (15–18 years) in seven Arab cities.
Figure 2.
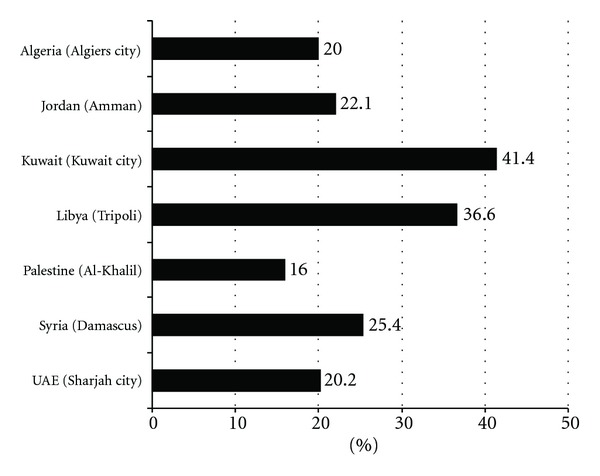
Comparison in prevalence of overweight and obesity among female adolescents (15–18 years) in seven Arab cities.
A comparison between the IOTF and CDC reference standard for the prevalence of overweight and obesity among adolescents (15–18 years) in seven Arab countries is presented in Table 3. In general, the CDC reference provided a lower prevalence of overweight and higher prevalence of obesity than the IOTF reference. For example, the prevalence of overweight in Algerian males was 9.3% based on the IOTF reference, compared with 4.6% based on the CDC reference. The corresponding proportions for obesity were 4.1% and 9.6%, respectively.
Table 3.
Comparison between IOTF and CDC reference standards in prevalence of overweight and obesity in seven Arab countries.
| Country | Sex | Overweight | % difference | Obesity | % difference | ||
|---|---|---|---|---|---|---|---|
| IOTF | CDC | IOTF | CDC | ||||
| Algeria | M | 9.3 | 4.6 | −4.7 | 4.1 | 5.6 | +1.5 |
| F | 15.5 | 12.1 | −3.40 | 4.5 | 4.5 | 0.0 | |
| Jordan | M | 21.6 | 15.9 | −5.7 | 10.2 | 13.1 | +2.9 |
| F | 17.5 | 14.2 | −3.3 | 4.6 | 5.2 | +0.6 | |
| Kuwait | M | 25.6 | 15.4 | −10.2 | 34.8 | 42.1 | +7.3 |
| F | 20.8 | 17.7 | −3.10 | 20.6 | 21.1 | +0.5 | |
| Libya | M | 16.4 | 11.1 | −5.3 | 9.6 | 12.6 | +3.0 |
| F | 26.6 | 20.9 | −5.7 | 10.0 | 11.4 | +1.4 | |
| Palestine | M | 12.7 | 8.6 | −4.1 | 5.0 | 5.9 | +0.9 |
| F | 12.5 | 10.5 | −2.0 | 3.5 | 3.5 | +0.0 | |
| Syria | M | 20.3 | 13.5 | −6.8 | 6.7 | 7.5 | +0.8 |
| F | 20.1 | 15.8 | −4.3 | 5.3 | 5.5 | +0.2 | |
| UAE | M | 16.8 | 11.1 | −5.7 | 19.1 | 22.5 | +3.4 |
| F | 13.6 | 11.5 | −2.1 | 6.6 | 7.0 | +0.4 | |
CDC reference: overweight 85th centile to <95th centile of BMI for age and sex.
Obesity ≥95th centile of BMI for age and sex.
4. Discussion
This paper has presented for the first time a comparison of the prevalence of overweight and obesity in seven Arab countries using a similar methodology and reference standard (IOTF). The findings have revealed a relatively high percentage of overweight among adolescents (15–18 years) in all countries studied, ranging from 9.3% in Algeria to 25.6% in Kuwait. As for obesity, the prevalence was higher in males than females, and ranged from 4.1% in Algeria to 34.8% in Kuwait.
It is difficult to compare the findings of this study with many previously published studies because of the differences in the standard used and in the age range. Moreover, there has been an absence of published data on adolescent obesity in some Arab countries included in this study, such as Algeria, Libya, and Sharjah. However, when the results of this study are compared with those reported in Kuwait for 14–19 year olds using the IOTF standard [10], we noticed that the present data showed a higher prevalence of obesity among boys (34.8% versus 24.8%), and a similar finding among girls (20.6% versus 20.0%). As for overweight, the findings of this study were 25.6% for boys, compared with 18.8% in the previous study, and the equivalent proportions for girls were 20.8% and 25.3%, respectively. It is important to mention that there was a 6–10 years gap between the two studies, and we can observe that obesity is increasing among male Kuwaitis, but not among females. Similar findings were seen when we compared the present data for Sharjah (UAE) with the national data for UAE adolescents aged 10–19 years [11], using same reference standard (IOTF). There was an increase in proportion of obesity among males (19.1% versus 13.2%), but a decrease in females (6.6% versus 11.0%). For overweight, the present data showed a lower prevalence (16.8% versus 21.2% for boys and 13.6% versus 21.7% for girls). Nevertheless, it is difficult to reach a concrete conclusion, since we are comparing national data with regional data and a different age group. Therefore, it is necessary in any national information on obesity to show the regional differences in the obesity proportion.
The high prevalence of overweight and obesity among some Arab countries, especially in Kuwait, could be due to rapid nutrition transition, which started earlier in Kuwait than in other countries. In addition, Kuwait has the highest socioeconomic status among these countries, which may contribute to the increase in the prevalence of obesity [3]. In general, the difference in the prevalence of obesity between the seven Arab countries can be attributed to several factors such as ethnicity, economic status, physical activity, dietary habits, timing of puberty, and genetic admixtures [12, 13].
Overweight and obesity were more prevalent among males in Jordan, Kuwait, and UAE, than among females. Findings similar to this are also seen in Western countries [14]. BMI is an expression of weight related to height, not adiposity, and there is no standard definition of adiposity or excess body fat in childhood against given BMI levels in the Arab countries. The higher prevalence of obesity among males compared to females in some Arab countries may be related to the difference in timing of puberty, muscular tissue, and dietary habits between boys and girls. The association between obesity and the timing of puberty differs among populations [13, 15].
The prevalence of overweight and obesity among adolescents (using different reference standards) in previous reports in Jordan [16], Kuwait [10], Palestine [17], Syria [18], and UAE [11] is relatively high, which is also confirmed by this study. This study has also suggested a high prevalence of overweight and obesity in middle-income countries, such as Libya, and in poor countries, such as Palestine. A plan of action to prevent and control obesity should be urgently established in the Arab countries, especially among children and adolescents to combat the comorbidities associated with obesity. This study provides comparable and useful data to build on for this plan of action. We hope that this study will stimulate researchers in other Arab countries to carry out similar surveys to compare obesity in this region.
References
- 1.Campbell KJ, Crawford DA, Salmon J, Carver A, Garnett SP, Baur LA. Associations between the home food environment and obesity-promoting eating behaviors in adolescence. Obesity. 2007;15(3):719–730. doi: 10.1038/oby.2007.553. [DOI] [PubMed] [Google Scholar]
- 2.Musaiger AO, Sadeq A, Obeid O. The paradox of nutrition-related diseases in the Arab countries. Journal of Environmental Research and Public Health. 2011;8(9):3637–3671. doi: 10.3390/ijerph8093637. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Musaiger AO. Overweight and obesity in eastern Mediterranean region: prevalence and possible causes. Journal of Obesity. 2011:17 pages. doi: 10.1155/2011/407237.407237 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Sibai AM, Nasreddine L, Mokdad AH, Adra N, Tabet M, Hwalla N. Nutrition transition and cardiovascular disease risk factors in middle East and North Africa countries: reviewing the evidence. Annals of Nutrition and Metabolism. 2011;57(3-4):193–203. doi: 10.1159/000321527. [DOI] [PubMed] [Google Scholar]
- 5.Habib SH, Saha S. Burden of non-communicable disease: global overview. Diabetes and Metabolic Syndrome. 2010;4(1):41–47. [Google Scholar]
- 6.Musaiger AO, Al HM, Al-Qahtani A, et al. Strategy to combat obesity and to promote physical activity in Arab countries. Diabetes, Metabolic Syndrome and Obesity. 2011;4:89–97. doi: 10.2147/DMSO.S17322. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Lobstein T, Baur L, Uauy R. Obesity in children and young people: a crisis in public health. Obesity Reviews, Supplement. 2004;5(1):4–104. doi: 10.1111/j.1467-789X.2004.00133.x. [DOI] [PubMed] [Google Scholar]
- 8.Al-Sendi AM, Shetty P, Musaiger AO. Prevalence of overweight and obesity among Bahraini adolescents: a comparison between three different sets of criteria. European Journal of Clinical Nutrition. 2003;57(3):471–474. doi: 10.1038/sj.ejcn.1601560. [DOI] [PubMed] [Google Scholar]
- 9.Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Establishing a standard definition for child overweight and obesity worldwide: international survey. British Medical Journal. 2000;320(7244):1240–1243. doi: 10.1136/bmj.320.7244.1240. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Department of Food and Nutrition Administration. Kuwait Nutritional Surveillance System. Shuwaikh, Kuwait: Ministry of Health; 2005. [Google Scholar]
- 11.UAE-GSHS. United Arab Emirates Global School-Based Student Survey. Abu-Dhabi, Emirates: United Arab Emirates; 2005. [Google Scholar]
- 12.McMurray RG, Harrell JS, Deng S, Bradley CB, Cox LM, Bangdiwala SI. The influence of physical activity, socioeconomic status, and ethnicity on the weight status of adolescents. Obesity Research. 2000;8(2):130–139. doi: 10.1038/oby.2000.14. [DOI] [PubMed] [Google Scholar]
- 13.Styne DM. Puberty, obesity and ethnicity. Trends in Endocrinology and Metabolism. 2004;15(10):472–478. doi: 10.1016/j.tem.2004.10.008. [DOI] [PubMed] [Google Scholar]
- 14.Ogden CL, Carroll MD, Curtin LR, Lamb MM, Flegal KM. Prevalence of high body mass index in US children and adolescents, 2007-2008. Journal of the American Medical Association. 2010;303(3):242–249. doi: 10.1001/jama.2009.2012. [DOI] [PubMed] [Google Scholar]
- 15.Ahmed ML, Ong KK, Dunger DB. Childhood obesity and the timing of puberty. Trends in Endocrinology and Metabolism. 2009;20(5):237–242. doi: 10.1016/j.tem.2009.02.004. [DOI] [PubMed] [Google Scholar]
- 16.Ahmed MN, Darawshah MA. Anthropometric indicators of overweight and obesity and dietary habits of school children 6–12 years in Jordan. Arab Journal of Food Nutrition. 2002;3:225–240. [Google Scholar]
- 17.Abdul-Rahim HF, Holmboe-Ottesen G, Stene LCM, et al. Obesity in a rural and an urban Palestinian West Bank population. International Journal of Obesity. 2003;27(1):140–146. doi: 10.1038/sj.ijo.0802160. [DOI] [PubMed] [Google Scholar]
- 18.Nasreddine L, Mehio-Sibai A, Mrayati M, Adra N, Hwalla N. Adolescent obesity in Syria: prevalence and associated factors. Child: Care, Health and Development. 2010;36(3):404–413. doi: 10.1111/j.1365-2214.2009.01042.x. [DOI] [PubMed] [Google Scholar]