

Abstract
Background:
Herpes simplex virus type 2 (HSV-2) is the cause of most genital herpes. Now, HSV-1 has become an important cause and represents even about 30% of genital herpes in some countries. So, study related to genital herpes should consider both HSV-1 and HSV-2.
Aim:
To examine trends in HSV-1 and 2 seroprevalence by Serum HSV-1 and 2 IgM in all type of sexually transmitted disease (STD) patients and also to evaluate correlation of serum HSV-1 and 2 IgM in STD.
Materials and Methods:
150 patients attending the STD clinic attached to a tertiary care hospital of Ahmedabad were included in the study. Serum HSV-1 and 2 IgM correlations with clinical manifestations of recurrent and non-recurrent type of genital herpes patients and other non-herpetic STD patients were studied.
Results:
The overall serum HSV-1 and 2 IgM in STD seroprevalence were 15.66%. Female has significant higher prevalence (P < 0.05). STD cases and HSV seroprevalence were specially concentrated in persons aged 21 to 30 years. Among those positive with HSV, the distribution of STD are wide spread and found in non-herpetic group at high frequency. Out of total 23 serum HSV-1 and 2 IgM positive, 12 and 11 are distributed in herpetic and non-herpetic STDs, respectively.
Discussion and Conclusion:
Though serum HSV-1 and 2 IgM in STDs are less diagnostic, they help to see the iceberg part of the infection among the population concerned in recent scenario or in another words, it provides recent infective burden.
Keywords: Genital herpes, HSV-1 and 2 IgM, STD
INTRODUCTION
Sexually transmitted diseases (STDs) are markers of high risk sexual behavior. Herpes simplex virus (HSV) types 1 and 2 cause genital herpes infections and are the most common cause of genital ulcer disease worldwide.[1,2] Considering that herpes is a life long infection, not cured by antimicrobial treatment, HSV-2 antibodies are a much more reliable indicator of risky behavior than Treponema palladium antibodies.[3,4] As large number of genital infections are also caused by HSV-1. The present study was thus undertaken for finding IgM antibodies against HSV-1 and 2.
While most herpetic infections are asymptomatic or mild, some can be transmitted to neonates and are associated with other STDs and cervical neoplasia. Genital herpes may contribute more to human immunodeficiency virus (HIV) infection because of its higher frequency than other STDs, the recurrence of genital herpes and large number of herpes infected persons who continue their sexual activities despite being infectious.[3] Serology is the only practical way to diagnose HSV infection in individuals without any relevant clinical history or presentation with lesions.[5] Immunoglobulin M (IgM) antibodies to HSV are increased to four times the normal value 2–4 weeks after the infection and the enzyme linked immuno sorbent assay (ELISA) is a specific, sensitive, and simple test which confirms the infection by HSV.[6]
MATERIALS AND METHODS
One hundred fifty (150) blood samples were collected from patients attending the STD clinic attached to a tertiary care hospital of Ahmedabad. These patients’ clinical diagnosis was made by department of skin and venereal diseases, B. J. Medical College, Ahmedabad. The consecutive patients only whose clinical history suggested that clinical manifestations of STDs were established by sexual route were included in this study. Along with blood sample, all clinical history especially regarding the recurrence of genital herpes was also taken. The sera were tested for HSV-1 and 2 IgM type specific antibodies by ELISA CA, USA. As we wanted to study genital herpes infection as a whole, irrespective type of causative agent, we used ELISA assay that detects HSV-1 and 2 IgM antibodies simultaneously. Results are analyzed here.
RESULTS
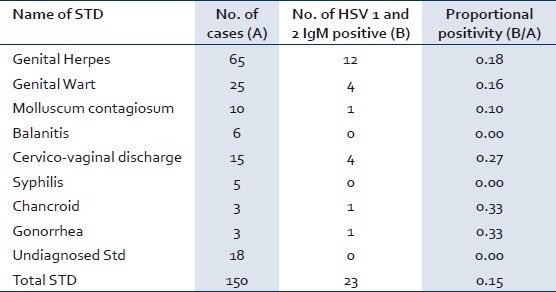
In our study, out of 150 patients we found 23 (15.66%) for serum HSV-1 and 2 IgM from all the STD patients. In disease wise analysis, numbers of genital herpes were the highest among all diseases and their proportional positivity for serum HSV-1 and 2 IgM was 18% only. All other STDs and their proportional positivity of serum HSV-1 and 2 IgM antibodies are as described in Table 1.
Table 1.
Disease pattern in STD clinic patients
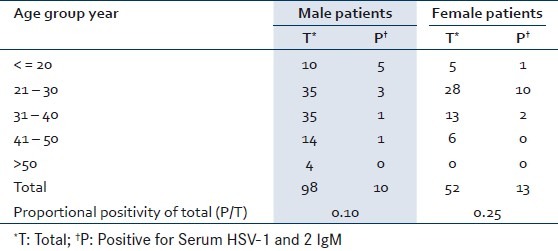
98 male and 52 female out of 150 STD patients, 10 male and 13 female were positive for serum HSV-1 and 2 IgM. Female has statistically significant higher positive proportion than male (P <0.05%).Though in study; there were no bar in age group selection, majority of the patients (>97%) of all STDs fall into 15–49 age group. Overall 21–30 age group has more number of HSV positive patients (52% ) than any other age group and especially in female 76% HSV positive in this age group [Table 2].
Table 2.
Age - Sex wise distribution of STD patients
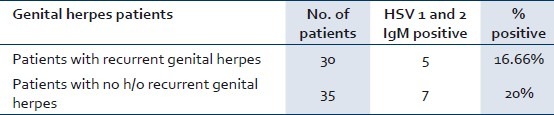
Out of 150 patients, 65 were of clinical symptoms of genital herpes. From these 65 patients, 30 and 35 patients were with and without history of recurrent herpes, respectively. Serum HSV-1 and 2 IgM were found positive in 16.66% (6 out o 30) in patients with recurrent history of genital herpes and also in 20% (7 out of 35) in patients without any clinical history of herpes in the past [Table 3].
Table 3.
HSV 1 and 2 IgM among with and without history of recurrent genital herpes
DISCUSSION
This study applies the clinical presentation of STD and serological herpetic infection correlation in a STD clinic of a tertiary care hospital in India. Using serum HSV-1 and 2 IgM testing provides valuable information. That will help in interpreting the test result of serum HSV-1 and 2 IgM in any STD patients as many times serological test reports are given unnecessary higher importance without knowing the surrounding factors. The herpes simplex virus persists life-long in neuronal cells (especially in trigeminal and sacral ganglia) and is frequently reactivated with or without clinical manifestations.[7] This study effectively shows that when the disease (e.g., genital herpes) whose prevalence is more in population concerned and have latent period, its serological test especially detecting IgM only helps in screening to detect the burden of the disease, but has less correlation with the clinical symptoms.
All 23 serum HSV-1 and 2 IgM positive are also distributed in other type of STDs (48% – 11 out of 23), apart form genital herpes cases (52% – 12 out of 23). Now a days, serum HSV-1 and 2 IgM found positive in patients of non-herpetic clinical manifestations in STD patients is quite common and also reported by many authors in India as well as outside India too.[3,8,9] This shows that these patients may have either simultaneous co-infection with HSV-1 and or 2, though the virus is not clinically manifesting the herpetic symptoms and patients shows asymptomatic sero conversion or HSV-1 and /or 2 IgM reactivation.[10]
Despite the relatively high number of genital herpes positive among all STDs (12 out of 23), proportional positivity rate of serum HSV-1 and 2 IgM is highest in cervico-vaginal discharge (27%). Female as compare to male has tendency more number and early sero conversion.[11,12] In our study, a high proportion (25%) of female patient was HSV positive and even from this positive female, 84% were up to age of 30 year. These female of child bearing can act as potential transmitters to their offspring. Detection of sub clinical HSV co-infection in this group, by serology facilitates counseling regarding advisability of acyclovir therapy when needed (in addition to treating the other coexisting STD). Transmission of infection from HSV positive males to their sexual partners may further cascade the situation.[13]
In genital herpetic patients, those having no history of clinical herpetic manifestation in past, only 20% of them show positivity by serum HSV-1 and 2 IgM while others remain negative. This is not due to false clinical diagnosis but rather due to earlier primary HSV infection that did not converted in to clinical herpetic presentation and remained unrecognizable at that time. In earlier studies[14,15] of comparing the relationship between a history of herpes, symptoms suggestive of herpes, and HSV antibody prevalence, overall, only one-third of those with antibodies to HSV had a clinical diagnosis of herpes. While the patients having recurrent genital herpes in genital herpes group, 16.66% of them show positivity by serum HSV-1 and 2 IgM. It suggests that along with IgG some people with recurrent herpetic infection get reactivated IgM. So IgM cannot be taken as diagnostic for primary episode of herpetic infection only.
This study has shown that among STDs patients, overall the clinical genital herpes are increased than other STD of earlier time like gonorrhea, syphilis. Genital herpes has become the most common ulcerative STD worldwide.[2] Serological analyses have also shown less prevalence of syphilis than herpes in general as well as STD group as shown in last some studies too.[16–19]
A higher seroprevalence of HSV-1 and or 2 among females as compared to males has been recorded in the studies in India and outside India. Higher seroprevalence among younger women as compared to men of a similar age group was observed.[20–22] In our study, the prevalence of HSV-1 and 2 among males was 10% (10 out of 98) which was less compared to females 25% (13 out of 52), particularly the 21-30 age group, the male to female difference is more 8 to 35%, respectively. These differences were statistically significant.
CONCLUSION
Since most genital HSV infections are unrecognized and undiagnosed,[11] serum HSV-1 and 2 IgM helps to see the iceberg part of the infection among the population concerned. But when serum HSV-1 and 2 IgM come positive in any of the patients having STD, it may be sero-conversion of primary infection or reactivation. In the community, when HSV transmissibility increased by sexual route, case of primary infection and reactivation of herpes virus also increased. This phenomenon directly leads the level of serum HSV-1 and 2 IgM in STD patients – both herpetic and non-herpetic groups are also going to be increased. So, serum HSV-1 and 2 IgM can be used for periodically screening in STD patient to know the trend, transmissibility and load of HSV.
ACKNOWLEDGEMENTS
We are thankful to the staff of Microbiology Department and also to the Department of Skin and Venereal Disease, B. J. Medical College, Ahmedabad, India for their assistance in our study.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Singh A, Preiksaitis J, Ferenczy A, Romanowski B. The laboratory diagnosis of herpes simplex virus infections. Can J Infect Dis Med Microbiol. 2005;16:92–8. doi: 10.1155/2005/318294. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Gupta R, Warren T, Wald A. Genital herpes. Lancet. 2007;370:2127–37. doi: 10.1016/S0140-6736(07)61908-4. [DOI] [PubMed] [Google Scholar]
- 3.Aggarwal A, Kaur R. Seroprevalence of herpes simplex virus-1 and 2 Antibodies in STD clinic patients. Indian J Med Microbiol. 2004;224:244–6. [PubMed] [Google Scholar]
- 4.Bogaerts J, Ahmed J, Akhter N, Begum N, Rahman M, Nahar S, et al. Sexually transmitted infections among married women in Dhaka, Bangladesh: Unexpected high prevalence of herpes simplex type 2 infection. Sex Transm Infect. 2001;77:114–9. doi: 10.1136/sti.77.2.114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Morrow R, Friedrich D. Performance of a novel test for IgM and IgG antibodies in subjects with culture-documented genital herpes simplex virus-1 or -2 infections. Clin Microbiol Infect. 2006;12:463–9. doi: 10.1111/j.1469-0691.2006.01370.x. [DOI] [PubMed] [Google Scholar]
- 6.Hook EW, 3rd, Cannon RO, Nahmias AJ, Lee FF, Campbell CH, Jr, Glasser D, et al. Herpes simplex virus infection as a risk factor for human immunodeficiency virus infection in heterosexuals. J Infect Dis. 1992;165:251–5. doi: 10.1093/infdis/165.2.251. [DOI] [PubMed] [Google Scholar]
- 7.Buxbaum S, Geers M, Gross G, Schöfer H, Rabenau HF, Doerr HW. Epidemiology of herpes simplex virus types 1 and 2 in Germany: What has changed? Med Microbiol Immunol. 2003;192:177–81. doi: 10.1007/s00430-003-0183-0. [DOI] [PubMed] [Google Scholar]
- 8.Choudhry S, Ramachandran VG, Das S, Bhattacharya SN, Mogha NS. Serological profile of HSV-2 in patients attending STI clinic: Evaluation of diagnostic utility of HSV-2 IgM detection. Indian J Pathol Microbiol. 2009;52:353–6. doi: 10.4103/0377-4929.54992. [DOI] [PubMed] [Google Scholar]
- 9.Santos FC, de Oliveira SA, Setúbal S, Camacho LA, Faillace T, Leite JP, et al. Seroepidemiological study of herpes simplex virus type 2 in patients with the acquired immunodeficiency syndrome in the City of Niterói, Rio de Janeiro, Brazil. Mem Inst Oswaldo Cruz. 2006;101:315–9. doi: 10.1590/s0074-02762006000300016. [DOI] [PubMed] [Google Scholar]
- 10.Wald A. Herpes simplex virus type 2 transmission: Risk factors and virus shedding. Herpes. 2004;11(Suppl 3):130A–7A. [PubMed] [Google Scholar]
- 11.Madhivanan P, Krupp K, Chandrasekaran V, Karat C, Arun A, Klausner JD, et al. The epidemiology of herpes simplex virus type-2 infection among married women in Mysore, India. Sex Transm Dis. 2007;34:935–7. doi: 10.1097/OLQ.0b013e3180ca965a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Cowan FM, Johnson AM, Ashley R, Corey L, Mindel A. Antibody to herpes simplex virus type 2 as serological marker of sexual lifestyle in populations. BMJ. 1994;309:1325–9. doi: 10.1136/bmj.309.6965.1325. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Peters BP, Rastogi VL, Monica, Nirwan PS. Coinfection of HSV with other sexually transmitted diseases. Indian J Med Microbiol. 2005;23:143–4. doi: 10.4103/0255-0857.16062. [DOI] [PubMed] [Google Scholar]
- 14.Cowan FM, Johnson AM, Ashley R, Corey L, Mindel A. Relationship between antibodies to herpes simplex virus (HSV) and symptoms of HSV infection. J Infect Dis. 1996;174:470–5. doi: 10.1093/infdis/174.3.470. [DOI] [PubMed] [Google Scholar]
- 15.Koutsky LA, Ashley RL, Holmes KK, Stevens CE, Critchlow CW, Kiviat N, et al. The frequency of unrecognized type 2 herpes simplex virus infection among women. Implications for the control of genital herpes. Sex Transm Dis. 1990;17:90–4. doi: 10.1097/00007435-199004000-00009. [DOI] [PubMed] [Google Scholar]
- 16.Sgaier SK, Mony P, Jayakumar S, McLaughlin C, Arora P, Kumar R, et al. Prevalence and correlates of Herpes Simplex Virus-2 and syphilis infections in the general population in India. Sex Transm Infect. 2011;87:94–100. doi: 10.1136/sti.2010.043687. [DOI] [PubMed] [Google Scholar]
- 17.Clark JL, Konda KA, Munayco CV, Pún M, Lescano AG, Leon SR, et al. Prevalence of HIV, herpes simplex virus-2, and syphilis in male sex partners of pregnant women in Peru. BMC Public Health. 2008;8:65. doi: 10.1186/1471-2458-8-65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Yang Y, Yao J, Gao M, Su H, Zhang T, He N. Herpes simplex virus type 2 infection among female sex workers in Shanghai, China. AIDS Care. 2011;23(Suppl 1):37–44. doi: 10.1080/09540121.2011.555740. [DOI] [PubMed] [Google Scholar]
- 19.Schneider JA, Lakshmi V, Dandona R, Kumar GA, Sudha T, Dandona L. Population-based seroprevalence of HSV-2 and syphilis in Andhra Pradesh state of India. BMC Infect Dis. 2010;10:59. doi: 10.1186/1471-2334-10-59. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Shivaswamy KN, Thappa DM, Jaisankar TJ, Sujatha S. High seroprevalence of HSV-1 and HSV-2 in STD clinic attendees and non-high risk controls: A case control study at a referral hospital in south India. Indian J Dermatol Venereol Leprol. 2005;71:26–30. doi: 10.4103/0378-6323.13782. [DOI] [PubMed] [Google Scholar]
- 21.Fleming DT, McQuillan GM, Johnson RE, Nahmias AJ, Aral SO, Lee FK, et al. Herpes simplex virus type-2 in the United States, 1976 to 1994. N Engl J Med. 1997;337:1105–11. doi: 10.1056/NEJM199710163371601. [DOI] [PubMed] [Google Scholar]
- 22.Obasi A, Mosha F, Quigley M, Sekirassa Z, Gibbs T, Munguti K, et al. Antibody to herpes simplex type-2 as a marker of sexual risk behavior in rural Tanzania. J Infect Dis. 1999;179:16–24. doi: 10.1086/314555. [DOI] [PubMed] [Google Scholar]