

Abstract
Objective
To describe the methodology used to conduct a scoping review of spinal cord injury (SCI) rehabilitation service delivery in Canada, and to explain the reporting process intended to advance future service delivery.
Evidence acquisition
A SCI rehabilitation framework derived from the International Classification of Function, Disability and Health was developed to describe the goals and interprofessional processes of rehabilitation. An adapted Arksey and O'Malley (2005) methodological framework was used to conduct a scoping review of SCI rehabilitation services in Canada. Data were obtained from multiple relevant sources via survey (N = 3572 data fields) from 13 of 15 Canadian tertiary SCI rehabilitation sites, systematic reviews, white papers, literature reviews, clinical practice resources, and clinicians. Multidisciplinary teams of content experts (n = 17), assisted with data interpretation and validation by articulating practice trends, gaps, and priorities.
Evidence synthesis
The findings will be presented in an atlas, which includes aggregate national data regarding impairment and demographic characteristics, service utilization, available resources (staff and capital equipment), specialized services, local expertise, and current best practice indicators, outcome measures, and clinical guidelines. Data were collated and synthesized relative to specific rehabilitation goals. The current state of SCI rehabilitation service delivery (specific to each rehabilitation goal) is summarized in a report card within three domains, knowledge generation, clinical application, and policy change, and specifies key 2020 priorities.
Conclusion
These findings should prompt critical evaluation of current Canadian SCI rehabilitation service delivery while specifying enhancements in knowledge generation, clinical application and policy change domains likely to assist with achievement of best practices by 2020.
Keywords: Disability, Spinal cord injuries, Clinical practice, Rehabilitation, Scoping review, Service delivery
Introduction
Although more than 85 000 persons currently live with a spinal cord injury (SCI) in Canada,1 with more than 4000 new cases occurring every year, there is limited understanding of the national rehabilitation resources available to persons with SCI or their adequacy. With low incidence and prevalence rates compared with other health conditions, and the high economic burden of SCI rehabilitation (The total direct cost of acute care and rehabilitation was $123 674 in 2005/2006 Canadian Dollars2 and the fact that rehabilitation and health care service delivery is provincially funded, national strategies to direct change for SCI service delivery are at best extremely challenging. Canadian initiatives attempting to capture the spectrum of available clinical services have been plagued by the lack of existing infrastructure to enable tracking of patients and their outcomes across the continuum of care; evaluation of treatment effectiveness; or development and evaluation of related programs and policies.3 For example, the Ontario Spinal Cord Injury Registry based on the model of the national Rick Hansen Spinal Cord Injury Registry (RHSCIR) and implemented over a two-year period in Toronto and Hamilton, represented the first single source of clinical SCI data that included comprehensive rehabilitation data.3 In addition to these issues, there has been little opportunity for interprofessional and multidisciplinary research, knowledge exchange, and data sharing among SCI experts and professionals.3 The net result of these barriers to information exchange is the absence of a prior comprehensive account of SCI rehabilitation service delivery in Canada.
The Rehabilitation Environmental Scan (E-Scan) project is part of a translational research program intended to describe current SCI rehabilitation service delivery in Canadian tertiary rehabilitation centers and to create a related national dataset. This manuscript seeks to describe the methodology used to conduct a scoping review of SCI rehabilitation services in Canada and explain the atlas reporting process intended to inform and advance future SCI rehabilitation service delivery.
Methods
Defining the research question
The primary objective of this scoping review was to describe current SCI rehabilitation services for individuals with subacute and chronic SCI admitted to 13 tertiary SCI rehabilitation sites in Canada. This objective was defined by the investigators following discussion with the members of the rehabilitation arm of the SCI Solutions Translational Research Network, a national group of scientists and clinical thought leaders, frustrated by the challenges associated with articulating and promoting the processes of SCI rehabilitation. Secondary objectives were (1) to develop a rehabilitation framework that represents the goal oriented, interprofessional and multi-modal (emotional, physical, medical, and surgical) aspects of SCI rehabilitation service delivery; (2) to describe the key constructs and specific health outcomes underlying each rehabilitation goal and the related models of SCI rehabilitation service delivery; (3) to profile sites with comprehensive or exemplary services; (4) to identify national trends, gaps (regional or process disparity), and priorities in SCI rehabilitation service delivery; (5) to utilize the scoping review findings to inform future enhancements in SCI service delivery. An overview of the E-Scan scoping review methods is illustrated in Fig. 1.
Figure 1.

Overview of E-Scan Methods.
The SCI rehabilitation framework
The form and content of the data collection, synthesis and reporting of this scoping review stems from the SCI rehabilitation framework. The SCI rehabilitation framework was derived from the International Classification of Function, Disability and Health (ICF) by the study investigators. The ICF is a classification system that underlies definition, measurement, and policy formulations in the fields of health and disability.4 A hybrid of medical and social models of disability, the ICF framework depicts functioning and disability as interacting factors that further relate to the individual, and contextual factors unique to the individual including their environment, and personal factors. The dimensions are seen as also interacting with the environment, which encompasses external factors such as architectural characteristics, legal, and social structures, and climate; and personal factors (or the social context), which includes factors relating to the individual and his/her socio-cultural surroundings such as social background, education, profession, experiences, gender and age. The interplay between these factors influences how an individual experiences their SCI-related disability. These concepts are thought to be interactive and dynamic, rather than linear and static. In this framework, information is organized into the three ICF dimensions:
Body functions and structure, which consists of the physiological and psychological body functions and anatomical body parts, and incorporates impairments that may occur as a result of SCI;
Activities, which refers to the individual's the tasks and actions executed by an individual with SCI; and
Participation, which refers to the individual's involvement in life situations.
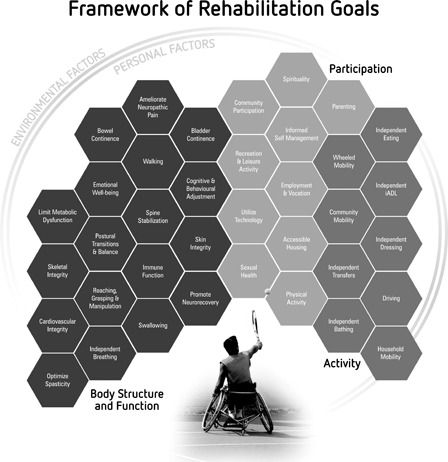
The SCI rehabilitation framework displays the goal-oriented nature of SCI rehabilitation service delivery within these dimensions – body structure and function, activity, and participation (Fig. 2). The hexagon or “mosaic tile-like appearance” of the rehabilitation goals are intended to visually represent the complex interplay of the individual, their goals and the interprofessional and multimodal nature of SCI rehabilitation service delivery, with a variety of cognitive, physical, or medical therapies and diagnostic interventions targeting multiple rehabilitation goals ongoing at any one time. The rehabilitation framework emphasizes the central role of the individual with SCI in the rehabilitation process, and the need to customize and tailor the goals and processes of rehabilitation to the individual, while taking into consideration their unique environment and personal factors. The strength of the framework is that it enables distinction between disease, consequences of disease, and contributing factors. The SCI rehabilitation framework was developed a priori to conduct of the scoping review. The rehabilitation goals were used to guide selection of relevant data elements, data collection, collation, and the data reporting processes.
Figure 2.
SCI Rehabilitation Framework.
Modified scoping review methods
We modified the scoping review methods described in the Arskey and O'Malley Framework for scoping reviews.5 This widely used scoping review framework specifies six steps for conducting a scoping review. The investigative team modified these steps in order to align with the field and project scope.
Identification of rehabilitaiton goals from the rehabilitation framework.
The decision was based on
accordance with the ICF framework,
relevance to the Canadian Context,
the state of existing literature/guidelines,
the richness of the dataset available after the multi-center data collection,
gaps – regional disparities or inequities,
stakeholder domains of interest,
correspondence with the Rick Hansen Institute's Best Practice Implementation program.
The framework presents 45 goals of rehabilitation practice: 28 in body structure and function, nine in activity, and ten in participation. Each of the 17 rehabilitation goals will be a separate chapter of the E-Scan Atlas and fall within specific ICF domains:
Body structure and function: Walking; reaching, grasping and manipulation; cardiovascular integrity; skeletal integrity; skin integrity; bowel continence; bladder continence; ameliorate neuropathic pain; independent breathing; emotional well-being; and optimizing spasticity.
Activity: Wheelchair mobility.
Participation: Community participation, employment and vocation, informed self-management, physical activity, and sexual health.
Identification of data elements relevant to primary objective
The focus of the review was to provide an account of rehabilitation service and practices. Data elements and studies were selected for inclusion based on their relevance to the rehabilitation goals and current practice. A substantial portion of the data was obtained from the E-Scan survey. The survey was developed by the investigators; consideration was given to the data elements, their relevance, clarity, and administrative burden. The survey was piloted by several sites in Ontario Windsor, London, Kingston and Toronto, then refined based on feedback prior to national dissemination. The web-based survey, included 3572 elements regarding patient utilization, availability and adequacy of staff resources, capital equipment and services. In addition, data regarding current clinical practice guidelines, care maps and publications used to guide service delivery were collected. Survey respondents were also asked to identify clinicians and scientists likely to influence practice in the next 5 years. Table 1 provides a brief overview of the E-Scan survey data elements. A letter of introduction regarding the survey process, a data element codebook, and survey guide were distributed to participating sites, prior to data collection. Survey administration was web based with typical respondents being administrators and clinicians from the 13 participating sites (Fig. 3). Data were stored in a central on-line repository. Unclear or missing data were clarified with each participating site. Data cleaning was done prior to analysis.
Table 1.
Summary of E-Scan survey data elements.
| Section heading | Data element category/descriptors (examples) |
|---|---|
| (A) Demographic, impairment, capacity & utilization data |
|
| (B) Administrative structure of site and parent organization |
|
| (C) Rehab team structure & service providers at sites |
|
| (D) Specialized equipment |
|
| (E) Diagnostic services |
|
| (F) Subspecialty clinics |
|
| (G) Discharge planning services |
|
| (H) Follow-up services |
|
| (I) Local expertise |
|
| (J)Assessments/outcomes |
|
Terms: ALC – alternate level of; C&S– Culture & Sensitivity; EMG – Electromyography; FTE – Full Time Equivalent;
MRI – Magnetic Resonance Imaging; NCS – Nerve Conduction Study; PT – Physiotherapist; TR – Therapeutic Recreation.
Figure 3.

E-Scan participating site locations.
Selection of data elements from multiple sources for inclusion
In order to provide a comprehensive account of current practice against the backdrop of best available practice, the E-Scan Investigative team examined a number and variety of additional sources. There sources included published systematic reviews (www.scireproject.com), clinical practice guidelines, clinical trial and cohort study registries, recent conference programs, relevant Canadian white papers, and grey literature for data elements relevant to the focus of the scoping review and the 17 rehabilitation goals. Coincidentally, many of the SCIRE systematic review chapter authors were recruited to assist with data identification and had recently completed extensive reviews of MEDLINE, CINAHL, etc., using long established search terms specific and data quality assessment tools including the Downs & Black checklist and PeDRO scoring systems (www.pedro.org.au).
Descriptive analysis of the data elements
The data from the E-Scan survey were analyzed using SPSS (version 19), and initial national summary reports were produced using descriptive statistics.
Collate, summarize, and report results of the review
Data for each rehabilitation goal were produced in written form for an initial audit and reviewed by an member of the E-Scan Investigative team. Conventional scoping review methods for summary and weighting of the data acquired were not used as the volume, type, and nature of the data varied widely across rehabilitation goals, rendering cross-chapter comparisons of data infeasible. Rather, we chose to rely on the experts' perception of the relevance of the data to practice as the key filters.
Consult with stakeholders
Content experts appropriate to the selected rehabilitation goals were contacted and invited to participate in a series of WebEx teleconferences regarding data interpretation and/or validation. Interprofessional working groups comprised at least five Canadians content experts per rehabilitation goal. Content review working groups then collated the survey findings with information obtained from the aforementioned data sources with their own expertise and produced analytical interpretations of the information collected. Each rehabilitation goal report included a definition of the key construct or rehabilitation goal, descriptors of current service delivery including staff, resources, practice patterns, and outcome assessments; current key practice references and guidelines in use; a list of Canadian content experts likely to influence practice in the next 5 years. Reviewers were asked to identify best practice organizations and indicators; and, to highlight clinical, research and policy barriers to service delivery throughout the data collation process based on their own experience and knowledge of the field, or new insights obtained from the discussions. Validation of the information obtained was received from practicing clinicians across the country via WebEx.
Presentation of the scoping review – using a formal KT strategy
The Atlas will feature an E-Scan report card at the conclusion of each of chapter. Report cards will provide an overall rating of SCI rehabilitation service delivery, relative to three domains: knowledge generation, reflecting current research endeavours (innovation) and their outcomes; clinical application, referring to the use of research and best practice findings and their alignment with current clinical practice; and policy change, which signifies the extent to which health policy currently enables or impedes changes to service delivery. As shown in Table 2, each report card category contains four operationally defined subelements, which are rated on a scale from insufficient to optimal (−5 to +5) and converted to a visual scale. At the bottom of each report card, there is a priority rating on a numerical scale ranging from 1 to 3, with 1 indicating the category/domain of highest priority. Priority ratings will identify one of the three categories to which prospective efforts and funding must be directed in order to achieve evolution in rehabilitation service delivery and practice (Fig. 4). Specifically, we have set our sights on the year 2020, to achieve significant enhancement in best practice. Thus, the report cards will serve as summaries for specific rehabilitation goals, as well as provide a means by which one may compare across all rehabilitation goals included in the Atlas.6 Content experts together with participating experts provide a “take home message” describing the steps required to revitalize the area of highest priority between atlas publication and 2020.
Table 2.
Elements contributing to report card domains.
| Domain | Elements | Definition/descriptor |
|---|---|---|
| Knowledge generation | Innovation/discovery | Novel methods, ideas, and/or practices that lead to advances in the field |
| Emerging evidence | The academic weight and clinical value of findings from ongoing and recently completed research studies | |
| Outcome measures | The tools being used to estimate the results of a treatment and evaluate its effectiveness | |
| Resource capacity | The extent to which the field has adequate graduate students, basic and clinical scientists with the appropriate skills to investigate the needs expressed by patients and service providers | |
| Clinical application | Integrative care | The multidisciplinary and synergistic approach to health care service delivery7 |
| Effective practice (evidence/outcomes) | The existence of clinical practice guidelines, best practice indicators or other relevant evidence to support practice implementation | |
| Practice equity | The equivalence of care provision across the country | |
| Capacity | The number of specialized staff members and the state of their professional development across the country | |
| Policy change | Environmental shift | Formation of community groups or coalitions with common SCI rehabilitation/health interests |
| Change agents | Leaders/experts/organizations willing to partner to effect policy change | |
| Societal awareness | General community awareness of the need for policy change to alter practice and influence the health of persons with SCI and/or rehabilitation service delivery | |
| Community capacity | The capacity of the SCI community and its' stakeholders to collaborate with policy makers during the planning, implementation, and evaluation of policy change |
Figure 4.

nreport card.
Discussion
Scoping reviews are an increasingly popular approach for reviewing evidence and investigating issues, particularly in the field of health.6,8–10 The methodology has enabled the collation of information from a variety of sources and people. The findings will provide baseline information on the state of Canadian SCI rehabilitation service delivery, while identifying trends and gaps in these services, thus leading to a critical re-evaluation of Canadian SCI rehabilitation practice.
Our scoping review process has likely suffered from the lack of a quality assessment or a critical appraisal assessment tool. One positive aspect of this process was use of the SCI rehabilitation framework to anchor all of our data sorting and filtering as it pertained to SCI rehabilitation service delivery.
As discussed by Levac et al.,11 synthesis of the collated scoping review data requires three key steps, “data analysis”, “reporting the results”, and “applying meaning to the results”. We chose to apply meaning to the results through use of report cards and actionable take home messages. Report cards are a known means for creating accountability to and by stakeholders.6 The report cards amalgamate information about a rehabilitation goal, highlight the specific areas/domains (knowledge generation, clinical application policy change) requiring support/attention through quality and priority ratings, and key messages from content experts to facilitate positive changes in service delivery as rapidly as possible. Our intent is that the Atlas will inform best practice implementation initiatives and the development of future Canadian clinical practice guidelines. To this end, the E-Scan Atlas will provide report cards for 17 rehabilitation goals. These Atlas features should support the abandonment of ineffective practices and enable provincial and national advocacy for appropriate practice resources to eliminate regional disparity in service provision.
The Rehabilitation E-Scan Atlas will be published in October 2012 and presented at the 5th National SCI Conference (www.sciconference.ca) in Toronto. Following publication of the E-Scan Atlas, a second phase of the project, will focus on knowledge implementation strategies by disseminating the E-Scan Atlas to various stakeholders and interested parties. When this occurs, the report cards may be used to ensure that areas of highest priority receive adequate attention and resources. The E-Scan is meant to serve as a baseline descriptor of SCI rehabilitation service delivery, prior to implementation of other national initiatives intended to influence SCI rehabilitation service provision. These initiatives include the SCI Knowledge Mobilizations Network, a network of six centers across three provinces (Ontario, Quebec, and Alberta) focused on the implementation of common best practices across participating sites, and the evolving Accreditation Canada SCI Distinction Program. If relevant stakeholders collectively focus on the areas requiring the most attention, as highlighted in each report card, it should be possible to leverage these concurrent efforts to create service delivery that is unencumbered by problems related to inadequate facilities, expertise, or policy, thus ensuring the best possible outcomes for the SCI population we serve by the year 2020.
Acknowledgements
Funding and infrastructure support to enable data collection for this project was provided by the Rick Hansen Institute. The authors acknowledge the support of the Toronto Rehabilitation Institute, which receives funding under the Provincial Rehabilitation Research Program from the Ministry of Health and Long-Term Care in Ontario. The views expressed do not necessarily reflect those of the Ministry. The authors thank Carey Yada-Lee of RHI for her graphic design assistance, and John Cobb and Heather Askes for their support with the data collection and storage process.
The authors wish to thank their many colleagues in each of the participating sites who contributed to the data collection and cleaning process.
Conflict of interest statement
The Rick Hansen Institue employs three of the authors (Noonan, Cherban, and Raschid). The remaining authors declare no conflict of interest.
References
- 1.Noonan VK, Fingas M, Farry A, Baxter D, Singh A, Fehlings MG, Dvorak MF. Incidence and prevalence of spinal cord injury in Canada: a national perspective. Neuroepidemiology 2012;38(4):219–26 [DOI] [PubMed] [Google Scholar]
- 2.Munce SE, Wodchis WP, Guilcher SJ, Couris CM, Verrier M, Fung K, Craven BC, Jaglal SB. Direct costs of adult traumatic spinal cord injury in Ontario. Spinal Cord 2012. 2012 Jul 17. doi: 10.1038/sc.2012.81. [Epub ahead of print] PMID:22801189. [DOI] [PubMed] [Google Scholar]
- 3.Verrier M, Ahn H, Craven C, Drew B, Fehlings F, Ford M, Jaglal S, Parsons D. Ontario spinal cord injury informatics: informing practice research and innovations. Ontario Neurotrauma Foundation: Toronto Ontario, Canada; 2009 [Google Scholar]
- 4.World Health Organization Towards a common language for functioning, disability, and health. ICF; Geneva: Switzerland; 2002 [Google Scholar]
- 5.Arksey H, O'Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol 2005;8(1):19–32 [Google Scholar]
- 6.Brien SE, Lorenzetti DL, Lewis S, Kennedy J, Ghali WA. Overview of a formal scoping review on health system support cards. Implement Sci 2010;5:2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Boon H, Verhoef M, O'Hara D, Findlay B, Majid N. Integrative health care: arriving at a working definition. Altern Ther Health Med 2004;10(5):48–56 [PubMed] [Google Scholar]
- 8.Davis K, Drey N, Gould D. What are scoping studies? A review of the nursing literature. Int J Nurs Stud 2009;46(10):1386–400 [DOI] [PubMed] [Google Scholar]
- 9.O'Brien K, Wilkins A, Zack E, Solomon P. Scoping the field: identifying key research priorities in HIV and rehabilitation. AIDS Behav 2009;14(2):448–58 [DOI] [PubMed] [Google Scholar]
- 10.Weisser J, Morrow M, Jamer B. A critical exploration of social inequities in the mental health recovery literature. Vancouver, BC: Centre for the Study of Gender, Social Inequities and Mental Health (CGSM); 2011 [Google Scholar]
- 11.Levac D, Colquhoun H, O'Brien K. Scoping studies: advancing the methodology. Implementation Sci. 2010;69(5):1–9 [DOI] [PMC free article] [PubMed] [Google Scholar]