

Abstract
Calcified nondilatable lesions remain a challenge for the interventional cardiologist, and they are becoming more frequent in the catheterization laboratory as the overall complexity of interventions increases. Stent underexpansion is the main risk factor for restenosis and thrombosis, which is the most feared complication for the interventionalist.
In this report, we present our initial experience (8 patients) with a new noncompliant high-pressure balloon, the OPN NC balloon, a double-layered device. When we used this device at 40 atm, our rate of success was reasonable (75%) and our patients experienced no adverse sequelae. The OPN NC balloon appears to offer a new means of dilating lesions or underexpanded stents when other noncompliant balloons have failed. Safety seems reasonable, even at pressures as high as 40 atm.
Key words: Angioplasty, balloon, coronary/instrumentation/methods; balloon dilation; calcinosis/therapy; compliance; coronary stenosis/therapy; prosthesis failure; stents
Coronary calcification is a common phenomenon in coronary artery disease. In cases of significant calcification, the coronary lesion is resistant, nondistensible, and difficult to dilate.1 Calcified vessels frequently dissect during lesion preparation. In addition, the inability to fully dilate a lesion can lead to stent underexpansion, thereby increasing the risk of restenosis and the feared complication of stent thrombosis. Lesions that cannot be dilated with a balloon catheter due to their rigidity might be amenable to cutting-balloon angioplasty,2,3 scoring balloons,4 rotablators,5 or the so-called “buddy wire” technique.6 Recently, a new noncompliant balloon has become available: the OPN NC® High-Pressure PTCA Balloon (SIS Medical AG; Winterthur, Switzerland),7 which is a double-layered balloon that allows high-pressure dilation. We present 8 cases of nondilatable lesions treated with dilations at 40 atm of pressure with this balloon.
From April 2010 through April 2011, we collected all percutaneous coronary intervention (PCI) cases in which an OPN NC balloon was used at 40 atm of pressure. From a total of 965 percutaneous coronary interventions performed during that one-year period, we found in our database 8 cases of unexpandable stents, in-stent restenosis (ISR), or plaque preparation before stent implantation, out of 18 cases in which this type of balloon was used. A detailed review of each patient's history, chart, angiogram, and PCI was carried out. The registry of these 8 patients was approved by the ethics committee of our institution.
The clinical characteristics of the 8 patients in this series are presented in Table I. Their mean age was 70.25 years, and 50% of them were women. All patients were hypertensive, 6 of them were diabetic (75%), 4 had a history of previous PCI (50%), and 1 had undergone coronary artery bypass grafting. The clinical presentation was stable angina in 4 patients, unstable angina in 2, and myocardial infarction in 2. Among the angiographic characteristics (Table I), the culprit vessel was the left main coronary artery in 2 patients, the left anterior descending coronary artery (LAD) in 3, the left circumflex coronary artery in 2, and the right coronary artery in 1. All patients had some degree of calcification on the angiogram.
TABLE I. Clinical and Angiographic Characteristics
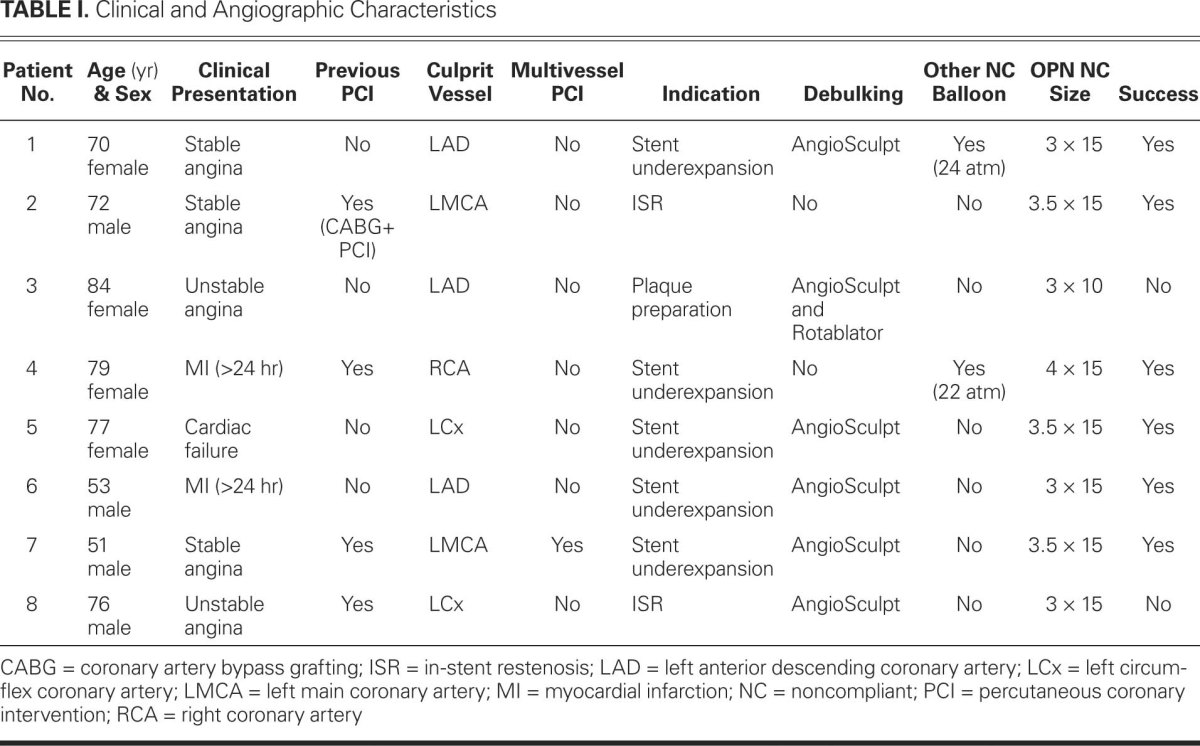
The OPN NC balloon was used for stent postdilation due to underexpansion in 5 patients, for treatment of ISR in 2 patients, and for plaque preparation before stent implantation in 1 patient. It was successful in 6 patients (75%): that is, in all of the cases of stent underexpansion and in 1 of the cases of ISR. It had an acceptable but not optimal result in the other case of ISR and did not work at all for plaque preparation. Intravascular ultrasonography was used only in the case of plaque preparation, just in order to check for dissection, because the patient could not be stented due to the impossibility of breaking the plaque.
It is important to note that in all patients the balloon was inflated at the maximal pressure possible (40 atm), precisely because that was the highest pressure possible on the inflation device. No cases of dissection, perforation, or balloon rupture were seen, and no new ST changes or cardiac-marker increases were observed after the procedure.
Patient 1 is of special interest, because her case was the first in which a pressure of 40 atm was used; it opened the way to the regular use of this technique.
Illustrative Case
A 70-year-old woman (patient 1) with exertional angina and a positive result on her exercise test underwent attempted PCI of severe proximal and mid-segment LAD lesions (Fig. 1A). Access was from the right radial artery with a 6F Medtronic Launcher® Coronary Guiding Catheter (Medtronic, Inc.; Minneapolis, Minn) Extra Back-Up 3.5. After guidewire insertion, both lesions were predilated with a 2.5 × 15-mm AngioSculpt® Scoring Balloon (AngioScore, Inc.; Fremont, Calif), and 2 drug-eluting Endeavor® Resolute stents (Medtronic) were implanted: 2.75 × 24-mm distally and 3 × 24-mm proximally (overlapping). There was a clear angiographic waist in the latter (Fig. 1B), and a suboptimal angiographic result (Fig. 1C). An attempt was made to postdilate at 30 atm of pressure with a 3.5 × 12-mm Sprinter® NC balloon (Medtronic), but it was unsuccessful (Fig. 1D). After dilation at 40 atm of pressure with a 3 × 15-mm OPN NC balloon, a good angiographic result was achieved (Fig. 1E).

Fig. 1 Patient 1. Angiograms show A) two “tandem” lesions on the left anterior descending coronary artery (anteroposterior cranial projection); B) drug-eluting stent implantation with a marked waist caused by a nondilatable calcified lesion; C) a suboptimal angiographic result after stent implantation; D) unsuccessful noncompliant-balloon dilation; and E) an optimal angiographic result after OPN NC dilation at 40 atm of pressure.
Discussion
Calcified lesions carry the risk of inadequate stent expansion because of rigidity and reduced vessel distensibility. Fibrocalcific plaques have been found to lower the degree of stent expansion.8 Rotational atherectomy has usually been considered the adequate choice for plaque preparation when dealing with highly calcified lesions, or even after balloon failure.9 This has especially been true when the operator has faced very tight lesions on small vessels; in larger vessels and in lesions that are not so tight, burrs might not be able to ablate the plaque. Although some degree of calcification was present in all of our patients, only in patient 3 was the rotablator used; in the other 7 patients, balloons were tracked to the lesion site and expanded to some extent in the predilation phase.
Other options for the preparation of fibrocalcific plaques include cutting-balloon angioplasty,10 AngioSculpt balloon angioplasty,11 the buddy-wire technique,6 and the “hugging-balloons” technique.12 In 6 of our patients, we attempted use of the AngioSculpt Scoring Balloon at a very high pressure (>25 atm), unsuccessfully. In the other 2 patients, the use of at least 1 regular balloon was attempted at high pressure.
The OPN NC balloon has been recently added to the interventionalist's armamentarium, and its usefulness in dilating lesions where other noncompliant balloons had failed has already been shown.7 It is a double-layer balloon with a very flat compliance chart.
In the report of 4 patients by Raja and colleagues,7 the OPN NC balloon was used at pressures of 35 atm in 1 patient, 30 atm in 2 patients, and 28 atm in 1 patient, all of them successfully. To our knowledge, there is no previous report on the use of the device at 40 atm, because the burst-rate pressure is 35 atm. The main finding of our registry is that the OPN NC balloon appears to be safe: no cases of dissection, perforation, or even balloon rupture were seen in our 8 patients. As in 5 of our 8 patients, the chief indication for its use appears to be post-stent dilation.
Conclusion
In conclusion, this device offers a new means of dilating lesions or underexpanded stents when other NC balloons have failed. Safety appears to be more than reasonable, even at pressures as high as 40 atm. Although larger studies must be performed before use of the OPN NC balloon at such high pressure can be recommended, our own limited initial experience has been quite favorable.
Footnotes
Address for reprints: José F. Díaz, MD, Interventional Cardiology Unit, Juan Ramon Jiménez University Hospital, Ronda Norte sn, 21004 Huelva, Spain
E-mail: jfdiazf@yahoo.es
References
- 1.Farman MT, Sial JA, Khan NU, Masood T, Saghir T. Undefeatable coronary lesion [published erratum appears in J Pak Med Assoc 2011;61(4):424]. J Pak Med Assoc 2011;61(2):185–7. [PubMed]
- 2.Bertrand OF, Bonan R, Bilodeau L, Tanguay JF, Tardif JC, Rodes J, et al. Management of resistant coronary lesions by the cutting balloon catheter: initial experience. Cathet Cardiovasc Diagn 1997;41(2):179–84. [DOI] [PubMed]
- 3.Asakura Y, Furukawa Y, Ishikawa S, Asakura K, Sueyoshi K, Sakamoto M, et al. Successful predilation of a resistant, heavily calcified lesion with cutting balloon for coronary stenting: a case report. Cathet Cardiovasc Diagn 1998;44(4):420–2. [DOI] [PubMed]
- 4.de Ribamar Costa J Jr, Mintz GS, Carlier SG, Mehran R, Teirstein P, Sano K, et al. Nonrandomized comparison of coronary stenting under intravascular ultrasound guidance of direct stenting without predilation versus conventional predilation with a semi-compliant balloon versus predilation with a new scoring balloon. Am J Cardiol 2007;100(5):812–7. [DOI] [PubMed]
- 5.Rosenblum J, Stertzer SH, Shaw RE, Hidalgo B, Hansell HN, Murphy MC, Myler RK. Rotational ablation of balloon angioplasty failures. J Invasive Cardiol 1992;4(6):312–8. [PubMed]
- 6.Lindsey JB, Banerjee S, Brilakis ES. Two “buddies” may be better than one: use of two buddy wires to expand an underexpanded left main coronary stent. J Invasive Cardiol 2007;19 (12):E355–8. [PubMed]
- 7.Raja Y, Routledge HC, Doshi SN. A noncompliant, high pressure balloon to manage undilatable coronary lesions. Catheter Cardiovasc Interv 2010;75(7):1067–73. [DOI] [PubMed]
- 8.Goldberg SL, Hall P, Almagor Y, Maiello L, Finci L, Tobis J, Colombo A. Intravascular ultrasound guided rotational atherectomy of fibro-calcific plaque prior to intracoronary deployment of Palmaz-Schatz stents [abstract]. J Am Coll Cardiol 1994;23(2s1):290A.7507504
- 9.Brogan WC 3rd, Popma JJ, Pichard AD, Satler LF, Kent KM, Mintz GS, Leon MB. Rotational coronary atherectomy after unsuccessful coronary balloon angioplasty. Am J Cardiol 1993;71(10):794–8. [DOI] [PubMed]
- 10.Karvouni E, Stankovic G, Albiero R, Takagi T, Corvaja N, Vaghetti M, et al. Cutting balloon angioplasty for treatment of calcified coronary lesions. Catheter Cardiovasc Interv 2001;54(4):473–81. [DOI] [PubMed]
- 11.Fonseca A, Costa Jde R Jr, Abizaid A, Feres F, Abizaid AS, Costa R, et al. Intravascular ultrasound assessment of the novel AngioSculpt scoring balloon catheter for the treatment of complex coronary lesions. J Invasive Cardiol 2008;20(1):21–7. [PubMed]
- 12.Feld H, Valerio L, Shani J. Two hugging balloons at high pressures successfully dilate a lesion refractory to routine coronary angioplasty. Cathet Cardiovasc Diagn 1991;24(2):105–7. [DOI] [PubMed]