

Abstract
Laparoscopic inguinal hernia repair started over two decades ago. It has been gaining ground as a mode of treatment for inguinal hernia in children. Several surgical techniques have emerged since its inception. The aim of this article is to review the role of laparoscopy in inguinal hernia repair in children, the various emerging laparoscopic surgical techniques, and their current trend in pediatric surgical practice. In this study, extensive review and analysis of recent articles on laparoscopic inguinal hernia repair in children revealed that laparoscopy plays a great role in the treatment of inguinal hernia in children. There were several emerging laparoscopic techniques, with trends toward extracorporeal suturing and knotting technique and single-port access technique as well. The recent advance is toward the use of tissue adhesives in laparoscopic inguinal hernia repair in children.
Keywords: Children, hernia, inguinal, laparoscopic, repair, technique
INTRODUCTION
Inguinal hernia is a common condition in children. The treatment for this condition is high ligation of patent processus vaginalis at the level of the internal inguinal ring. This can be achieved either by conventional open method or by laparoscopic technique.[1]
There have been conflicting reports regarding the place of laparoscopy in the treatment of inguinal hernia in children.[2] At the moment, laparoscopic inguinal hernia repair is not only possible in children, but also is gaining ground as a safe, feasible, and popular method.[3–15] There are, however, several reports comparing the conventional open method and laparoscopic inguinal hernia repair in children, but the current trend is toward laparoscopic method.[16–20]
With increasing interest in laparoscopic inguinal hernia repair, several treatment techniques have developed over the past two decades, aimed at improving the outcome.[21] The various techniques differ in their approach to the inguinal internal ring, suturing and knotting techniques, number of ports used in the procedure, endoscopic instruments used, mode of dissection of the hernia sac, and gender of the patient as well. The emerging techniques show a tendency for simple extracorporeal suturing and knotting technique, and diminished use of endoscopic ports and instruments.
The aim of this article is to review the role of laparoscopy in inguinal hernia repair in children, the various emerging laparoscopic surgical techniques, and their current trend in pediatric surgical practice.
MATERIALS AND METHODS
Literature search was performed using search engines like Google, PubMed, SpringerLink, and journals. Search for English language articles on laparoscopic inguinal hernia in children was done. Citations found in selected articles were screened and used for further references. The articles were selected based on appropriateness to the subject matter, year of publication (articles beyond 1990 were excluded), operative procedure, and institutions where the studies were conducted.
The various techniques were evaluated based: approach to the inguinal internal ring (intraperitoneal or extraperitoneal), suturing and knotting techniques (intracorporeal or extracorporeal), number of ports used (three, two, or one), instruments used, and outcome of procedure (safety, feasibility, and reproducibility).
RESULTS
There have been a lot of publications on laparoscopic inguinal hernia repair over the past two decades, based on PubMed citations on this topic. Laparoscopic inguinal hernia repair is currently employed in developed countries and developing countries as well.
The papers reviewed show that laparoscopy has a role in the treatment of inguinal hernia in children. The advantages, disadvantages, and limitations of this procedure are well highlighted in the articles.
The various laparoscopic surgical techniques for inguinal hernia repair in children cited in the review include: intracorporeal or extracorporeal, three- or single-port procedure, sac inversion and ligation in female children, resection and no ligation technique, flip-flap technique, and finally use of tissue adhesives – a current concept.
DISCUSSION
Laparoscopic inguinal hernia repair in children started over two decades ago. Initially it was doubtful whether this mode of treatment could be employed in children. This controversy lingered on until several reports established that this procedure was feasible and safe in children.[3–15] Then came the controversy between laparoscopic and conventional open surgery for inguinal hernia repair in children.[16–20]
Role of laparoscopy
The above controversies have been overtaken by events. This review establishes the fact that more and more laparoscopic inguinal hernia repairs are being carried out in children with satisfactory outcome.[22–24] Laparoscopic inguinal hernia repair has an established role in the management of this condition in children in trained hands. Indeed, it is fast becoming the gold standard for the treatment of inguinal hernia in children. The laparoscopic technique has the advantage that it is simple, feasible, and safe. Also, the contralateral internal inguinal ring and other hernia sites such as femoral, obturator, or internal hernia can be diagnosed and treated at same sitting and other occult pathologies may be diagnosed. The risk of injury to the vas deferens and cord structures in this procedure is lesser when compared to the conventional open technique.[16–19] The general advantages of laparoscopic technique such as cosmesis, low wound infection, less pain, and short hospital stay, all apply here. The disadvantages of laparoscopic technique in inguinal hernia repair in children are: it is expensive, longer duration of surgery, higher recurrence rates, and longer learning curve when compared to the conventional open method. The technique is highly limited if there is no training, and there is lack of expertise and equipment.
The issue of injury to the vas deferens and affectation of testicular vascular supply following laparoscopic surgery has been addressed. Indeed, studies by Schier and Parelkar et al. have shown that laparoscopic inguinal hernia repair in children does not affect testicular perfusion or growth.[6,13] None of the studies reviewed recorded any incidence of injury to the vas deferens.
Laparoscopic techniques
With increasing interest, there has been a proliferation of various techniques in the laparoscopic repair of inguinal hernia in children. This proliferation has been orchestrated by refinements in methods of ligation of the patent processus vaginalis at the internal inguinal ring in order to improve results and the outcome of treatment. The various techniques are: extracorporeal or intracorporeal suturing and knotting, three- or single-port procedure, sac inversion and ligation technique in girls, flip-flap technique, and use of tissue adhesives. Some studies have been highlighted in order compare the various techniques vis-à-vis the authors and their complication rates [Tables 1–3].
Table 1.
Comparison between extracorporeal and intracorporeal techniques
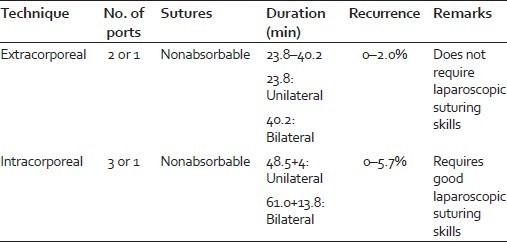
Table 3.
Comparison between three and single port (Bharathi et al. J Laparoendosc Adv Surg Tech A, 2008)[40]

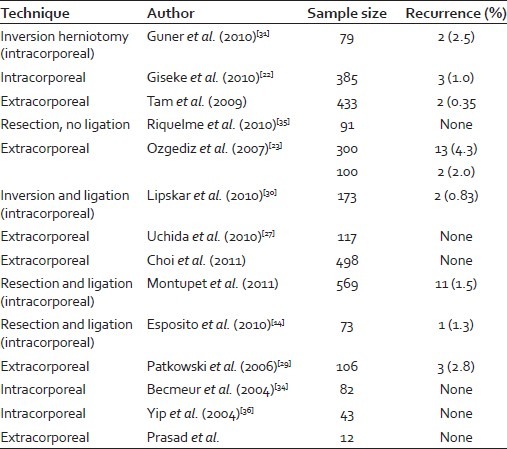
Table 2.
Various techniques by different authors and recurrence rates
Extracorporeal suturing and knotting technique
The review shows that extracorporeal technique is currently being adopted by many pediatric surgeons.[25–29] The two-port technique using nonabsorbable suture material is employed. The trend is shifting toward this technique because it is simple, safe, feasible, and reproducible. This method particularly has low recurrence rates (0–2.0%), and more importantly, knotting does not require any special skill because it is done externally in the subcutaneous tissue in the conventional manner [Table 1]. The low recurrence rate in this technique is attributed to the fact that in this procedure the sac is wholly ligated without leaving skip portions. The skip portions, especially at the medial aspect of internal inguinal ring, account for some of the recurrences in some reports.[22,28] The limitation of this technique is that special needles and introducers are required. In the review, spinal needle, special 19-guage needle, hook, and host of other instruments are currently being used with good outcome.[28]
Intracorporeal suturing and knotting technique
This was the initial method adopted at the inception of laparoscopic inguinal hernia repair in children. The technique employs three ports and uses nonabsorbable suture materials. In this method, intraperitoneal knotting is performed to close the internal inguinal ring. The closure is achieved by applying a suturing in purse-string fashion and knotting tight the internal inguinal ring. Sometimes interrupted suturing is done to close the ring.[10] This method has a high recurrence rate (0–5.7%) and is not as simple and easy as the extracorporeal technique. Here, good intracorporeal laparoscopic knotting skill is required [Table 1].
Inversion and ligation technique
This method of laparoscopic inguinal repair is widely used in female children. This is a modification of the intracorporeal technique, using three ports and nonabsorbable sutures. It is thought that inversion and ligation of sac at the internal inguinal ring would reduce the risk of recurrence (0.8–2.5%).[30–32] The problems faced in the intracorporeal technique may also apply here. In a similar manner, the selective sac extraction method for inguinal hernia repair in children by minimally invasive procedure has been described with satisfactory surgical and cosmetic outcome by Ikeda et al.[33] In the sac extraction method, the sac is extracted and ligated openly. In the inversion and ligation technique, the sac is isolated, inverted, and ligated laparoscopically.
Resection and ligation technique
This is another modification of the intracorporeal technique, with three ports and nonabsorbable sutures employed. In this technique, the hernia sac is resected and closed with a purse-string suture at the level of the internal inguinal ring. Becmeur et al. recorded no recurrence with this method.[34] This was done in an attempt to reduce the recurrence.
Resection and no ligation technique
Here, the hernia sac is resected at the level of the internal inguinal and allowed to close spontaneously. This novel technique has been reported in literature with preliminary results showing satisfactory outcome and no recurrence.[35] The method uses three ports and no sutures are employed.
Flip-flap technique
In this procedure, a flip-flap is raised in the internal inguinal ring and used to close the defect. This is a three-port technique that uses absorbable sutures. Yip et al. did not record any recurrence with this technique.[36] Satisfactory results have been noticed by Hassan et al. in a comparative study of this flip-flap technique with the conventional open technique.[37]
Three-port or single-port technique
The pioneer procedures for inguinal hernia repair in children by laparoscopy used the three-port method. Recently, with refinements in technology, the single procedure is currently attracting attention. In their experience with modified single-port laparoscopic procedures in children, Rothenberg et al. found very encouraging outcome.[38] This report corroborates with a study by Chang on technical refinements in single-port laparoscopic surgery of inguinal hernia in infants and children.[39] In a comparison study by Bharathi et al., single-port technique was preferred to the three port due to better outcome.[40] The technical difficulties encountered with the single port are a major limitation [Table 3].
Use of tissue adhesives
Initial animal experimental studies showed that tissue adhesives could be used in tissue approximation.[41] Further, experimental animal models have continued to establish the role of tissue adhesives in inguinal hernia repair.[42,43] Cusheiri in a study had earlier published an article forecasting the promising role of tissue adhesives in endosurgery.[44] Today tissue adhesive is being employed in a host of pediatric endoscopic surgeries, including inguinal hernia repair.[45]
Current trend
This review shows preference for extracorporeal technique because it is simple, safe, reproducible, and has low recurrent rates.[21] The other trend is toward the single-port technique because it results in virtually scarless abdomen as the surgical incision is hidden within the umbilicus.[38,39]
CONCLUSION
Laparoscopy plays a great role in the treatment of inguinal hernia in children. There are several emerging laparoscopic techniques in the repair of inguinal hernia in children, geared toward improving results and outcome. The current trend is toward extracorporeal suturing and knotting technique and single-port access technique as well. The future or recent advancement is the use of tissue adhesives in laparoscopic inguinal hernia repair in children.
ACKNOWLEDGMENT
I wish to express my profound gratitude to Prof. R. K. Mishra, whose teaching, inspiration, and advice enabled me to publish this article.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Brandt ML. Pediatrichernias. SurgClin North Am. 2008;88:27–43. [Google Scholar]
- 2.Rosenberg J. Pediatric inguinal hernia repair: A critical appraisal. Hernia. 2008;12:113–5. doi: 10.1007/s10029-007-0316-2. [DOI] [PubMed] [Google Scholar]
- 3.Tan HL. Laparoscopic repair of inguinal hernias in children. J PediatrSurg. 2001;36:833. [PubMed] [Google Scholar]
- 4.Holcomb GW., 3rd Diagnostic laparoscopy for congenital inguinal hernia. SeminLaparoscSurg. 1998;5:55–9. doi: 10.1177/155335069800500110. [DOI] [PubMed] [Google Scholar]
- 5.Schier F, Montupet P, Esposito C. Laparoscopic inguinal herniorrhaphy in children: A three-center experience with 933 repairs. J PediatrSurg. 2002;37:395–7. doi: 10.1053/jpsu.2002.30842. [DOI] [PubMed] [Google Scholar]
- 6.Schier F. Laparoscopic inguinal hernia repair- a prospective series of 542 children. J PediatrSurg. 2006;41:1081–4. doi: 10.1016/j.jpedsurg.2006.02.028. [DOI] [PubMed] [Google Scholar]
- 7.Kaya M, Huckstedt T, Schier F. Laparoscopic approach to incarcerated inguinal hernia in children. J PediatricSurg. 2006;41:567–9. doi: 10.1016/j.jpedsurg.2005.11.066. [DOI] [PubMed] [Google Scholar]
- 8.Chinnaswamy P, Malladi V, Jani KV, Parthasarthi K, Shetty RA, Kavalakat AJ, et al. Laparoscopic inguinal hernia repair in children. JSLS. 2005;9:393–8. [PMC free article] [PubMed] [Google Scholar]
- 9.Chan KL, Pam PK. A safe laparoscopic technique for the repair of inguinal hernias in boys. J Am CollSurg. 2003;196:987–9. doi: 10.1016/S1072-7515(03)00121-2. [DOI] [PubMed] [Google Scholar]
- 10.López Diaz M, Cano Novillo I, GarcíaVázquez A, CabezalíBarbancho D, Tejedor Sánchez R, PortelaCasalod E, et al. Laparoscopic inguinal herniorrhaphy in children. First results. Cir Pediatr. 2007;20:220–2. [PubMed] [Google Scholar]
- 11.Arbell D, Orkin B, Udassin R. Laparoscopic inguinal hernia repair in infants. Harefuah. 2007;146:745–6. [PubMed] [Google Scholar]
- 12.Turial S, Enders J, Krause K, Schier F. Laparoscopic inguinal herniorrhaphy in babies weighing 5Kg or less. SurgEndosc. 2011;25:72–8. doi: 10.1007/s00464-010-1132-9. [DOI] [PubMed] [Google Scholar]
- 13.Parelkar SV, Oak S, Gupta R, Sanghvi B, Shimoga PH, Kaltari D, et al. Laparoscopic inguinal hernia repair in a pediatric age group-experience with 437 children. J pediatrSurg. 2010;45:789–92. doi: 10.1016/j.jpedsurg.2009.08.007. [DOI] [PubMed] [Google Scholar]
- 14.Esposito C, Montinaro L, Alicchio F, Savanelli A, Armenise T, Settimi A. Laparoscopic treatment of inguinal hernia in the first year of life. J LaparoendoscAdvSurg Tech A. 2010;20:473–6. doi: 10.1089/lap.2009.0323. [DOI] [PubMed] [Google Scholar]
- 15.Oak SN, Parelkar SV, K R, Pathak R, Viswanath N, Akhtar T, et al. Large inguinal hernia in infants: Is laparoscopic repair the answer? J Laparoendosc Adv Surg Tech A. 2007;17:1148. doi: 10.1089/lap.2006.0507. [DOI] [PubMed] [Google Scholar]
- 16.SarangaBharathi R, Arora M, Baskaran V. Pediatric inguinal hernia: Laparoscopicversus open surgery. JSLS. 2008;12:277–81. [PMC free article] [PubMed] [Google Scholar]
- 17.Niyogi A, Tahim AS, Sherwood WJ, De Caluwe D, Madden NP, Abel RM, et al. A comparative study examining open inguinal herniotomy with or without hernioscopy to laparoscopic inguinal hernia repair in a paediatric population. PediatrSurgInt. 2010;20:387–92. doi: 10.1007/s00383-010-2549-x. [DOI] [PubMed] [Google Scholar]
- 18.Kuhry E, Van Veen RN, Langeveld HR, Steyerberg EW, Jeckel J, Bonjer H. Open or total extraperitoneal inguinal hernia repair? A systemic review. SurgEndosc. 2007;21:161–6. doi: 10.1007/s00464-006-0167-4. [DOI] [PubMed] [Google Scholar]
- 19.Nah SA, Glacomello L, Eaton S, de Coppi P, Curry JI, Drake DP, et al. Surgical repair of incarcerated inguinal hernia in children. Laparoscopic or open. Eur J PediatrSurg. 2011;2:8–11. doi: 10.1055/s-0030-1262793. [DOI] [PubMed] [Google Scholar]
- 20.Endo M, Watanabe T, Nakano M, Yoshida F, Ukiyama E. Laparoscopic completely extraperitoneal repair of inguinal hernia in children; a single-institute experience with 1257 repairs compared with cutdownherniotomy. SurgEndosc. 2009;23:1706–12. doi: 10.1007/s00464-008-0300-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.SarangaBharathi R, Arora M, Baskaran V. Minimal access surgery of pediatric hernia: A review. SurgEndosc. 2008;22:1751–62. doi: 10.1007/s00464-008-9846-7. [DOI] [PubMed] [Google Scholar]
- 22.Giseke S, Glass M, Tapadar P, Matthyssens L, Philippe P. A true laparoscopic herniotomy in children. Evaluation of long term outcome. J laparoendoscAdvSurg Tech A. 2010;20:191–4. doi: 10.1089/lap.2009.0069. [DOI] [PubMed] [Google Scholar]
- 23.Ozgediz D, Roayaie K, Lee H, Nobuhara KK, Farmer DL, Bratton B, et al. Subcutaneous endoscopically assisted ligation(SEAL) of the internal ring for repair of inguinal hernia in children: Report of a new technique and early results. SurgEndosc. 2007;21:1327–31. doi: 10.1007/s00464-007-9202-3. [DOI] [PubMed] [Google Scholar]
- 24.Zakehara H, Yakabe S, Kameola K. Laparoscopic percutaneous extraperitoneal closure for inguinal hernia in children: Clinical outcome of 972 repairs done in 3 pediatric surgical institutions. J PediatrSurg. 2006;41:1999–2003. doi: 10.1016/j.jpedsurg.2006.08.032. [DOI] [PubMed] [Google Scholar]
- 25.Kellnar S. Percutaneous laparoscopic hernia repair in children. ZentralblChir. 2009;134:542–4. doi: 10.1055/s-0029-1224609. [DOI] [PubMed] [Google Scholar]
- 26.Dutta S, Albanese C. Transcutaneous laparoscopic hernia repair in children: A prospective review of 275 hernia repair with minimium 2 year follow up. SurgEndosc. 2009;23:103–7. doi: 10.1007/s00464-008-9980-2. [DOI] [PubMed] [Google Scholar]
- 27.Uchida H, Kawashima H, Goto C, Sato K, Yoshida M, Takazawa S, et al. Inguinal hernia repair in children using single-incision laparoscopic-assisted percutaneous extraperitoneal closure. J PediatrSurg. 2010;45:2386–9. doi: 10.1016/j.jpedsurg.2010.08.037. [DOI] [PubMed] [Google Scholar]
- 28.Shalaby R, Ismail M, Dorgham A, Hefny K, Alsaied G, Gabr K, et al. Laparoscopic hernia repair in infancy and childhood: Evaluation of 2 different techniques. J PediatrSurg. 2010;45:2210–6. doi: 10.1016/j.jpedsurg.2010.07.004. [DOI] [PubMed] [Google Scholar]
- 29.Patkowski D, Czernik J, Chrzan R, Jawoski W, Apoznanski W. Percutaneous internal ring suturing: A minimally invasive technique for repair of inguinal hernia in children. J LaparoendoscAdvSurg Tech A. 2006;16:513–7. doi: 10.1089/lap.2006.16.513. [DOI] [PubMed] [Google Scholar]
- 30.Lipskar AM, Soffer SZ, Glick RD, Rosen NG, Levitt MA, Hong AR. Laparoscopic inguinal hernia inversion and ligation in female children: A review of 173 consecutive cases at a single institution. JPediatrSurg. 2010;45:1370–4. doi: 10.1016/j.jpedsurg.2010.02.113. [DOI] [PubMed] [Google Scholar]
- 31.Guner YS, Emami CN, Chokshi NK, Wang K, Shin CE. Inversion hernoiotomy: A laparoscopic technique for female inguinal hernia repair. J LaparoendoscAdvSurg Tech A. 2010;20:481–4. doi: 10.1089/lap.2009.0169. [DOI] [PubMed] [Google Scholar]
- 32.Zallen G, Glick PL. Laparoscopic inversion and ligation inguinal hernia repair in girls. J LaparoendoscAdvSurg Tech A. 2007;17:143–5. doi: 10.1089/lap.2006.0553. [DOI] [PubMed] [Google Scholar]
- 33.Ikeda H, Hatanaka M, Suzuki M, Fuji J, Takara K, Ishimara Y. Selective sac extraction method: Another minimally invasive procedure for inguinal hernia repair in children: A technical innovation with satisfactory surgical and cosmetic outcome. J PediatrSurg. 2009;44:1666–71. doi: 10.1016/j.jpedsurg.2009.04.017. [DOI] [PubMed] [Google Scholar]
- 34.Becmeur F, Philippe P, Lemandat-Schultz A, Moog R, Grandadam S, Lieber A, et al. A continuous series of 96 laparoscopic inguinal hernia repair in children by a new technique. SurgEndosc. 2004;18:1738–41. doi: 10.1007/s00464-004-9008-5. [DOI] [PubMed] [Google Scholar]
- 35.Riquelme M, Aranda A, Riquelme QM. Laparoscopic pediatric inguinal hernia repair: No ligation, just resection. J LaparoendoscAdvSurg Tech A. 2010;20:77–80. doi: 10.1089/lap.2008.0329. [DOI] [PubMed] [Google Scholar]
- 36.Yip KF, Tam PK, Li MK. Laparoscopic flip-flap hernioplasty: An innovative technique for pediatric hernia surgery. SurgEndosc. 2004;18:1126–9. doi: 10.1007/s00464-003-9155-0. [DOI] [PubMed] [Google Scholar]
- 37.Hassan ME, Mustafawi AR. Laparoscopic flip-flap technique versus conventional inguinal hernia repair in children. JSLS. 2007;11:90–3. [PMC free article] [PubMed] [Google Scholar]
- 38.Rothenberg SS, Shipman K, Yoder S. Experience with modified single port laparoscopic procedures in children. J LaparoendoscAdvSurg Tech A. 2009;19:695–8. doi: 10.1089/lap.2009.0148. [DOI] [PubMed] [Google Scholar]
- 39.Chang YT. Technical refinements in single port laparoscopic surgery of inguinal hernia in infants and children. DiagTherEndosc. 2010;2010:392847. doi: 10.1155/2010/392847. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Bharathi RS, Dabas AK, Arora M, Baskaran V. Laparoscopic ligationof internal ring- three port versus single port technique. Are working ports necessary? J LaparoendoscAdvSurg Tech A. 2008;18:891–4. doi: 10.1089/lap.2007.0246. [DOI] [PubMed] [Google Scholar]
- 41.Olguner M, Aktuq T, Akqur FM, Pabuccuoglu U. Experimental study investigating the feasibility of new method for laparoscopic indirect hernia repair. J InvestSurg. 1997;10:189–92. doi: 10.3109/08941939709032156. [DOI] [PubMed] [Google Scholar]
- 42.Kato Y, Yamataka A, Miyano G, Tei E, Koga H, Lane GJ, et al. Tissue adhesives for repairing inguinal hernia: A preliminary study. J LaparoendoscAdv Tech A. 2005;15:424–8. doi: 10.1089/lap.2005.15.424. [DOI] [PubMed] [Google Scholar]
- 43.Turial S, Kreutz M, Hausser S, Enders J, Schier F. CD rats as an animal model in the experimental study of laparoscopic hernia repair. Eur J PediatrSurg. 2010;20:330–3. doi: 10.1055/s-0030-1254107. [DOI] [PubMed] [Google Scholar]
- 44.Cushieri A. Tissue adhesives in endosurgery. SeminLaparoscSurg. 2001;8:63–8. [PubMed] [Google Scholar]
- 45.Esposito C, Damiano K, Settimi A, De Marco M, Maglio P, Centonze A. Experience with use of tissue adhesives in pediatric endoscopic surgery. SurgEndosc. 2004;18:290–2. doi: 10.1007/s00464-003-9032-x. [DOI] [PubMed] [Google Scholar]