

Abstract
Background and aims
Fatigue is associated with longitudinal ratings of health in patients with chronic obstructive pulmonary disease (COPD). Although the degree of airflow obstruction is often used to grade disease severity in patients with COPD, multidimensional grading systems have recently been developed. The aim of this study was to investigate the relationship between perceived and actual fatigue level and multidimensional disease severity in patients with COPD.
Materials and methods
Twenty-two patients with COPD (aged 52-74 years) took part in the study. Multidimensional disease severity was measured using the SAFE and BODE indices. Perceived fatigue was assessed using the Fatigue Severity Scale (FSS) and the Fatigue Impact Scale (FIS). Peripheral muscle endurance was evaluated using the number of sit-ups, squats, and modified push-ups that each patient could do.
Results
Thirteen patients (59%) had severe fatigue, and their St George's Respiratory Questionnaire scores were significantly higher (p < 0.05). The SAFE index score was significantly correlated with the number of sit-ups, number of squats, FSS score and FIS score (p < 0.05). The BODE index was significantly associated with the numbers of sit-ups, squats and modified push-ups, and with the FSS and FIS scores (p < 0.05).
Conclusions
Peripheral muscle endurance and fatigue perception in patients with COPD was related to multidimensional disease severity measured with both the SAFE and BODE indices. Improvements in perceived and actual fatigue levels may positively affect multidimensional disease severity and health status in COPD patients. Further research is needed to investigate the effects of fatigue perception and exercise training on patients with different stages of multidimensional COPD severity.
Keywords: BODE index, COPD, disease severity, endurance, fatigue, SAFE index
Introduction
Fatigue is the perception of mental or physical exhaustion due to exertion [1]. In addition to dyspnea, fatigue is one of the dominant symptoms that impairs exercise capacity and functional status in patients with chronic obstructive pulmonary disease (COPD), which is a slowly progressive disease characterized by irreversibly impaired pulmonary function [2]. The presence of COPD is associated with impaired muscle endurance [3]. COPD patients with increased fatigue frequently have more functional limitations [4] and worse current [2,4] and longitudinal health ratings [1].
The staging system to assess COPD severity is based on airflow obstruction and is expressed as a percentage of the predicted value for the forced expiratory volume in one second (FEV1) [5]. Studies have found that the degree of airflow limitation is closely related to mortality [6]. However, FEV1 does not reflect the systemic involvement [7] and does not provide an overall assessment of COPD severity [8]. Recently, multidimensional grading systems (BODE and SAFE indices) have been developed to assess both pulmonary and systemic manifestations of COPD. Both indices incorporate different domains quantifying the characteristics of COPD to provide a more holistic stratification of disease severity [7,8]. The BODE index includes pulmonary impairment (FEV1), symptoms (modified Medical Research Council dyspnea scale, MMRC), exercise capacity (six-minute walk test, 6 MWT) and nutritional state (body mass index). BODE index scores have been shown to correlate well with the rate of COPD hospitalization [9] and survival [7]. A newer index, the SAFE index, incorporates a standardized health-related quality of life assessment tool, St George's Respiratory Questionnaire (SGRQ), in addition to 6 MWT distance and FEV1 [8].
Despite conceptual change in COPD staging, to our knowledge no previous study has investigated whether there is an association between fatigue, a common disabling symptom, and these more holistic approaches to the measurement of COPD disease severity. Therefore, the aim of this study was to investigate the relationship between perceived and actual fatigue level and multidimensional disease severity (respiratory symptoms and systemic consequences) in patients with clinically stable COPD.
Materials and methods
Twenty-two male patients with clinically stable COPD (aged 52-74 years) took part in the study. The diagnosis of COPD, made by a pulmonologist, was based on medical history, current symptoms, and pulmonary function testing following the Global Initiative for Chronic Obstructive Pulmonary Disease (GOLD) Guidelines [5]. Subjects who had significant musculoskeletal or cardiovascular conditions were excluded. All subjects provided their written consent for the study, which was approved by the Hacettepe University Ethics Committee.
Age, gender, height, weight, time from diagnosis, and smoking history were all recorded. Body mass index was calculated as kg/m2. Subjects underwent pulmonary function testing using a spirometer (Spirolab, Medical International Research, Rome, Italy). Forced vital capacity (FVC), FEV1, peak expiratory flow rate (PEF), and forced expiratory flow between 25% and 75% of FVC (FEF25-75%) were expressed as percentages of the predicted values [10]. Dyspnea was evaluated using the MMRC dyspnea scale [11]. Exercise tolerance was assessed using the 6 MWT [12]. Quality of life was determined using the SGRQ, with total scores ranging from 1 to 100, where 100 indicates the worst health [13].
Perceived fatigue was assessed using the Fatigue Severity Scale (FSS) and the Fatigue Impact Scale (FIS). The FSS is a 9-item scale measuring the severity of fatigue. The total score ranges from 1 to 7. Scores ≥ 4 indicate severe fatigue [14]. The FIS scale is a 40-item, three-dimensional (cognitive, physical, and psychosocial function) scale measuring the effects of fatigue on daily living activities and the quality of life [15]. Scores range from 0 to 160, and a higher score reflects a greater impact of fatigue. Peripheral muscle endurance was evaluated using the number of sit-ups (trunk endurance), squats (lower extremity endurance), and modified push-ups (upper extremity endurance) that patients could do in 30 seconds [16].
Multidimensional disease severity was measured using the SAFE and BODE indices. The SAFE index consists of the SGRQ score, FEV1, and 6 MWT distance [8]. The maximum possible score is 9. The SAFE index has four stages: stage I (score 0-2), stage II (score 3-4), stage III (score 5-6), and stage IV (score 7-9). The BODE index incorporates FEV1, MMRC score, 6 MWT distance, and body mass index [7]. Scores range from 0 to 10. The BODE index has four severity stages: stage I (score 0-2), stage II (score 3-4), stage III (score 5-7), and stage IV (score 8-10). In both indices, higher scores indicate increased COPD severity.
Statistical analysis was performed using the Statistical Package for Social Sciences (SPSS) version 15.0 [17]. Data are presented as mean ± SD unless specified. To determine the relationship between disease severity and fatigue, Spearman rank correlation coefficients were used. Statistical significance was defined as a value of p < 0.05.
Results
According to the GOLD classification, 5 patients had mild COPD, 4 had moderate COPD, 6 had severe COPD, and 7 had very severe COPD. The mean time from diagnosis was 10.9 ± 7.7 years. The mean level of cigarette smoking was 46.3 ± 24.9 pack-years. Patient characteristics are presented in Tables 1 and 2. The FSS scores showed that 13 patients (59%) with COPD had severe fatigue. These patients' total SGRQ score was significantly higher than that of the patients with less severe fatigue (p = 0.030).
Table 1.
Patient Characteristics
| Variable | |
|---|---|
| Age (years) | 62.5 ± 6.5 |
| Body mass index (kg/m2) | 26.0 ± 4.4 |
| FEV1 (% pred.) | 49.7 ± 28.5 |
| FVC (% pred.) | 66.0 ± 23.9 |
| PEF (% pred.) | 56.1 ± 28.8 |
| FEF25-75% (% pred.) | 29.6 ± 23.4 |
| MMRC (0-4) | 1.82 ± 0.96 |
| 6 MWT distance (m) | 506.3 ± 128.0 |
| SGRQ (0-100) | 50.9 ± 22.3 |
| SAFE index score (0-9) | 3.7 ± 2.5 |
| BODE index score (0-10) | 2.9 ± 2.1 |
| FSS (0-7) | 4.52 ± 1.89 |
| FIS (0-160) | 32.9 ± 31.3 |
| Sit-ups (n) | 17.4 ± 6.1 |
| Squats (n) | 16.5 ± 4.6 |
| Push-ups (n) | 17.2 ± 6.9 |
Definition of abbreviations: FEF25-75%, forced expiratory flow between 25% and 75% of FVC; FEV1, forced expiratory volume in one second; FIS, Fatigue Impact Scale; FSS, Fatigue Severity Scale; FVC, forced expiratory volume in one second; MMRC, modified Medical Research Council dyspnea scale; 6 MWT, six minute walk test; PEF, peak expiratory flow rate; SGRQ, St George's Respiratory Questionnaire.
Table 2.
Individual Values for All Parameters for Each of the 22 COPD Patients
| No | Age | BMI | Time from diagnosis | Smoking history | FEV1 | FVC | FEV1/FVC | PEF | FEF25-75% | MMRC | 6 MWT | SGRQ | SAFE | BODE | FSS | FIS | Sit-ups | Squats | Push- ups |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 74 | 22.2 | 15 | 0 | 57 | 65 | 68 | 3 | 38 | 2 | 404 | 56.2 | 3 | 2 | 5.67 | 20 | - | - | - |
| 2 | 63 | 25.2 | 2 | 35 | 57 | 80 | 75.9 | 38 | 25 | 2 | 466 | 56.2 | 3 | 2 | 5.56 | 12 | - | 10 | - |
| 3 | 52 | 25.2 | 10 | 45 | 61 | 77 | 63.9 | 64 | 28 | 1 | 716 | 40.4 | 2 | 1 | 5.00 | 1 | 15 | 20 | 17 |
| 4 | 52 | 32.7 | 15 | 52.5 | 47 | 85 | 44 | 57 | 19 | 2 | 654 | 65.5 | 5 | 3 | 2.00 | 115 | 15 | 18 | 25 |
| 5 | 64 | 28.8 | 10 | 40 | 52 | 61 | 67.8 | 55 | 25 | 1 | 529 | 72.9 | 4 | 1 | 2.89 | 16 | 13 | 15 | 14 |
| 6 | 56 | 24.1 | 14 | 25 | 26 | 46 | 45 | 45 | 14 | 2 | 600 | 83.8 | 6 | 4 | 5.78 | 54 | 21 | 16 | 16 |
| 7 | 70 | 31.5 | 8 | 40 | 16 | 38 | 33.5 | 29 | 9 | 3 | 316 | 70.9 | 7 | 6 | 6.22 | 36 | - | - | - |
| 8 | 71 | 29.4 | 20 | 50 | 35 | 64 | 43.1 | 75 | 16 | 1 | 512 | 31.8 | 3 | 3 | 6.00 | 76 | 16 | 13 | 12 |
| 9 | 53 | 24.5 | 7 | 67.5 | 34 | 48 | 54.2 | 49 | 19 | 1 | 563 | 45.9 | 3 | 3 | 5.44 | 44 | 11 | - | - |
| 10 | 58 | 27.5 | 4 | 75 | 22 | 37 | 46.8 | 29 | 9 | 3 | 382 | 72.1 | 7 | 5 | 6.78 | 76 | 11 | 13 | - |
| 11 | 64 | 23.9 | 7 | 40 | 41 | 52 | 62.2 | 63 | 18 | 3 | 434 | 76.6 | 5 | 4 | 5.67 | 55 | 8 | 12 | 1 |
| 12 | 62 | 22.6 | 8 | 24 | 25 | 46 | 57 | 20 | 14 | 3 | 583 | 52.2 | 5 | 5 | 6.78 | 16 | 10 | 12 | 9 |
| 13 | 59 | 32.4 | 9 | 80 | 36 | 62 | 46.2 | 51 | 13 | 1 | 532 | 55.9 | 4 | 2 | 4.78 | 20 | - | 12 | - |
| 14 | 63 | 20.6 | 30 | 53 | 23 | 51 | 34.7 | 27 | 11 | 3 | 171 | 86.1 | 9 | 8 | 7.00 | 81 | - | - | - |
| 15 | 55 | 21.0 | 30 | 30 | 23 | 40 | 47.8 | 30 | 13 | 1 | 558 | 30.1 | 4 | 3 | 1.56 | 1 | 21 | 15 | 19 |
| 16 | 68 | 30.6 | 13 | 32 | 38 | 43 | 68.9 | 43 | 23 | 1 | 456 | 39.3 | 3 | 2 | 3.67 | 8 | 23 | 27 | 23 |
| 17 | 63 | 17.4 | 4 | 103 | 22 | 51 | 33.8 | 28 | 11 | 3 | 392 | 67.4 | 7 | 6 | 1.67 | 35 | 12 | 14 | 13 |
| 18 | 65 | 25.5 | 3 | 42 | 98 | 97 | 78.6 | 128 | 82 | 2 | 620 | 32.3 | 1 | 1 | 6.22 | 6 | 23 | 24 | 25 |
| 19 | 61 | 22.5 | 11 | 80 | 94 | 110 | 66.8 | 89 | 55 | 1 | 601 | 29.5 | 0 | 0 | 3.67 | 11 | 18 | 16 | 14 |
| 20 | 62 | 26.3 | 1 | 60 | 95 | 99 | 76.6 | 86 | 69 | 0 | 633 | 14.4 | 0 | 0 | 1.89 | 11 | 27 | 20 | 25 |
| 21 | 65 | 25.0 | 8 | 45 | 104 | 113 | 72 | 119 | 67 | 1 | 612 | 9.7 | 0 | 0 | 1.44 | 0 | 25 | 21 | 23 |
| 22 | 74 | 34.4 | 10 | 0 | 87 | 87 | 77.3 | 56 | 73 | 3 | 404 | 30.7 | 1 | 2 | 3.67 | 30 | 26 | 19 | 22 |
Definition of abbreviations: BMI, body mass index; COPD, chronic obstructive pulmonary disease; FEF25-75%, forced expiratory flow between 25% and 75% of FVC; FEV1, forced expiratory volume in one second; FIS, Fatigue Impact Scale; FSS, Fatigue Severity Scale; FVC, forced expiratory volume in one second; MMRC, modified Medical Research Council dyspnea scale; 6 MWT, six minute walk test; PEF, peak expiratory flow rate; SGRQ, St George's Respiratory Questionnaire.
Percentage of the predicted FEV1 was significantly correlated with the number of sit-ups, squats, and push-ups done (Table 3). FEV1 was also significantly associated with the total FIS score (r = -0.55), the FIS physical score (r = -0.56), FIS cognitive score (r = -0.43), and FIS psychosocial score (r = -0.52, p < 0.05). When patients were classified according to the GOLD severity classification system, the patient's GOLD stage was significantly associated with the number of sit-ups, squats and push-ups done (Table 3), and with the FSS score (r = 0.56), total FIS score (r = 0.52), FIS physical score (r = 0.54), and FIS psychosocial score (r = 0.49, p < 0.05).
Table 3.
Relationship Between Peripheral Muscle Endurance and Disease Severity Measures
| Variable | FEV1 | GOLD | SAFE | BODE | FSS | FIS |
|---|---|---|---|---|---|---|
| Sit-ups (n) | 0.59* | -0.69* | -0.68* | -0.67* | -0.43 | -0.51* |
| Squats (n) | 0.56* | -0.59* | -0.48* | -0.57* | -0.37 | -0.51* |
| Push-ups (n) | 0.56* | -0.62* | -0.43 | -0.55* | -0.37 | -0.39 |
Definition of abbreviations: FEV1, forced expiratory volume in one second; FIS, Fatigue Impact Scale; FSS, Fatigue Severity Scale; GOLD, Global Initiative for Chronic Obstructive Pulmonary Disease.
*p < 0.05.
Six patients (27.3%) were in SAFE stage I, 8 patients (36.4%) were stage II, 4 patients (18.2%) were stage III, and 4 patients (18.2%) were stage IV. The SAFE index score was significantly correlated with the number of sit-ups, number of squats, the FSS score and the total FIS score (p < 0.05, Table 3, Figure 1).
Figure 1.
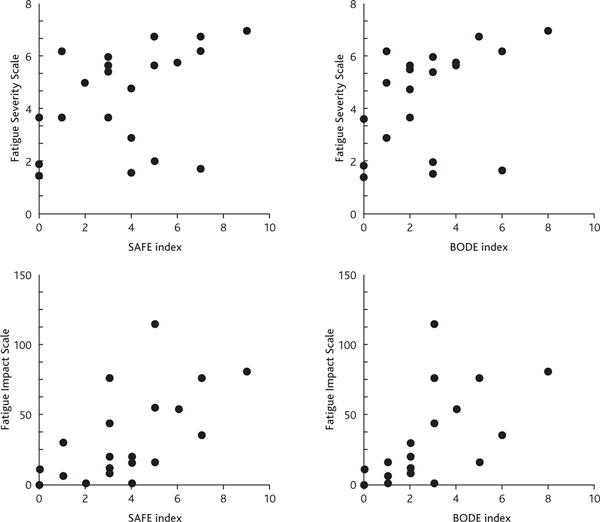
Relationship Between Multidimensional Disease Severity Indices (Bode and Safe Indices) and Perceived Fatigue Measures.
The FIS physical (r = 0.67), cognitive (r = 0.51), and psychosocial (r = 0.64) scores were also significantly associated with the SAFE index (p < 0.05). There were 11 patients (50%) in BODE stage I, 6 patients (27.3%) in stage II, 4 patients (18.2%) in stage III, and 1 patient (18.2%) in stage IV. The BODE index score was significantly correlated with the number of sit-ups, squats and push-ups; the FSS score; and the total FIS score (p < 0.05, Table 3, Figure 1). The FIS physical (r = 0.73), cognitive (r = 0.58) and psychosocial (r = 0.68) scores were also significantly associated with the BODE index (p < 0.05).
Only the FIS total and FIS physical scores were significantly correlated with the number of sit-ups (r = -0.51 and r = -0.52, respectively) and the number of squats (r = -0.51 and r = -0.56, respectively, p < 0.05).
Discussion
The findings of this study show that peripheral muscle endurance and fatigue perception are related to multidimensional disease severity measured using either the SAFE or BODE index in patients with clinically stable COPD. Physical fatigue was associated with peripheral muscle endurance.
According to previous findings, 47% to 58% of patients with COPD report fatigue everyday [18,19], and 44% of patients report that their fatigue is the worst symptom that they perceive [19]. We found that 59% of our patients had severe fatigue, suggesting that fatigue is a prevalent symptom in patients with clinically stable COPD. These patients with severe fatigue had significantly higher SGRQ scores than patients with less severe fatigue, indicating that greater perception of fatigue was associated with a greater subjective influence of the disease on the patient's quality of life [2,4]. Fatigue might play a role in the vicious circle, with more functional limitations and worse health perception [2]. Increased fatigue should be taken into account in clinical practice because fatigue has a notable impact on both current [2,4] and future [1] health ratings in patients with COPD.
In the current study, decreased FEV1 was associated with increased severity and impact of fatigue in COPD patients. We found that the physical, cognitive, and psychosocial dimensions of fatigue were affected by the severity of the airflow obstruction in our COPD patients. In previous studies, fatigue has been shown to be associated with the severity of air-flow obstruction [4,20-22]. It is likely that the increased severity of pulmonary impairment affects the subjective perception of fatigue and of every aspect of daily life in patients with mild to severe COPD. In addition to physical fatigue [22], cognitive and psychosocial fatigue might also benefit from treatments targeting airflow limitations in COPD patients.
Reduced peripheral muscle (especially trunk and lower extremity) endurance was associated with an increase in the severity of pulmonary impairment measured using FEV1. Skeletal muscle endurance has been shown to be reduced in patients with COPD [3,23,24], and it develops even in early stages of COPD [3]. Impaired quadriceps endurance is associated with the degree of airflow obstruction (i.e. FEV1) [3,23], and it is related to an increased susceptibility to peripheral muscle fatigue in patients with COPD [24]. Muscle endurance cannot be predicted from disease severity or muscle strength [24]. Therefore, muscle endurance should be measured using an appropriate apparatus [3,23,24] or field test, similar to the one used in the current study. Our results confirmed those of previous reports suggesting that peripheral muscle endurance is reduced from the early stages of disease and that it is related to the severity of the disease measured using FEV1. Peripheral muscle endurance, especially lower body and trunk endurance, was shown to be related to composite scores of disease severity. We also showed that only physical fatigue was significantly correlated with trunk and lower extremity peripheral muscle endurance. This finding is probably due to the more common use of these body parts in daily activities, such as walking, in COPD patients.
With use of two multidimensional staging systems, we showed that multidimensional disease severity measured using either the BODE or SAFE indices was associated with the severity and impact of fatigue. In a previous study investigating the factors contributing to the perception of health, Nguyen et al. showed no association between BODE index scores and fatigue. They used a 4-item one-dimensional scale [1] reflecting the general intensity and the frequency of fatigue [20]. The use of multidimensional scales has been proposed to ensure a complete description of the fatigue experience of patients [21]. Multidimensional fatigue measures seek to explore a wider experience of fatigue with the inclusion of several factors. In our study, the similarity of the correlations between actual and subjective fatigue, which are potentially modifiable factors, and the BODE and SAFE indices suggests that both indices capture the adverse effects induced by fatigue beyond the FEV1 and that both scales can be used in clinical practice. Multidimensional disease severity assessment, which addresses multiple characteristics and manifestations of COPD and its impact on function, is more informative than the severity of air flow obstruction alone.
In conclusion, we showed for the first time in the literature that peripheral muscle endurance and fatigue perception in patients with COPD is related to multidimensional disease severity measured using either the SAFE or BODE indices, which go beyond the severity of air flow limitation (i.e. FEV1). Comparison of fatigue perception in patients at different stages of multidimensional disease severity should be investigated using wider samples in each stage. Further research is also needed to investigate the effects of fatigue perception and exercise training in patients with different stages of multidimensional COPD severity. Whether improvements in perceived and actual fatigue levels may positively affect multidimensional disease severity and health status in these patients should be investigated.
Conflict of Interest Statement
None of the authors has any conflict of interest to declare in relation to the subject matter of this manuscript except Lutfi Coplu who is involved in the UPLIFT Study sponsored by Boehringer Ingelheim and Pfizer.
References
- Nguyen HQ, Donesky-Cuenco D, Carrieri-Kohlman V. Associations between symptoms, functioning, and perceptions of mastery with global self-rated health in patients with COPD: a cross-sectional study. Int J Nurs Stud. 2008;45:1355–1365. doi: 10.1016/j.ijnurstu.2007.09.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Theander K, Jakobsson P, Torstensson O, Unosson M. Severity of fatigue is related to functional limitation and health in patients with chronic obstructive pulmonary disease. Int J Nurs Pract. 2008;14:455–462. doi: 10.1111/j.1440-172X.2008.00720.x. [DOI] [PubMed] [Google Scholar]
- Coronell C, Orozco-Levi M, Méndez R, Ramírez-Sarmiento A, Gáldiz JB, Gea J. Relevance of assessing quadriceps endurance in patients with COPD. Eur Respir J. 2004;24:129–136. doi: 10.1183/09031936.04.00079603. [DOI] [PubMed] [Google Scholar]
- Breslin E, van der Schans C, Breukink S, Meek P, Mercer K, Volz W, Louie S. Perception of fatigue and quality of life in patients with COPD. Chest. 1998;114:958–964. doi: 10.1378/chest.114.4.958. [DOI] [PubMed] [Google Scholar]
- The GOLD Expert Panel. Global Strategy for Diagnosis, Management, and Prevention of COPD. http://www.goldcopd.com
- Pellegrino R, Viegi G, Brusasco V, Crapo RO, Burgos F, Casaburi R, Coates A, van der Grinten CP, Gustafsson P, Hankinson J, Jensen R, Johnson DC, MacIntyre N, McKay R, Miller MR, Navajas D, Pedersen OF, Wanger J. Interpretative strategies for lung function tests. Eur Respir J. 2005;26:948–968. doi: 10.1183/09031936.05.00035205. [DOI] [PubMed] [Google Scholar]
- Celli BR, Cote CG, Marin JM, Casanova C, Montes de Oca M, Mendez RA, Pinto Plata V, Cabral HJ. The body-mass index, airflow obstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonary disease. N Engl J Med. 2004;350:1005–1012. doi: 10.1056/NEJMoa021322. [DOI] [PubMed] [Google Scholar]
- Azarisman MS, Fauzi MA, Faizal MP, Azami Z, Roslina AM, Roslan H. The SAFE (SGRQ score, air-flow limitation and exercise tolerance) Index: a new composite score for the stratification of severity in chronic obstructive pulmonary disease. Postgrad Med J. 2007;83:492–497. doi: 10.1136/pgmj.2006.052399. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ong KC, Earnest A, Lu SJ. A multidimensional grading sys-tem (BODE index) as predictor of hospitalization for COPD. Chest. 2005;128:3810–3816. doi: 10.1378/chest.128.6.3810. [DOI] [PubMed] [Google Scholar]
- Quanjer PH, Tammeling GJ, Cotes JE, Pedersen OF, Peslin R, Yernault JC. Lung volumes and forced ventilatory flows. Report Working Party Standardization of Lung Function Tests, European Community for Steel and Coal. Official Statement of the European Respiratory Society. Eur Respir J. 1993. pp. 5–40. [PubMed]
- Savci S, Inal D, Arıkan H. Assessment of three different dyspnea scales in chronic obstructive pulmonary disease. Solunum Hastaliklari. 1997;8:355–362. [Google Scholar]
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med. 2002;166:111–117. doi: 10.1164/ajrccm.166.1.at1102. [DOI] [PubMed] [Google Scholar]
- Salepci B, Eren A, Cağlayan B, Fidan A, Torun E, Kiral N. The effect of body mass index on functional parameters and quality of life in COPD patients. Tuberk Toraks. 2007;55:342–349. [PubMed] [Google Scholar]
- Armutlu K, Korkmaz NC, Keser I, Sumbuloglu V, Akbiyik DI, Guney Z, Karabudak R. The validity and reliability of the Fatigue Severity Scale in Turkish multiple sclerosis patients. Int J Rehabil Res. 2007;30:81–85. doi: 10.1097/MRR.0b013e3280146ec4. [DOI] [PubMed] [Google Scholar]
- Armutlu K, Keser I, Korkmaz N, Akbiyik DI, Sümbüloğlu V, Güney Z, Karabudak R. Psychometric study of Turkish version of Fatigue Impact Scale in multiple sclerosis patients. J Neurol Sci. 2007;255:64–68. doi: 10.1016/j.jns.2007.01.073. [DOI] [PubMed] [Google Scholar]
- Rogers C. Exercise physiology laboratory manual. Dubuque: Wm C Brown Publishers; 1990. [Google Scholar]
- Green SB, Salkind NJ, Akey TM. Using SPSS for Windows: analyzing and understanding data. New Jersey: Prentice Hall; 2000. [Google Scholar]
- Gift AG, Shepard CE. Fatigue and other symptoms in patients with chronic obstructive pulmonary disease: do women and men differ? J Obstet Gynecol Neonatal Nurs. 1999;28:201–208. doi: 10.1111/j.1552-6909.1999.tb01985.x. [DOI] [PubMed] [Google Scholar]
- Theander K, Unosson M. Fatigue in patients with chronic obstructive pulmonary disease. J Adv Nurs. 2004;45:172–177. doi: 10.1046/j.1365-2648.2003.02878.x. [DOI] [PubMed] [Google Scholar]
- Wijkstra PJ, TenVergert EM, van der Mark TW, Postma DS, Van Altena R, Kraan J, Koëter GH. Relation of lung function, maximal inspiratory pressure, dyspnoea, and quality of life with exercise capacity in patients with chronic obstructive pulmonary disease. Thorax. 1994;49:468–472. doi: 10.1136/thx.49.5.468. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Breukink SO, Strijbos JH, Koorn M, Koëter GH, Breslin EH, van der Schans CP. Relationship between subjective fatigue and physiological variables in patients with chronic obstructive pulmonary disease. Respir Med. 1998;92:676–682. doi: 10.1016/S0954-6111(98)90517-0. [DOI] [PubMed] [Google Scholar]
- Lewko A, Bidgood PL, Garrod R. Evaluation of psychological and physiological predictors of fatigue in patients with COPD. BMC Pulm Med. 2009;9:47. doi: 10.1186/1471-2466-9-47. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Serres I, Gautier V, Varray A, Prefaut C. Impaired skeletal muscle endurance related to physical inactivity and altered lung function in COPD patients. Chest. 1998;13:900–905. doi: 10.1378/chest.113.4.900. [DOI] [PubMed] [Google Scholar]
- Vilaro J, Rabinovich R, Gonzalez-deSuso JM, Troosters T, Rodríguez D, Barberà JA, Roca J. Clinical assessment of peripheral muscle function in patients with chronic obstrutive pulmonary disease. Am J Phys Med Rehabil. 2009;88:39–46. doi: 10.1097/PHM.0b013e31818dff86. [DOI] [PubMed] [Google Scholar]