

Abstract
The purpose of this study was to characterize the mechanical demands of the lower-extremity musculature during the standing forward lunge (FL) and the standing lateral lunge (LL) exercises performed by older adults. Twenty healthy older adults (9 men, 11 women, mean age 75.0 ± 4.4 years) performed FL and LL while instrumented for biomechanical analysis. Low-er-extremity net joint moments, powers, impulse, and mechanical energy expenditure were determined using standard inverse dynamics techniques. The FL preferentially targeted the hip extensors, producing a greater flexion angle (12.8%), peak joint moment (13.6%), joint power (56.5%), and mechanical energy expenditure (25.1%). Conversely, LL targeted the ankle plantar flexors, producing greater dorsiflexion angles (19.3%), joint moments (40.9%), impulse (87.0%), and mechanical energy expenditure (61.1%). Kinetic differences at the knee were less consistent. Fitness professionals may use this information to better match the biomechanical attributes of FL and LL activities with the needs of the trainee.
Keywords: strength training, functional exercise, mechanical energy expenditure, impulse
INTRODUCTION
As our society continues to age, the preservation of physical function is a growing concern. Decreases in physical capabilities are associated with loss of functional independence; however, these decreases are often attributable to inactivity and not to underlying pathologies. To this end, resistance training may be an effective means of preserving physical function and independence in seniors.
When prescribing lower-extremity exercise for seniors, “functional” exercises (multijoint, closed-kinetic-chain, weight-bearing activities, such as the squat) are often the activities of choice because these exercises more closely approximate the movement patterns of common activities, train several muscle groups simultaneously, and require minimal specialized equipment (10). The multiplejoint characteristics of these types of activities, however, allow for an unequal distribution of the mechanical demands imposed on the ankle, knee, and hip joint musculature (5, 8, 12). In order to determine the appropriateness of a particular exercise, it is important to have an understanding of how the mechanical demand is distributed across the joints (and musculature) of the lower extremity.
When prescribing exercise activities appropriate for an older adult, a multitude of functional exercises are available, including squats, step-ups, and lunges. Both the mechanical demands and the demand distribution have been characterized during squatting (5) and step-up (12) exercises performed by seniors. Biomechanical analyses of lunging exercises, however, have been limited to a single joint (the knee) and have examined only 1 variation of the lunge (1, 11).
The standing forward lunge (FL) and the standing lateral lunge (LL) are recommended for older adults because they are relatively safe, can be performed in the home without supervision, require a minimum of equipment, and permit unilateral loading. The standing FL and LL activities are safer than stepping, walk-through, or reverse lunging activities because they do not require single-limb support. Rather, during FL and LL exercises, both feet continually remain in contact with the floor; consequently, there is a lower risk of falling. In this regard, FL and LL activities may also serve as introductory or “beginning” activities to more advanced lunging exercises.
The FL and LL exercises differ from squatting activities in that the demand is not symmetric between limbs (i.e., the greatest amount of the resistance is borne by the lead limb). Thus, FL and LL activities, performed with body weight alone, are more physically challenging than a squat. This consideration may be important when prescribing exercise for older adults—allowing for increased muscular loading without application of an external resistance. Moreover, the asymmetrical nature of these activities may be used to individually target left and right muscle groups in order to prevent bilateral substitution patterns and to correct strength differences.
Despite the potential utility of these exercise activities in preserving physical function in older men and women, the kinematic and kinetic attributes of FL and LL have not been reported. The biomechanical characterization of these and other exercise activities, however, will permit strength professionals to more appropriately and efficiently prescribe exercise for older adults by (a) identifying specific exercises that target intended muscle groups and/or “unload” muscle groups, (b) reducing the redundancy of prescribed exercises that target the same muscle groups, (c) identifying similar exercises that can be substituted to reduce overtraining and repetitive-use injuries, and (d) identifying exercises that have relatively higher/lower load and power demands. Thus, the purpose of this investigation was to compare and contrast the kinematics and kinetics of FL and LL activities within the same healthy, elder participant sample. We hypothesized that differences in hip, knee, and ankle angular excursions and joint kinetics (e.g., moments and powers) would exist between the 2 exercise activities.
METHODS
Experimental Approach to the Problem
The present study characterized the kinematics and kinetics of the both the standing FL and standing LL performed by older adults using their body mass as the sole form of resistance. Twenty subjects performed both types of lunging activities while instrumented for biomechanical analysis. The lower extremity was then modeled as 7 rigid body segments, and joint kinetics were calculated using ground reaction forces, segmental orientations and accelerations, and Newton-Euler equations. Within-subject comparisons were made to evaluate the mechanical demand on, and individual joint contributions of, the lower extremity during these exercises.
Subjects
Media advertisements were used to recruit 9 men and 11 women who were healthy, older adults (75.0 ± 4.4 years) from the greater Los Angeles area. The average height of the subjects was (1.65 ± 0.13 m), and the average weight of the subjects was (70.20 ± 14.13 kg). The subjects can be described as a relatively independent, healthy, and predominantly Caucasian group of older adults.
Prospective subjects were screened using (a) a self-administered medical history form; (b) a previously published physical activity questionnaire, Advanced Activities of Daily Living Hierarchical Exercise Scale (7); and (c) bone mineral density tests of their lumbar spine and dominant hip joint (dual-energy X-ray absorptiometry; DXA, Hologic QDR1500, Waltham, MA). Prospective subjects were disqualified for the following medical conditions: (a) musculoskeletal disorders such as osteoporosis (T-score ≤ −2.5), joint arthroplasty, current injury, pain in lower extremities or back, rheumatoid arthritis, polymyalgia rheumatica, balance disturbance, or the need for an assistive device; (b) cardiovascular disorders such as known angina or coronary heart disease, congestive heart failure, systolic blood pressure greater than 160 mm Hg, or diastolic blood pressure greater than 95 mm Hg; and (c) neurological diseases such as stroke, polio, Parkinson’s disease, dementia, or uncontrolled seizures. The purpose and methods of the investigation, along with the rights and responsibilities of each subject, were explained to all participants. Each subject provided written consent to participate in the study. The study protocol was approved by the Health Sciences Institutional Review Board of University of Southern California.
Instrumentation
Eighteen reflective markers were placed bilaterally over the following anatomical landmarks: heels, second and fifth metatarsal heads, lateral malleoli, lateral tibiae, lateral epicondyles, lateral thighs, anterior superior iliac spines, and posterior superior iliac spines. Lower-extremity kinematic data were collected using a 6-camera motion analysis system at 60 Hz (Vicon 370, Oxford Metrics, Oxford, UK). Ground reaction forces were recorded from force platforms, embedded into the floor, at 1,200 Hz (model #OR6-6-1, AMTI, Watertown, MA).
The lower body was modeled as 7 rigid bodies (2 feet, 2 legs, 2 thighs, and a pelvis) connected by frictionless pin joints. Segmental lengths were directly measured. Locations of joint centers and segmental centers of mass, along with the magnitudes of segmental centers of mass, were calculated from measured anthropometric data using published scaling factors (3, 13). Segmental orientations and accelerations were measured from the kinematic data (6), and the magnitude and location of the center of pressure was determined from the force platform data. Joint reaction forces and net joint moments at the hip, knee, and ankle were then calculated using standard inverse dynamic equations (13) and the data processing software Workstation (Oxford Metrics, Oxford, UK). These techniques have been used previously by our research team to examine multijoint lower-extremity exercises (5, 12), and they have been found to be highly reliable (ICC alphas between 0.75 and 0.95).
Exercise Protocol
Subjects were instructed in the performance of the standing FL (Figure 1) and standing LL (Figure 2) activities during their first laboratory visit, by a certified strength and conditioning specialist. For FL, subjects were instructed to maintain a shoulder-width foot position while placing their lead foot forward “as far as comfortable.” Keeping an erect posture of the trunk, subjects then flexed their lead hip and knee and dorsiflexed their ankle while lowering their body toward the floor. Subjects continued to descend until either (a) they were as low as they could comfortably go or (b) their posterior knee was within approximately 2 inches from the floor. The subjects were instructed to pause briefly in the bottom position before returning to the starting position. For LL, subjects were instructed to assume a stance approximately 1½ to 2 times their shoulder width. Keeping an erect posture, subjects flexed their lead hip and knee and dorsiflexed their ankle as they shifted their trunk laterally over the lead limb. They were instructed to lower their body as low as they could comfortably go. After a slight pause in the bottom position, subjects returned to the starting position.
Figure 1.
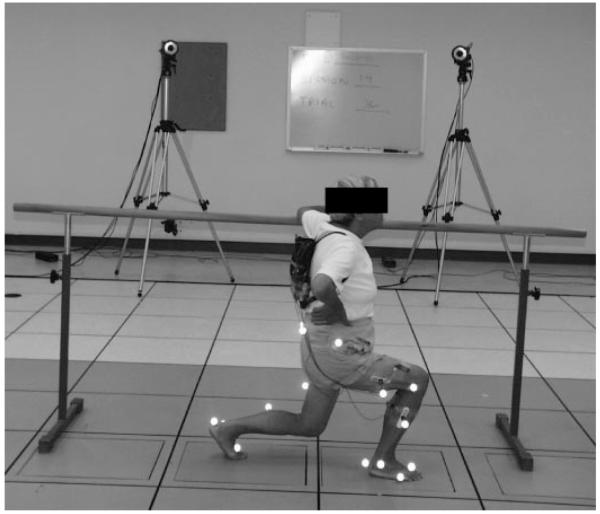
The standing forward lunge exercise, performed while the participant is instrumented for biomechanical analysis.
Figure 2.
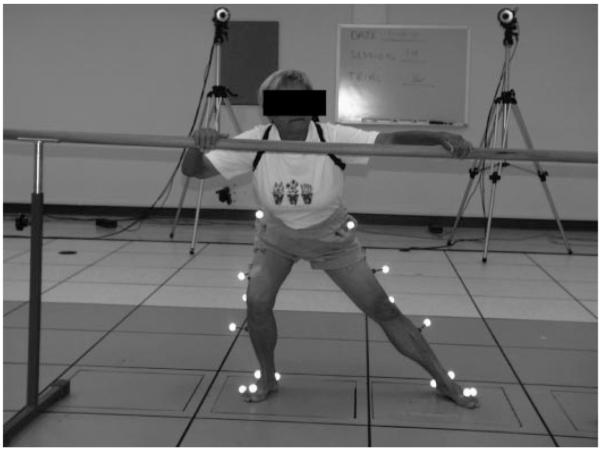
The standing lateral lunge exercise, performed while the participant is instrumented for biomechanical analysis.
The subjects practiced the modified lunging activities at home until their next laboratory visit, 1 to 2 weeks later. During their next laboratory visit, subjects were instrumented for biomechanical analysis. They performed 3 trials of both the FL and the LL activities, in a random order, at a self-selected pace and depth during a single data collection session. Data were collected on the dominant limb—the limb the participant used to kick a ball. During data collection, a safety bar was also provided to assist subjects if they lost their balance; they were instructed, however, not to use the bar to assist their movement.
Statistical Analyses
The duration of each exercise, including pause period, was quantified. Additionally, 5 dependent variables at each joint (hip, knee, and ankle) were of interest during this investigation: peak flexion angle (JA), peak net joint moment (NJM), peak net joint moment power (JP), net joint moment impulse (IMP), and mechanical energy expenditure (MEE). The JP was calculated at the dot product of the NJM and angular velocity. The largest positive (concentric muscle action) and negative (eccentric muscle action) power amplitudes were defined as the peak JP. The IMP was calculated as the integrated amplitude of the extensor moment curve (4); thus, it is a measure of both the magnitude and the duration of an activity’s mechanical demand (Figure 3). A total support impulse was calculated as the sum of the individual joint impulses. The individual joint impulses were then divided by the total support impulse in order to determine the percent contribution of each joint moment to the overall exercise. The MEE was calculated as the integrated amplitude of the absolute net joint power curve; thus, it is a measure of the total work (concentric and eccentric) produced at a joint (Figure 4). The NJM and JP were obtained for both concentric and eccentric phases, while IMP and MEE were calculated over the duration of the movements.
Figure 3.
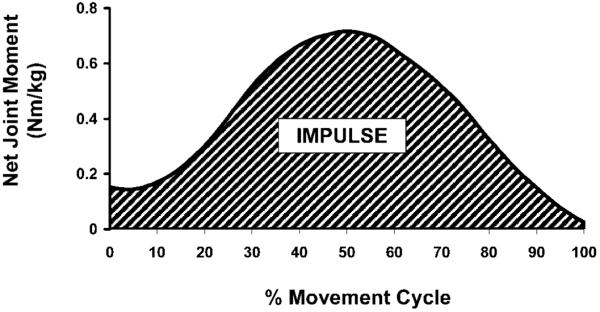
Representative net joint moment (NJM) curve, at the knee, for a single subject. A positive NJM indicates an extensor moment. The net joint moment impulse (IMPULSE) was calculated as the integrated area (striped region) under the curve.
Figure 4.
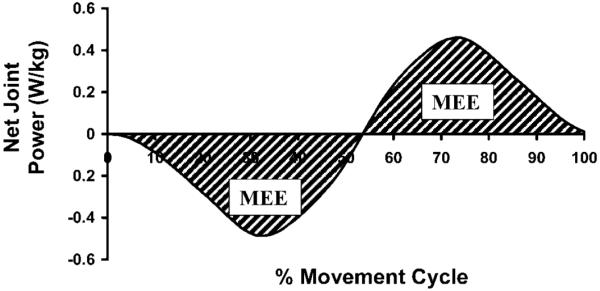
Representative net joint power (JP) curve, at the knee, for a single subject. A positive JP is indicative of power generation. A negative JP indicates power absorption. The mechanical energy expenditure (MEE) was calculated as the absolute integrated area (striped region) under the positive and negative regions of the curve.
The average values for each dependent variable, obtained over the 3 trials, were used for statistical analysis. Data was averaged across the 3 trials in order to mitigate any potential errors associated with the sampling rate or intrasubject variability. Two-factor analyses of variance (ANOVAs) (exercise × phase) with repeated measures were conducted to assess the differences in the mean values of NJM and JP between the 2 lunging conditions and movement phases. If a statistically significant interaction effect was identified with the omnibus test, post hoc, paired t-tests assessing the difference between lunging types across the ascending and descending phases were conducted. Paired t-tests were used to assess the differences in time, JA, IMP, and MEE between the 2 lunging activities at each joint. All statistical procedures were conducted using SPSS software version 10.0 (SPSS, Chicago, IL).
RESULTS
Duration
The mean (±SD) time to complete 1 repetition of LL (4.71 ± 1.51 seconds) was significantly greater (p < 0.001) than the mean time to complete 1 repetition of FL (3.74 ± 1.01 seconds).
Joint Angular Excursion
The maximum hip flexion angle obtained during FL was 12.8% greater than the angle obtained during LL (p = 0.001), and the maximum knee flexion angle was 18.8% greater than the angle obtained during LL (p < 0.001). Conversely, the maximum ankle dorsiflexion angle obtained during LL was 19.3% greater than the angle obtained during FL (p = 0.001) (Figure 5).
Figure 5.
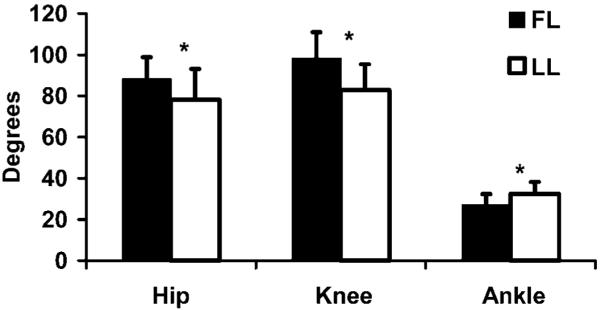
Maximum (mean ± SD) joint flexion angles, in degrees, for the forward lunge (black bars) and lateral lunge (white bars). *Statistically significant difference (p < 0.05) between FL and LL activities.
Joint Moments
Ensemble-average joint moment curves that included data from all subjects and trials were produced in order to examine the mean moment patterns generated during the lunging activities (Figures 6a-8a). For both exercises and at all 3 joints, a single peak in the joint moment occurred near the instant of maximum peak joint flexion. ANOVA identified a statistically significant main effect for lunging condition (p = 0.04) and phase (p = 0.002) among the peak hip extensor moments (Table 1). The FL produced a 13.6% greater mean peak net hip extensor moment than the LL. The ascending phase produced a 5.1% greater mean peak net hip extensor moment than the descending phase. There was not a significant interaction between activity type and phase (p = 0.84).
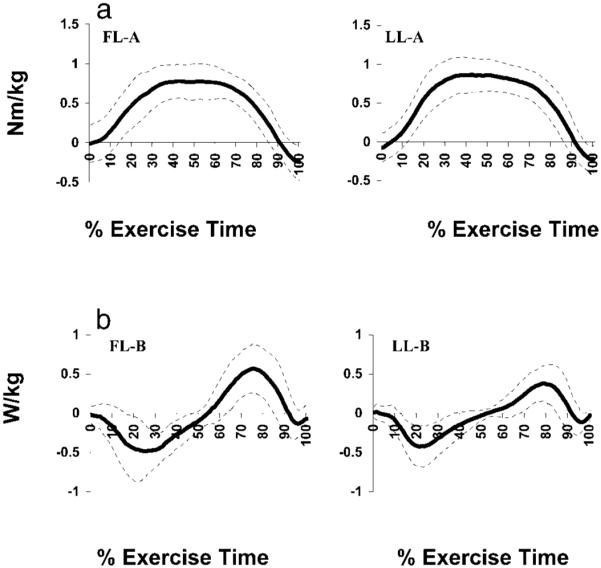
Figure 6.
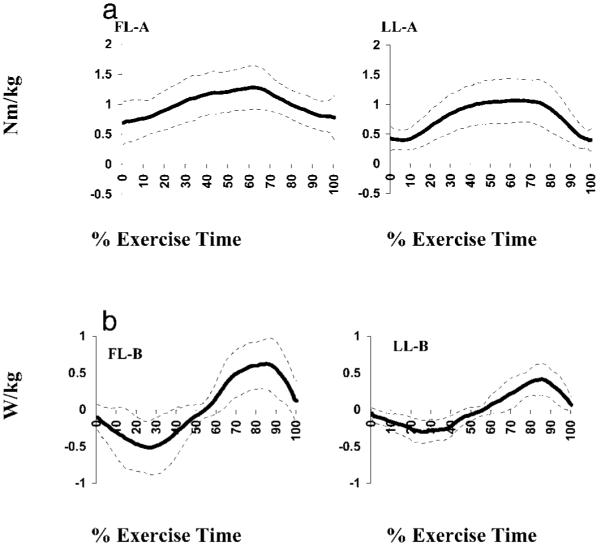
Ensemble average kinetic records for the hip during standing forward lunge (FL) and lateral lunge (LL) normalized to 100% of the movement cycle. Kinetic records include data from 20 subjects and 3 exercise trials per subject. (a) Sagittal plane moments in Nm·kg−1. (b) Power in W·kg−1.
Figure 8.
Ensemble average kinetic records for the ankle during standing forward lunge (FL) and standing lateral lunge (LL) normalized to 100% of the movement cycle. Kinetic records include data from 20 subjects and 3 exercise trials per subject. (a) Sagittal plane moments in Nm·kg−1. (b) Power in W·kg−1.
Table 1.
Peak hip, knee, and ankle joint extensor moments for standing forward lunge (FL) and standing lateral lunge (LL).
| Measurement* | FL | LL |
|---|---|---|
| Sagittal Plane | ||
| Hip Extensor Moment†,‡ | ||
| Descending | 1.25 (0.34) | 1.09 (0.33) |
| Ascending | 1.31 (0.36) | 1.15 (0.36) |
| Knee Extensor Moment†,‡ | ||
| Descending | 0.84 (0.23) | 0.93 (0.24) |
| Ascending | 0.81 (0.22) | 0.89 (0.23) |
| Ankle Plantar Flexor Moment†,‡ | ||
| Descending | 0.61 (0.17) | 0.86 (0.19) |
| Ascending | 0.63 (0.19) | 0.88 (0.19) |
| Coronal Plane | ||
| Hip Abductor Moment | ||
| Descending | −2.36 (4.82) | −1.32 (4.69) |
| Ascending | −1.72 (4.36) | −1.07 (2.83) |
All values are mean maximum peak net moments of force normalized to body mass (n·m/kg−1) of the lead limb (standard deviation).
Main effect, exercise type (p ≤ 0.05).
Main effect, phase (p ≤ 0.05).
A statistically significant main effect for lunging condition (p = 0.011) and movement phase (p < 0.001) was also identified among the peak knee extensor moments. Post hoc analysis revealed that the mean peak knee extensor moment produced with LL was 10.9% greater than that produced with FL. The mean peak knee extensor moment for the descending phase was 4.0% greater than the ascending phase. There was not a significant interaction between activity type and phase (p = 0.64).
The omnibus test also identified statistically significant main effects among the peak plantar flexor moments produced across lunging conditions (p = 0.001) and movement phases (p = 0.02). Post hoc analysis revealed that the mean peak plantar flexor moment produced with LL was 40.9% greater than that produced with the FL. The ascending phase produced a 3.0% greater mean peak plantar flexor moment than did the descending phase. There was not a significant interaction between activity type and phase (p = 0.77).
Peak Power
Ensemble average joint power curves that included data from all subjects and all trials were produced in order to examine the mean power patterns generated during the lunging activities (Figures 6b-8b). Joint power was absorbed during the descending phase (negative) and generated during the ascending phase of both activities.
A main effect difference between lunging conditions (p = 0.001) and movement phases (p = 0.004) was identified for the mean peak hip power (Table 2). Post hoc analysis revealed that the mean peak hip power produced with FL was 56.5% greater than with LL. The average peak hip power produced during ascent was 16.1% greater than that absorbed during descent. There was not a significant interaction between activity type and phase (p = 0.62).
Table 2.
Peak power at the hip, knee, and ankle for standing forward lunge (FL) and standing lateral lunge (LL).
| Measurement* | FL | LL |
|---|---|---|
| Sagittal Plane | ||
| Hip Peak Power†,‡ | ||
| Descending | 0.71 (0.41) | 0.43 (0.18) |
| Ascending | 0.79 (0.31) | 0.53 (0.21) |
| Knee Peak Power† | ||
| Descending | 0.71 (0.40) | 0.52 (0.26) |
| Ascending | 0.76 (0.35) | 0.48 (0.25) |
| Ankle Peak Power‡ | ||
| Descending | 0.17 (0.12) | 0.25 (0.21) |
| Ascending | 0.26 (0.11) | 0.34 (0.26) |
All values are absolute values of the maximum peak joint powers normalized to body mass (W·kg−1) for the lead limb (standard deviation).
Main effect, exercise type (p ≤ 0.05).
Main effect, phase (p ≤ 0.05).
A statistically significant main effect for lunging condition was also identified for mean peak knee power. Post hoc analysis revealed that the mean peak knee power generated during FL was 46.2% greater than during the LL. There was no effect for movement phase (p = 0.85); however, there was a significant interaction (p = 0.03). Post hoc analysis revealed no significant difference between movement phases for either the FL (p = 0.18) or the LL (p = 0.47). During the decent, the FL absorbed 35.64% more power at the knee than the LL (p = 0.011); during the ascent, the FL produced 57.8% more power at the knee than the LL (p < 0.001).
The omnibus test also identified statistically significant main effects among the peak ankle power produced across movement phases (p < 0.001). Post hoc analysis revealed that the mean peak plantar flexor power produced during ascent was 45.7% greater than that absorbed during descent. An apparent 38.1% greater mean ankle power with LL was not statistically significant. There was not a significant interaction between activity type and phase (p = 0.79).
Extensor Impulse
The total support impulse generated during LL was 31.2% greater than the total impulse generated during FL (p = 0.002). The extensor impulse at the hip did not differ between FL and LL; however, the knee extensor impulse was 43.9% greater during LL than during FL (p = 0.003), and the ankle plantar flexor impulse was 87.5% greater during LL than during FL (p < 0.001). The absolute values and relative contributions of the individual impulses to the overall support impulse are depicted in Figure 9.
Figure 9.

Extensor impulse at the hip, knee, and ankle, calculated as percent of the total support impulse generated during standing forward lunge (FL) and standing lateral lunge (LL). Values are extensor impulse normalized to body mass (Nm·s·kg−1) for the dominant limb (mean ± SD).
Mechanical Energy Expenditure
The MEE performed during FL at the hip was 25.1% greater than the MEE performed at the hip during LL (p < 0.05) (Figure 10). The knee MEE performed during FL was 27.0% greater than the MEE during LL (p = 0.006). Conversely, a 61.1% greater amount of MEE at the ankle was performed during LL when compared to FL (p = 0.02).
Figure 10.
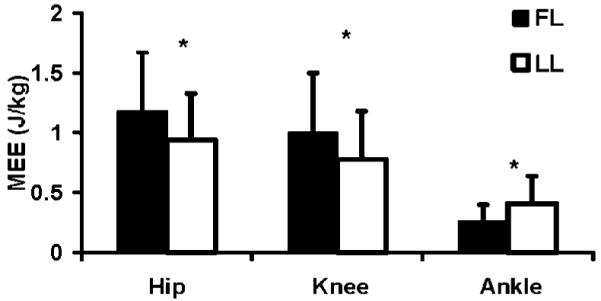
Total mechanical energy expenditure (J·kg−1) generated at the hip, knee, and ankle during the standing forward lunge (FL) and standing lateral lunge (LL). Error bars represent standard deviation of measurement. *Statistically significant difference (p < 0.05) between FL and LL activities.
DISCUSSION
This study demonstrates that FL and LL exercise activities impart different mechanical demands on the lower-extremity musculature in older adult subjects. In general, FL targeted the hip, producing greater flexion angles, and extensor NJM, JP, and MEE, whereas LL preferentially targeted the ankle plantar flexors, producing greater dorsiflexion angles, and plantar flexor NJM, IMP, and MEE. Kinetic patterns at the knee joint were more equivocal, as FL engendered greater knee flexion angles, JP, and MEE, but LL generated greater extensor NJM and IMP. These findings may be used to more effectively prescribe lower-extremity, multijoint exercise activities to restore, maintain, or improve physical function in older men and women.
Muscular strength, work, power, and physical function are associated in older adults. For example, we recently reported that lower-extremity isokinetic strength and work capacity accounted for between 41 and 54% of the variance in the performance of “higher-intensity” functional activities (stair-climb and sit-to-stand) in seniors (73.4 ± 7.3 years) (9). These relations suggest that preserving muscular strength and power may play an important role in the preservation of physical function. Nevertheless, wide-scale implementation of resistance-training programs for older men and women has been difficult because traditional programs require specialized equipment, close supervision, and often participant travel. To overcome these barriers to exercise, some have suggested that exercise for seniors should be low to moderate intensity, fun, interesting, convenient, effective, and safe (2). The FL and LL activities possess many of these qualities because (a) they can be performed in the home, (b) they do not require specialized equipment, (c) they can be performed without supervision, (d) they can be performed with varying resistance (e.g., exercise participants can use their body weight or wear a weighted vest), and (e) they can be performed relatively safely (e.g., participants can use self-spotting techniques while lightly grasping a railing or countertop). Moreover, FL and LL activities may be especially relevant exercises for older adults because they require simultaneous coordination of hip, knee, and ankle musculature.
Despite their general applicability and similar attributes, strength professionals can use kinematic and kinetic differences between FL and LL activities to specifically target intended muscle groups. For example, in older men and women with diagnosed hip extensor weakness or power deficits, FL is likely to be more effective than LL at restoring hip extensor function. Similarly, in elders with diagnosed plantar flexor weakness, LL would be a more beneficial activity.
Selecting the most appropriate exercise to restore, maintain, or improve the muscular capabilities of the knee extensors, however, requires a more sophisticated analysis because FL and LL kinetic attributes were varied. For example, LL produced a greater average NJM and IMP, while FL produced a greater average maximum knee flexion angle, JP, and MEE. Several observations can be drawn from these findings. First, the greatest average peak NJM and maximum flexion angles were produced with different exercises; thus, a larger maximum flexion angle does not necessarily result in a larger peak moment. Second, power is calculated as the dot product of the net joint moment and the angular velocity; therefore, the greater power generated and absorbed with FL can be attributed to a greater angular velocity at the knee with this activity. Third, MEE at the knee was greater with FL even though the NJM was greater with LL. The MEE is the product of the net joint moment and the angular displacement; thus, the greater MEE (i.e., work) observed with FL is due primarily to the larger average joint excursion produced with this movement. In regard to IMP, since both the magnitude (NJM) and the duration (movement time) were greater with LL, both factors contributed to the larger IMP at the knee with this exercise. These complex kinetic attributes may be used to more appropriately prescribe exercise activities for the knee extensors in elders. For example, if an increase in knee-extensor strength is the goal, practitioners should prescribe LL because LL will impart a greater muscle load over a longer time period than FL. Conversely, if an increase in knee power is the goal, FL activity is more appropriate. When prescribing exercise activities for older men and women without specific ankle, knee, or hip muscle-performance deficits, a combination of FL and LL exercises will ensure that all 3 extensor muscle groups will be targeted.
Ascending and descending phase differences were evident for both the peak joint moments and powers. These phase-dependent kinetic attributes may be important for clinicians when prescribing exercise, allowing them to adjust the resistance or provide assistance during different phases of the movement. The present data suggest that older adults are likely to have greater difficulty during the ascending phase with their hip extensors and ankle plantar flexors. Peak hip extensor moments (5.1%) and powers (16.1%) and peak plantar flexor moments (3.0%) and powers (45.7%) were greater during ascension. With this knowledge, rehabilitation specialists may instruct participants to use assistance during the ascending phase of the movements (e.g., use a handrail or sink for assistance when they experience muscle fatigue during later repetitions of an exercise set). Whenever possible, however, participants should attempt to descend without assistance, using the support only in the event of a slip or fall. At the knee, phase differences in the peak extensor moments were small but statistically significant (4.0% greater during descent), and there was no difference in the average peak power. The clinical relevance of these small, statistically nonsignificant differences, however, is not clear.
Interpretation of the findings of this investigation should be made with an appreciation of the study’s limitations. First, this study was part of a series of investigations examining the biomechanical attributes of functional exercises that may preserve physical function in older adults. Thus, our subject sample was between the ages of 70 and 85. Care should be used when attempting to extrapolate these findings to younger adults because the relative kinematics and kinetics associated with FL and LL may be age dependent. Second, this investigation was limited to the biomechanics of 2 different lunging activities performed by independent and healthy older adults. We believe, based on the subjects’ performance technique, that FL and LL required submaximal efforts and that each of our subjects had sufficient strength to perform the exercises. Nonetheless, the influence of the participants’ existing strength and/or strength-related compensation patterns were not addressed in this investigation. Future studies will need to explore the influence of these subject-specific factors. Third, in addition to the proper selection of the activities to be performed, exercise prescription must also consider the movement speed to be utilized, the number of repetitions and sets to be performed, the resistance to be applied, and the frequency of the training sessions. Because all these attributes are interrelated, changes in 1 attribute will affect others. Data from studies that systematically examine the influence of these additional considerations would further assist clinicians, therapists, and trainers when prescribing exercise programs for older adults.
PRACTICAL APPLICATIONS
Our data suggest that FL and LL impart different mechanical demands on the lower-extremity musculature in older adult subjects. There was a greater mechanical demand at the hip during FL; thus, FL is likely to be a more effective exercise for improving hip extensor function. Similarly, there was a greater mechanical demand at the ankle during LL; thus, this exercise is likely to be more effective at improving ankle plantar flexor function. Mechanical demands at the knee were more varied. The results indicate that FL generates greater mechanical energy expenditure, suggesting that this exercise targets the knee extensor musculature over a greater range of motion. The greater impulse associated with LL indicates that the knee extensor musculature is loaded for a longer time duration. These findings should be considered when prescribing exercises for older men and women—matching FL and LL biomechanical attributes with the restorative, maintenance, and/or improvement requirements of patient/client.
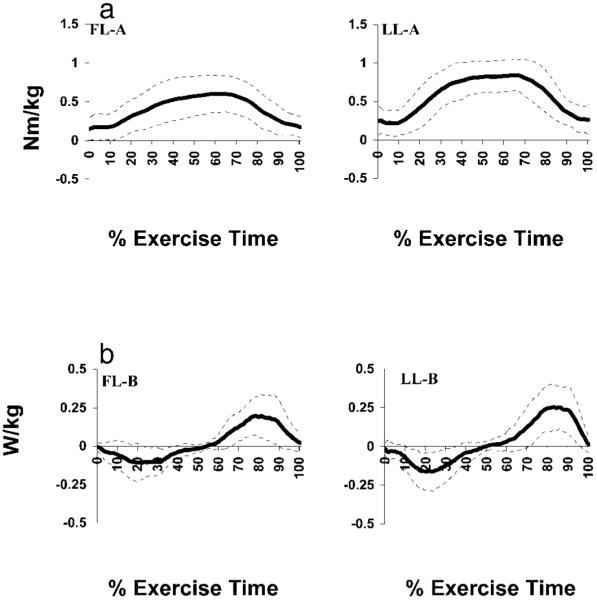
Figure 7.
Ensemble average kinetic records for the knee during standing forward lunge (FL) and standing lateral lunge (LL) normalized to 100% of the movement cycle. Kinetic records include data from 20 subjects and 3 exercise trials per subject. (a) Sagittal plane moments in Nm·kg−1. (b) Power in W·kg−1.
Acknowledgments
This research was supported by the National Institute on Aging Grant #NIA AG19320-01 and the James H. Zumberge Research Fund. The authors would like to thank Ms. Caroline Reiss, Ms. Serena Sanker, and Dr. Edward Schneider for their contributions to the project.
REFERENCES
- 1.Alkjaer T, Simonsen EB, Magnusson SP, Aagaard H, Dyhre-Poulsen P. Differences in the movement pattern of a forward lunge in two types of anterior cruciate ligament deficient patients: Copers and non-copers. Clin. Biomech. 2002;17:586–593. doi: 10.1016/s0268-0033(02)00098-0. [DOI] [PubMed] [Google Scholar]
- 2.Barry HC, Eathorne SW. Exercise and aging. Issues for the practitioner. Med. Clin. North Am. 1994;78:357–76. doi: 10.1016/s0025-7125(16)30164-x. [DOI] [PubMed] [Google Scholar]
- 3.Davis RB, Ounpuu S, Tyburski D, Gage JR. A gait analysis data collection and reduction technique. Hum. Mov. Sci. 1991;10:575–587. [Google Scholar]
- 4.Devita P, Hortobagyi T, Barrier J. Gait biomechanics are not normal after anterior cruciate ligament reconstruction and accelerated rehabilitation. Med. Sci. Sports Exerc. 1998;30:1481–1488. doi: 10.1097/00005768-199810000-00003. [DOI] [PubMed] [Google Scholar]
- 5.Flanagan S, Salem GJ, Wang MY, Sanker SE, Greendale GA. Squatting exercises in older adults: Kinematic and kinetic comparisons. Med. Sci. Sports Exerc. 2003;35:635–643. doi: 10.1249/01.MSS.0000058364.47973.06. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Kadaba MP, Ramakrishnan HK, Wooten ME. Measurement of lower extremity kinematics during level walking. J. Orthop. Res. 1990;8:383–392. doi: 10.1002/jor.1100080310. [DOI] [PubMed] [Google Scholar]
- 7.Reuben DB, Siu AL. An objective measure of physical function of elderly outpatients. The Physical Performance Test. J. Am. Geriatr. Soc. 1990;38:1105–12. doi: 10.1111/j.1532-5415.1990.tb01373.x. [DOI] [PubMed] [Google Scholar]
- 8.Salem GJ, Salinas R, Harding V. Bilateral kinematic and kinetic analysis of the squat exercise after anterior cruciate ligament reconstruction. Arch. Phys. Med. Rehabil. 2003;84:1211–1216. doi: 10.1016/s0003-9993(03)00034-0. [DOI] [PubMed] [Google Scholar]
- 9.Salem GJ, Wang MY, Young JT, Marion M, Greendale GA. Knee strength and lower- and higher-intensity functional performance in older adults. Med. Sci. Sports Exerc. 2000;32:1679–1684. doi: 10.1097/00005768-200010000-00003. [DOI] [PubMed] [Google Scholar]
- 10.Stone MH, Collins D, Plisk S, Haff G, Stone ME. Training principles: Evaluation of modes and methods of resistance training. Strength Cond. J. 2000;22:65–76. [Google Scholar]
- 11.Stuart MJ, Meglan DA, Lutz GE, Growney ES, An KN. Comparison of intersegmental tibiofemoral joint forces and muscle activity during various closed kinetic chain exercises. Am. J. Sports Med. 1996;24:792–799. doi: 10.1177/036354659602400615. [DOI] [PubMed] [Google Scholar]
- 12.Wang MY, Flanagan SP, Song JE, Greendale GA, Salem GJ. Lower extremity biomechanics during forward and lateral stepping activities in older adults. Clin. Biomech. 2003;35:635–643. doi: 10.1016/s0268-0033(02)00204-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Winter DA. Biomechanics and Motor Control of Human Movement. John Wiley & Sons; New York: 1990. [Google Scholar]