

Abstract
Purpose
We conducted a phase I study of dasatinib, an oral SRC-family tyrosine kinase inhibitor, in combination with paclitaxel and carboplatin in advanced and recurrent epithelial ovarian cancer.
Experimental Design
The primary objective was to determine the maximum tolerated dose (MTD). Secondary objectives included defining toxicity, response rate (RR), pharmacokinetics and pharmacodynamics. Using a “3+3” design, cohorts of 3–6 patients received paclitaxel (175 mg/m2) and carboplatin (AUC 6) every three weeks with escalating doses of dasatinib (100, 120, 150 mg daily), followed by an 8 patient expansion cohort.
Results
Twenty patients were enrolled between 06/07 and 12/09. The median age was 61 years (42–82) with a median of 2 prior regimens (0–6), and 71% had platinum-sensitive disease. There were 3–6 patients in each cohort, and 8 in the expansion cohort. Pharmacokinetics were observed over the first 2 cycles of therapy. One DLT was observed in the 100 mg dasatinib cohort (grade 3 myalgia). Other toxicities in all cycles included neutropenia (95% grade 3–4; 91% in the 150 mg dosing cohort), thrombocytopenia (35% grade 3–4), and fatigue (10% grade 3). The RR was 40% (3 complete responses, (15%); 5 partial responses, (25%)),10 (50%) had stable disease, and 2 were not evaluable. The PFS6-month actuarial estimate was 86%. The median PFS and OS were 7.8 and 16.2 months, respectively.
Conclusions
Due to the high incidence of myelosuppression with subsequent cycles the recommended phase II dose of dasatinib is 150 mg daily in combination with paclitaxel and carboplatin. The combination was safe with evidence of clinical activity.
Keywords: dasatinib, chemotherapy, ovarian cancer
Introduction
In 2008 there were an estimated 225,500 new cases of epithelial ovarian cancer diagnosed worldwide, with 140,200 deaths from this disease.1 Despite cytoreductive surgery and platinum/taxane first-line therapy,2 remissions are infrequently durable and the majority of patients will relapse.3 Treatment of recurrent disease offers some prolongation of survival,4 but most patients ultimately succumb to chemorefractory disease. Although biological agents have not had a major impact on the treatment of ovarian cancer thus far, SRC inhibitors are among the most promising classes of agents.
SRC kinase deregulation leads to increased activation of cell migration, proliferation, survival, invasion, and angiogenesis.5,6 The SRC pathway has been found to be frequently dysregulated in solid tumors, including ovarian cancers.5,7,8 SRC activity increases chemotherapy resistance via activation of RAS and AKT,2 and SRC inhibition has been associated with reversal of chemoresistance in ovarian cancer cells.3 Inhibition of SRC has been shown to enhance the cytotoxicity of both paclitaxel and cisplatin in ovarian cancer cell lines.3,4 SRC inhibition enhances paclitaxel mediated cytotoxicity through activation of caspase-3 and may restore paclitaxel sensitivity by reducing the intracellular concentration of paclitaxel needed for tubulin stabilization.3,5 In vivo studies have shown that SRC inhibition, by antisense Src constructs or pharmacologic measures, resulted in decreased tumor growth and enhanced taxane activity.6,7
We previously reported synergistic and additive activity when the Src-family inhibitor, dasatinib, was combined with both paclitaxel and carboplatin in ovarian cancer cell lines.11 Dasatinib is a tyrosine kinase inhibitor that inhibits the SRC family kinases as well as BCR-ABL, DDR2, c-KIT, EPHA kinases, PDGFβ and others.8 In view of these promising preclinical findings, we sought to determine the maximum tolerated dose (MTD) of dasatinib in combination with paclitaxel and carboplatin in patients with epithelial ovarian cancer.
PATIENTS AND METHODS
Study Design
The study was designed as a multicenter open-label phase I study of combination dasatinib, paclitaxel, and carboplatin in women with advanced or recurrent epithelial ovarian cancer. Patients with peritoneal and tubal cancers were also enrolled given the similarities in histology. Enrollment began in June 2007 and the study closed to enrollment in December 2009. Approval was obtained from the Duke University and Moffitt Cancer Center Institutional Review Boards. The trial was registered in the National Institutes of Health clinical trials database (NCT00672295).
Eligibility
Eligible patients must have had histologic or cytologic evidence of advanced (stage III or IV) or recurrent epithelial ovarian, peritoneal, or tubal cancer. Patients may have had prior cytotoxic chemotherapeutic regimens including prior treatment with carboplatin and paclitaxel. All patients must have had measurable disease; age ≥ 18 years; performance status of 0 to 2; absolute neutrophil count (ANC) ≥ 1500/mm3; platelets ≥ 100,000/mm3; creatinine ≤ 1.5 times the upper limit of normal (ULN); bilirubin ≤ 1.5 ULN; SGOT and alkaline phosphatase ≤ 2.5 ULN; and neuropathy ≤ grade 1. Patients provided written informed consent. Patients with a prolonged QTc interval on pre-entry electrocardiogram (> 450 msec), taking anticoagulants or medications that inhibit platelet function, serious concurrent medical illness, significant cardiac disease, pre-existing pleural effusions greater than ¼ of the lung field, or clinically significant ascites were excluded.
Drug Administration
The study used dasatinib provided by Bristol-Myers Squibb. Paclitaxel and carboplatin are commercially available Food and Drug Administration (FDA) approved drugs. Participants were considered for 4 planned dose levels of dasatinib 100mg, 120 mg, 150 mg, and 200 mg orally in combination with paclitaxel 175 mg/m2 intravenous (IV) infusion and carboplatin (AUC 6 mg/ml/min/IV) on day 1 of each 3 week cycle (Table 1). Dasatinib was administered continuously on days 2–21 in the first cycle of therapy and continuously (days 1–21) throughout the remainder of therapy. Dasatinib was not administered on day 1 of cycle one in order to obtain pharmacokinetic parameters for paclitaxel alone. On the day of coadministration of dasatinib with paclitaxel 175 mg/m2 IV dasatinib was dosed 2 hours post-initiation of the paclitaxel infusion.
Table 1.
Dosing Cohorts
| Treatment Cohort | Patients | Study Drug | ||
|---|---|---|---|---|
| N | Dasatinib mg | Paclitaxel (mg/m2) | Carboplatin (AUC) | |
| Cohort 1 | 6 | 100 | 175 | 6 |
| Cohort 2 | 3 | 120 | 175 | 6 |
| Cohort 3 | 11 | 150 | 175 | 6 |
| Cohort 4 | 0 | 200 | 175 | 6 |
Study Parameters
Patients were evaluated prior to randomization and every cycle. The baseline valuation was performed within 14 days prior to the first dose of study drug(s) and included a medical history; physical examination; CA-125; EKG; and laboratory assessment of bone marrow function and blood chemistries. Within 28 days prior to the first dose of study drug(s), baseline disease status was documented by imaging. Physical examination, chemistries, toxicity assessment, and CA-125 were performed prior to every cycle, and a complete blood count was obtained weekly. Radiologic assessments were performed every 6 weeks. Patients continued to receive study drugs until their disease progressed, unacceptable toxicity occurred, or consent was withdrawn.
Patients must have received a minimum of 2 cycles to be evaluable for efficacy. Response was based on Response Evaluation Criteria in Solid Tumors (RECIST 1.0).9 The safety analyses included all patients who received at least one dose of study drug(s). Toxicity was graded using the Common Terminology Criteria for Adverse Events (CTCAE (Version 3.0)).
Treatment Modifications
Initial treatment modifications consisted of cycle delay and/or dose reduction. The use of hematopoietic cytokines and protective reagents were restricted unless the patient experienced recurrent neutropenic complications after treatment modifications. Treatment decisions for hematologic toxicity were based on the ANC and platelet count. Subsequent cycles of therapy were not administered until the ANC was ≥ 1500 cells/mm3 (CTCAE v3.0 grade 1) and the platelet count was ≥ 75,000/ul. Therapy could be delayed for a maximum of two weeks. However, therapy with dasatinib was resumed when the ANC ≥ 1000 and platelets ≥ 50,000/mm3 during this delay period. Patients who failed to recover adequate counts after a two-week delay were removed from study.
Patients who experienced febrile neutropenia, grade 4 neutropenia ≥ 7 days, symptomatic grade 3 thrombocytopenia, grade 4 thrombocytopenia, ≥ grade 2 renal toxicity, ≥ grade 3 hepatic toxicity, and/or ≥ grade 3 other pertinent non-hematologic toxicity underwent a one dose level reduction (paclitaxel dose level -1: 150 mg/m2; carboplatin dose level -1: AUC 5) for subsequent cycles. For recurrent febrile neutropenia, and/or grade 4 neutropenia persisting ≥ seven days (after initial dose reduction), prophylactic growth factors were administered starting the day after chemotherapy. Patients with recurrent symptomatic grade 3 thrombocytopenia and/or grade 4 thrombocytopenia underwent another dose level reduction (paclitaxel dose level -2: 135 mg/m2; carboplatin dose level -2: AUC 4) for subsequent cycles. Patients experiencing grade 2 neurotoxicity underwent a one dose level reduction (paclitaxel dose level -1: 150 mg/m2). While those with ≥ grade 3 neurotoxicity were held for a maximum of 2 weeks until recovery to ≤ grade 1 and treatment was resumed with a one dose level reduction of paclitaxel. Participants who required more than 2 dose reductions or toxicity-related delays greater than 3 weeks were removed from the study.
Dasatinib was continued except in the setting of select hematologic parameters, pleural effusions, and cardiac toxicity. In the event of grade 4 neutropenia or grade 3 thrombocytopenia based on day 8 and 15 interval counts, dasatinib was held until ANC ≥ 1000/mm3 and platelets ≥ 50,000/mm3. Treatment was resumed with dasatinib at the original starting dose. If platelets < 25,000/mm3 and/or recurrence of ANC < 500/mm3 for > 7 days dasatinib was held until the appropriate counts were obtained. There were no dose reductions for dasatinib. Dasatinib could be resumed or the patient removed from protocol at the investigator’s discretion. The protocol included management instructions in the event of a new or worsening ≥ grade 1 pleural effusion and/or prolonged QTc intervals.
Pharmacokinetic Evaluation
Pharmacokinetic evaluation was performed for dasatinib and paclitaxel because both are metabolized in liver by CYP3A4 and have demonstrated respective inhibitory potential for CYP3A4. Pharmacokinetic evaluation was not conducted for carboplatin. Carboplatin undergoes spontaneous hydrolysis to the active compound and is excreted renally. Carboplatin would not be expected to have a pharmacokinetic drug interaction with either dasatinib or paclitaxel.
Samples were collected from a peripheral vein using vacutainers containing potassium ethylenediaminetetraacetic acid (K3 EDTA) as the anticoagulant. Blood samples (3 mL) for the analysis of dasatinib in plasma were collected at: pre-dose (0 h), 0.5, 1, 2, 3, 4, 6, 8, 10 and 24 h post-dosing on Day 15 of Cycle 1 (dasatinib alone) and Day 1 of Cycle 2 (dasatinib in combination with paclitaxel). Blood samples (3 mL) for the analysis of paclitaxel and its metabolite in human plasma were collected at: pre-dose (0 h), 1.5, 3 (immediately prior to end of infusion), 3.25, 3.5, 4, 5, 6, 8, 10, 24, and 48 h post-dosing on Day 1 of Cycle 1 (paclitaxel alone) and Day 1 of Cycle 2 (paclitaxel in combination with dasatinib). Plasma was isolated from patients’ whole blood for pharmacokinetic measurements on dasatinib and paclitaxel by centrifugation at 2000g for 5 minutes at 4 °C, and stored frozen at −20°C.
Dasatinib, paclitaxel, and the 6-OH metabolite of paclitaxel were assayed using a validated liquid-chromatography tandem mass spectrometry method (Bristol-Myers Squibb Company).10 The parameters for dasatinib were the maximum observed plasma concentration (Cmax), the time of Cmax (Tmax), the area under the plasma concentration-time curve from time zero to the last time of the last quantifiable concentration (AUC (0-T)), the AUC-time curve within the dosing interval (TAU = 24 h) (AUC(TAU)), and the plasma half-life (T-HALF). Due to different dose levels in subjects, concentration levels of dasatinib were dose normalized to 100 mg.The pharmacokinetic parameters of paclitaxel and its metabolite included: Cmax, AUC (0-T), the AUC-time from time zero to infinity (AUC(INF)), and plasma half-life. Additional parameters for paclitaxel included the mean residence time adjusted for infusion time (MRT(INF)), total body clearance, and volume of distribution at steady state (Vss). For 6-OH paclitaxel the metabolite to parent ratio based on dose normalized AUC(INF) was calculated. The Cmax and Tmax were obtained from experimental observations. Using no weighting factor, the terminal log-linear phase of the concentration-time curve was identified by least-square linear regression of at least 3 data points that yielded a maximum G-criteria, which is also referred to as adjusted R-squared. The T-HALF was calculated as Ln2/Lz, where Lz is the absolute value of the slope of the terminal log-linear phase. AUC values were calculated using the mixed log-linear trapezoidal algorithm in Kinetica™ 4.2 in the eToolbox (version 2.4; Thermo Electron Corp., Philadelphia, PA).
Gene Expression Microarray Pre-processing and Analysis
RNA was prepared per NCI protocol.11 Expression estimates for the Affymetrix U133A v2 GeneChips were obtained by robust multi-array average (RMA then log2 transformed).12 Based on measures of RNA degradation (3′/5′ ratios of AFFX control genes) and global principal component plots (22,215 total probesets), outlier samples of poor quality were removed prior to analysis. Differential expression at the gene-level was evaluated between patients identified as complete or partial responders versus stable disease (SD) using Limma13, and the Benjamini-Hochberg correction to estimate false-discovery rates (FDR).14 Although the sample size was too small for robust pathway analyses, patterns of differential expression were evaluated for the SRC pathway signature15 (applied as described in Gatza et al.16) and gene sets reported by Konecny17 and Huang18, using heatmaps with hierarchical clustering and SAFE plots.19 All microarray pre-processing, analyses and graphical images were generated in R version 2.9 GenePattern.20
Statistical Considerations
The primary endpoint was to determine the MTD of dasatinib in combination with paclitaxel and carboplatin during the first cycle of treatment. The dose escalation followed a “3+3” design, where up to 3 additional patients were enrolled at any dose level where a dose limiting toxicity (DLT) was noted. No intrapatient dose escalation was permitted and dose reductions were permanent. After each cohort of 3 patients enrolled, a minimum of 1 cycle (3 weeks) observation period was required to assess for DLTs before starting enrollment at the next higher dose level combination. The recommended Phase II dose (RP2D) was to be defined as the dose where 1 or fewer of 6 treated patients at a dose level experienced a DLT during the first treatment cycle. In order to confirm that the selected dose level was appropriate, a confirmatory cohort of 8 additional subjects was enrolled.
DLT was defined as non-hematologic or greater than expected hematologic toxicity (assessed according to CTCAE v3.0). Non-hematologic DLT was defined as grade 3 or greater non-hematologic toxicity (specifically diarrhea, rash, non-malignant pleural effusion, and ascites not attributable to malignancy). Fatigue, hypersensitivity reaction, nausea, and vomiting that are medically controlled would be exempt from the definition of DLT. Hematologic DLT was defined as either grade 4 thrombocytopenia, neutropenic fever, or neutropenia > 7 days duration, dose delay of greater than 2 weeks due to failure to recover counts to ≤ grade 1, and grade 3 or 4 non-surgical hemorrhage. Patients who were considered evaluable for MTD determination were those who had received any study treatment.
Secondary endpoints included toxicity, response rate (RR), and progression-free survival > 6 months (PFS6-month). The number and percent of patients achieving complete (CR) and partial response (PR) were summarized. PFS was defined as the time from trial registration until first recurrence or death, whichever occurred first, and for patients without an event, censored at the last follow-up date. Overall survival (OS) was defined as time from trial registration until death and for patients still alive it is censored at date of last follow-up. PFS and OS were estimated using the Kaplan-Meier method.
Role of the Funding Source
This was an investigator initiated study supported by Bristol-Myers Squibb US, New Jersey. The study was independently managed and analyzed. The final responsibility for the manuscript and the decision to submit for publication was made by the investigators.
RESULTS
Patient Characteristics
Twenty patients were enrolled including 8 in the confirmatory cohort. The median age was 61 years (42–82). Most patients had received previous chemotherapy, with a median number of 2 prior regimens (range, 0–6). Seventy-one percent had platinum-sensitive disease defined as a treatment-free interval greater than 6 months after platinum-therapy. Table 2 summarizes the patient demographics.
Table 2.
Baseline Demographic Characteristics
| Characteristic | N=20 n (%) |
|---|---|
|
| |
| Age | Median 61 (range: 42–82) |
|
| |
| Prior Therapies | Median 2 (range: 0–6) |
|
| |
| Primary | |
| Fallopian Tube | 2 (10) |
| Ovarian | 18 (90) |
| Peritoneal | - |
|
| |
| Race | |
| African-American | 2 (10) |
| Caucasian | 18 (90) |
| Hispanic | - |
|
| |
| Performance Status | |
| 0 | 16 (80) |
| 1 | 3 (15) |
| 2 | 1 (5) |
|
| |
| Initial Stage | |
| I | 1 (5) |
| II | 1 (5) |
| III | 15 (75) |
| IV | 3 (15) |
|
| |
| Histology | |
| Adenocarcinoma, unspecified | 4 (20) |
| Endometrioid | 1 (5) |
| Serous | 14 (70) |
| Transitional Cell | 1 (5) |
|
| |
| Platinum-free Interval1 | |
| < 6 months | 5 (29) |
| ≥ 6 months | 12 (71) |
3 patients had chemonaive disease
Pharmacokinetics
The pharmacokinetic parameters for dasatinib, paclitaxel and 6-OH paclitaxel are displayed in Table 3 and Figure 1. The Cmax, AUC(0-T), and AUC(TAU) for dasatinib were minimally lower after co-administration of paclitaxel. On Cycle 1, Day 15 and Cycle 2, Day 1, the values for Cmax were 129 ng/mL and 78 ng/mL, respectively, with high interpatient variability. Geometric means for AUC(0-T), and AUC(TAU) of dasatinib were slightly reduced by 11% (469 ng*hour/mL to 415 ng*hour/mL), and 13% (478 ng*hour/mL to 415 ng*hour/mL) respectively, at second assessment time. The mean terminal T-half (standard deviation [SD]) were 6.17 hours (2.32 hours) and 5.27 hours (1.26 hour) at the two assessment times, a non-significant difference.
Table 3.
Pharmacokinetic parameters of dasatinib, paclitaxel, and 6-OH paclitaxel.
| A. Summary of pharmacokinetic parameters for dasatinib.
| |||
|---|---|---|---|
| Parameters | Treatment | ||
| Dasatinib alone (N=14) | Paclitaxel and dasatinib (N=18) | ||
| Cmax (ng/mL) | Geo Mean (%CV) | 129 (57) | 78 (88) |
| AUC(0-T) (ng•h/mL) | Geo Mean (%CV) | 469 (41) | 415 (63) |
| AUC(TAU) (ng•h/mL) | Geo Mean (%CV) | 478 (43) | 415 (63) |
| Tmax (h) | Median (min, max) | 2.00 (0.50, 6.00) | 2.00 (0.50, 6.00) |
| T-HALF (h) | Mean (SD) | 6.17 (2.32) | 5.27 (1.26) |
| B. Summary of pharmacokinetic parameters for paclitaxel and 6-OH paclitaxel.
| |||||
|---|---|---|---|---|---|
| Parameters | Treatment | ||||
|
| |||||
| Paclitaxel | 6-OH Paclitaxel | ||||
| Paclitaxel alone (N=20) | Paclitaxel and Dasatinib (N=18) | Paclitaxel alone (N=20) | Paclitaxel and Dasatinib (N=18) | ||
| Cmax (ng/mL) | Geo Mean (%CV) | 4824 (37) | 3907 (23) | 349 (44) | 260 (58) |
| AUC(0-T) (ng•h/mL) | Geo Mean (%CV) | 15662 (28) | 13338 (25) | 732 (53) | 562 (68) |
| AUC(INF) (ng•h/mL) | Geo Mean (%CV) | 16088 (28) | 13761 (26) | 771 (53) | 615 (68) |
| T-HALF (h) | Mean (SD) | 11.7 (1.6) | 11.7 (3.8) | 1.26 (0.75) | 0.94 (0.47) |
| MRT(INF) (h) | Mean (SD) | 6.7 (1.5) | 6.9 (2.1) | - | - |
| CLt (L/h) | Mean (SD) | 20.9 (6.3) | 24.3 (6.0) | - | - |
| Vss (L) | Mean (SD) | 140.5 (52.3) | 163.4 (50.4) | - | - |
| M/Pa | Mean (SD) | - | - | 0.06 (0.04) | 0.05 (0.02) |
The parameters are dose-normalized to 100 mg of dasatinib, assuming dose proportionality.
The parameters are dose-normalized to 175 mg/m2, assuming dose proportionality.
Cmax, maximum observed plasma concentration; Tmax, time of maximum observed plasma concentration; AUC(0-T), area under the plasma concentration-time curve from time zero to the last time of the last quantifiable concentration; AUC(TAU), area under the plasma concentration-time curve within the dosing interval (TAU = 24 h); AUC(INF), area under the plasma concentration-time from time zero to infinity; T-HALF, plasma half-life; MRT(INF), mean residence time adjusted for infusion time (paclitaxel only); CLt, total body clearance (paclitaxel only); Vss, volume of distribution at steady state (paclitaxel only); M/P, metabolite to parent ratio based on dose normalized AUC(INF) (6-OH paclitaxel only).
Figure 1.

Dose normalized mean plasma concentration-time profiles of (A) dasatinib and (B) paclitaxel. The plasma concentrations for dasatinib (dasatinib alone (solid circles)) were lower after co-administration of paclitaxel (open circles) (A). Compared to paclitaxel alone treatment (solid circles and solid triangles), paclitaxel administered with dasatinib (open circles) showed comparable exposure to paclitaxel and 6-OH paclitaxel (combination with dasatinib (open triangles)) (B).
Paclitaxel exposure was unchanged by concurrent administration of dasatinib. On Cycle 1, Day 1 and Cycle 2, Day 1, the values for Cmax were 4824 ng/mL and 3907 ng/mL, respectively, representing a 19% reduction. The geometric means for AUC(0-T), and AUC(INF) of paclitaxel were slightly reduced by 15% (15662 ng*hour/mL to 13338 ng*hour/mL), and 14% (16088 ng*hour/mL to 13761 ng*hour/mL) respectively. Mean T-HALF, MRT(INF), CLt, and Vss values were comparable between paclitaxel alone and paclitaxel in combination with dasatinib considering differences were less than 20%. Compared to treatment with paclitaxel alone, paclitaxel administered with dasatinib slightly decreased exposure to 6-OH paclitaxel after dose-normalization. Following co-administration with dasatinib, geometric means for dose-normalized Cmax, AUC(0-T), and AUC(INF) of 6-OH paclitaxel were reduced by 25% (349 ng/mL to 260 ng/mL), 23% (732 ng*hour/mL to 562 ng*hour/mL), and 20% (771 ng*hour/mL to 615 ng*hour/mL), respectively. The mean T-HALF was reduced by 25% (1.26 hour (0.75 hour) to 0.94 hour (0.47 hour).
The inter-individual variabilities (%CV) for exposure to dasatinib and 6-OH paclitaxel were high (40–90% and 40–70%, respectively). While the inter-individual variability (%CV) for exposure to paclitaxel ranged from 20% to 40%, indicating moderate inter-individual variability.
Dose Administration
There were 3–6 patients in each cohort, and 8 in the expansion cohort. The first 3 patients started at a dasatinib dose of 100 mg daily, paclitaxel 175 mg/m2, and carboplatin AUC 6. There was one DLT observed in the 100 mg dasatinib cohort (grade 3 myalgia) during the first cycle of therapy. Three additional patients were treated at this same dose and no further DLTs were observed. The next 3 patients were treated with a dasatinib dose of 120 mg daily, paclitaxel 175 mg/m2, and carboplatin AUC 6 with no DLTs. The final cohort was treated with a dasatinib dose of 150 mg daily, paclitaxel 175 mg/m2, and carboplatin AUC 6 with no DLTs during the first cycle of therapy. However, all three patients had grade 4 neutropenia at 2 weeks and due to safety concerns no further dose escalation was conducted. The RP2D was established at 150 mg daily of dasatinib in combination with paclitaxel 175 mg/m2 and carboplatin AUC 6 every 3 weeks. The dose level was confirmed with 8 additional patients treated at the RP2D.
Toxicity
The most frequent drug-related adverse events were neutropenia (95% grade 3–4), thrombocytopenia (35% grade 3–4), anemia (30% grade 3–4), and fatigue (10% grade 2–3) (Table 4). While one case of grade 3 myalgia was observed as a DLT, significant musculoskeletal toxicity was otherwise not reported. Clinically-significant pleural effusions, ascites, or cardiac issues were not observed. Dose modifications were required in 90% of patients (100%, 67%, and 91% in cohort 1, 2, and 3, respectively), of which 48% (46/95) were secondary to hematologic toxicity (Supplemental Table 1).
Table 4.
Summary of Adverse Events for All Treatment Cycles
| 100 mg qd1 N=6 |
120 mg qd N=3 |
150 mg qd2 N=11 |
||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
| ||||||||||||
| Grade | 1 | 2 | 3 | 4 | 1 | 2 | 3 | 4 | 1 | 2 | 3 | 4 |
|
| ||||||||||||
| Variable | ||||||||||||
|
| ||||||||||||
| Hematologic | ||||||||||||
|
|
||||||||||||
| Anemia | 1 (17) | 4 (67) | 1 (17) | - | - | 2 (67) | 1 (33) | - | 2 (18) | 4 (36) | 3 (27) | 1 (9) |
|
|
||||||||||||
| Neutropenia | - | - | 2 (33) | 4 (67) | - | - | 1 (33) | 2 (67) | - | - | 1 (9) | 9 (82) |
|
|
||||||||||||
| Febrile Neutropenia | - | - | - | 1 (17)3 | - | - | - | - | - | - | 1 (9) | - |
|
|
||||||||||||
| Thrombocytopenia | 2 (33) | 1 (17) | 1 (17) | 1 (17) | - | - | 1 (33) | - | 1 (9) | 4 (36) | 2 (18) | 2 (18) |
|
| ||||||||||||
| Allergy | - | - | 1 (17) | - | - | - | 1 (33) | - | 1 (9) | 1 (9) | - | - |
|
| ||||||||||||
| Fatigue | 2 (33) | 1 (17) | 2 (33) | - | 3 (100) | - | - | - | 3 (27) | 7 (64) | - | - |
|
| ||||||||||||
| Dermatogic | ||||||||||||
|
|
||||||||||||
| Flushing | 1 (17) | - | - | - | 1 (33) | - | - | - | 1 (9) | - | 1 (9) | - |
|
|
||||||||||||
| Alopecia | - | 6 (100) | - | - | 1 (33) | 2 (67) | - | - | 2 (18) | 8 (73) | - | - |
|
|
||||||||||||
| Pruritis | - | 1 (17) | - | - | - | - | - | - | 1 (9) | - | - | - |
|
|
||||||||||||
| Rash | - | - | - | - | - | - | - | - | 3 (27) | - | - | - |
|
| ||||||||||||
| Gastrointestinal4, 5 | ||||||||||||
|
|
||||||||||||
| Anorexia | 2 (33) | 1 (17) | - | - | 3 (100) | - | - | - | 5 (45) | 3 (27) | - | - |
|
|
||||||||||||
| Constipation | - | 2 (33) | - | - | 1 (33) | - | - | - | 4 (36) | 1 (9) | - | - |
|
|
||||||||||||
| Diarrhea | 4 (67) | 2 (33) | - | - | 3 (100) | - | - | - | 6 (55) | 1 (9) | - | - |
|
|
||||||||||||
| Mucositis/Stomatitis | 2 (33) | - | - | - | 1 (33) | - | - | - | - | - | - | - |
|
|
||||||||||||
| Nausea | 2 (33) | 2 (33) | - | - | 3 (100) | - | - | - | 4 (36) | 5 (45) | - | - |
|
|
||||||||||||
| Dysgeusia | 1 (17) | - | - | - | - | - | - | - | 1 (9) | - | - | - |
|
|
||||||||||||
| Vomiting | 2 (33) | 1 (17) | - | - | 2 (67) | - | - | - | 4 (36) | 3 (27) | - | - |
|
| ||||||||||||
| Metabolic6,7 | ||||||||||||
|
|
||||||||||||
| Electrolyte | 1 (17)6 | - | - | - | 2 (67)6 | - | - | - | 7 (64)6 | 5 (45)6 | 2 (18)6 | 1 (9)6 |
|
|
||||||||||||
| Hyperglycemia | - | - | - | - | - | - | - | - | 1 (9) | 2 (18) | - | - |
|
| ||||||||||||
| Neurologic8 | ||||||||||||
|
|
||||||||||||
| Anxiety | - | 1 (17) | - | - | - | - | - | - | - | 1 (9) | - | - |
|
|
||||||||||||
| Sensory neuropathy | 3 (50) | 1 (17) | - | - | 2 (67) | - | - | - | 5 (45) | 1 (9) | 1 (9) | - |
|
| ||||||||||||
| Ocular | 1 (17) | - | - | - | 1 (33) | - | - | - | - | - | - | - |
|
| ||||||||||||
| Pain9 | ||||||||||||
|
|
||||||||||||
| Head | 1 (17) | - | - | - | - | - | - | - | 3 (27) | - | - | - |
|
|
||||||||||||
| Joint | - | 2 (33) | - | - | - | 1 (33) | - | - | - | - | 1 (9) | - |
|
|
||||||||||||
| Muscle | - | 1 (17) | 1 (17)1 | - | - | - | - | - | - | - | - | - |
|
|
||||||||||||
| Other | 1 (17) | - | 1 (17) | - | - | - | - | - | 1 (9) | - | 1 (9) | - |
|
| ||||||||||||
| Pulmonary10 | ||||||||||||
|
|
||||||||||||
| Cough | 1 (17) | - | - | - | 1 (33) | - | - | - | 2 (18) | - | - | - |
|
|
||||||||||||
| Dyspnea | - | - | 1 (17) | - | 2 (67) | 1 (33) | - | - | 3 (27) | 1 (9) | 1 (9) | - |
Additional toxicities in cohort 1 included musculoskeletal toxicity characterized by grade 1 joint-function toxicity (n=1) and grade 1 muscular complaints (n=1). The grade 3 myalgia is reported under pain.
Additional toxicities in cohort 3 included the following: grade 3 hypotension (n=1), grade 1 weight loss (n=2), grade 1 epitaxis (n=1), and grade 1 facial and neck edema (n=1).
There was one report of infection associated with febrile neutropenia. Two other infections occurred including 1 urinary tract infection occurred in cohort 1.
Gastrointestinal toxicity also included the following: (1) grade 1 dehydration (n=1) in cohort 1; (2) grade 1 distension (n=1), grade 1 xerostomia (n=1), grade 1 gastritis (n=1) in cohort 2; and (3) grade 1 xerostomia (n=1) in cohort 3.
Gastrointestinal toxicity included other unspecified etiologies: (1) grade 1 (n=1) and grade 2 (n=1) in cohort 1; (2) grade 1 (n=1) in cohort 2; and (3) grade 1 (n=1) in cohort 3.
Electrolyte abnormalities were the following: (1) grade 1 hyponatremia (n=1) in cohort 1; (2) grade 1 hypomagnesemia (n=1) and hypokalemia (n=1) in cohort 2; and (3) grade 3 hypercalcemia (n=1); grade 2 hypocalcemia (n=1); hypomagnesemia (grade 1 (n=2), grade 2 (n=1)); hypophosphatemia (grade 2 (n=2), grade 3 (n=1)); hypokalemia (grade 1 (n=3), grade 4 (n=1)); and grade 1 hyponatremia (n=2) in cohort 3. More than one electrolyte abnormality may have occurred in one patient.
Metabolic toxicities also included the following: grade 1 elevated transaminases (n=1), grade 1 elevated alkaline phosphatase (n=1), and proteinuria (grade 1 (n=1), grade 2 (n=1)) in cohort 3.
Neurologic toxicity included one case of grade 1 somnolence/depressed level of consciousness in cohort 2.
Pain toxicity also included the following: (1) grade 2 neuralgia (n=1), grade 1 sinus pain (n=1), and grade 1 throat pain (n=1) in cohort 1; and (2) grade 1 back pain (n=1) and grade 1 extremity pain (n=1) in cohort 2.
Pulmonary toxicity also included the following: (1) grade 1 other unspecified etiology (n=1) in cohort 1; and (2) grade 2 hypoxia (n=1 in cohort 2.
Of the 20 patients who received treatment, 3 (15%) patients completed treatment and had CRs. Three (15%) patients, who had SD, discontinued due to subsequent cancer progression. Two patients (10%) (1 with a PR and another with SD) switched to alternative treatments prior to progression. One (5%) patient refused further treatment and 11 (55%) discontinued due to toxicity (Supplemental Table 1). There were no patient deaths during the treatment phase.
Efficacy
The RR (CR + PR) was 40% (CR, 3/20 (15%); PR, 5/20 (25%)). Fifty percent (10/20) had SD and 2 were not evaluable (Supplemental Table 2). One CR was not confirmed. The median duration of response was 3.9 months. Fifty-six percent (10/18) had stable disease. The median duration of stable disease was 5.3 months. Of the 16 patients with recurrent and evaluable disease, 12 (75%) and 4 (25%) had platinum-sensitive and –resistant disease, respectively. Three (25%), 2 (17%), and 7 (58%) of patients with platinum-sensitive disease had a CR, PR, and SD, respectively. One (25%) and 3 (75%) with platinum-resistant disease had a PR and SD, respectively (Figure 2). There was 1 (17%) PR in cohort 1, 1 (33%) CR in cohort 2, and 2 (22%) CR and 4 (44%) PR in cohort 3. The PFS6-month actuarial estimate was 86% (95% confidence interval; 69–100%). The median PFS and OS were 7.8 and 16.2 months, respectively.
Figure 2.
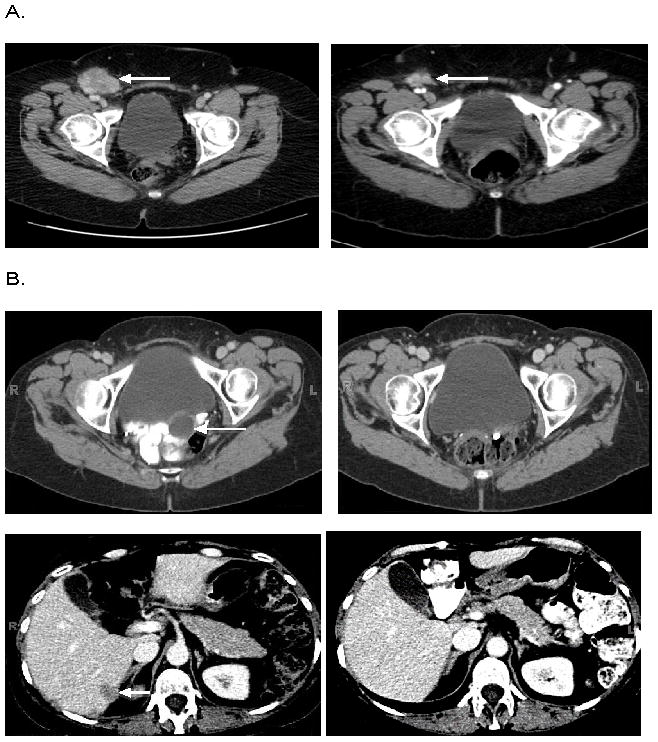
CT scan demonstrating partial response in a patient with platinum-resistant disease (A) and a complete response in a patient with platinum-sensitive disease (B).
Gene expression
Pre and post-treatment biopsies were obtained from 15 and 3 subjects, respectively. Sixty percent (9/15) of pretreatment samples had adequate quantity and quality RNA for analysis and were linked to patient response status (responder, n=5; stable disease, n=3; response data not available, n=1), survival, and PFS. The data discussed in this publication are accessible through GEO Series accession number GSE37180 (http://www.ncbi.nlm.nih.gov/geo/query/acc.cgi?acc=GSE37180).21 Gene-specific results are summarized in Supplemental Table 3 and Supplemental Figure 1. Briefly, a total of 16 genes were observed to have a p-value less than 0.001, but no genes were differentially expressed at a level to be statistically significant after correcting for multiple comparisons. This can in part be attributed to the limited power from an analysis with only 8 samples. Three gene-sets, (1) the SRC signature15, and (2) the genesets identified by Konency17 and Huang18, could not be applied directly as predictive models in this dataset because of limited sample size. However, the aggregate behavior of gene members was evaluated in heatmaps and “SAFE plots”.No distinct separation of responders from non-responders was observed in the global heatmaps and no conserved patterns observed in the “SAFE plots” (Supplemental Figure 2).
Discussion
Our phase I trial demonstrated that dasatinib could be safely administered in combination with paclitaxel and carboplatin. Concurrent administration of dasatinib with paclitaxel did not significantly alter either dasatinib or paclitaxel exposure. Dasatinib is primarily metabolized by CYP3A4 which can be induced by paclitaxel.22 Considering high variability associated with the pharmacokinetics of dasatinib, changes in Cmax and AUC following co-administration with paclitaxel were not clinically relevant, indicating dose adjustment is not necessary when dasatinib is administered with paclitaxel. Based on the consistent metabolite to parent ratio based on dose normalized AUC(INF) between paclitaxel alone and paclitaxel in combination with dasatinib, coadministration of dasatinib did not change the metabolic conversion of paclitaxel to 6-OH paclitaxel.
The combination had substantial clinical activity based on RR and disease stabilization. The toxicity profile of the combination was significant for cumulative bone marrow toxicity as manifested by a high frequency of neutropenia and thrombocytopenia. Although a dose level at which the predefined MTD (one-third of patients experienced a DLT) was not reached, the finding that all the patients who received 150mg of dasatinib once daily had significant hematologic toxicity suggested that a higher dose would probably not be tolerated. In addition, a 140 mg once daily dasatinib dose had recently been approved by the European Union for the treatment of advanced phases of chronic myelogenous leukemia (CML) and was pending FDA approval in the United States. While the optimal biologic dose for ovarian cancer remains unknown, based on the CML data, a dose of 150 mg daily was probably sufficient for target inhibition.
Hematologic toxicity was frequent in patients with leukemia and was the most common toxic effect of dasatinib in this patient population.10,23 In contrast grade 3 to 4 hematologic toxicity was rare (3–6%) in patients with solid tumors.28 Thus suggesting that dasatinib has minimal direct myelosuppressive effects on normal hemapoietic progenitor cells which are not driven by the Abl kinase. 28 Our data indicate that dasatinib in combination with cytotoxics agents with known myelosuppressive effects may increase the severity and frequency of pancytopenia.
Another common toxicity was fatigue which is similar to other studies.17,29 Ninety percent of patients in our trial reported fatigue. Fortunately most had mild or moderate fatigue, while 2 (10%) patients experienced grade 3 fatigue. We had a lower than expected incidence of pleural effusion, ascites, and edema. Severe fluid retention has been reported in 8% of patients, including pleural and pericardial effusions in 5% and 1% of patients, respectively.28 We anticipated an even higher rate in our patient population given that ovarian cancer patients often have ascites and pleural effusions secondary to their disease. Fortunately this adverse event was not a clinical problem. In contrast, Johnson and colleagues observed pleural effusions in 32% of study participants. Most of these effusions occurred in patients receiving either 90 mg twice daily or 180 mg daily doses; the incidence of effusions was only 9% in those treated with 140 mg daily.10 Thus, the decreased frequency of fluid retention seen in our trial was probably secondary to a lower dose of dasatinib.
Single agent dasatinib has been evaluated in several solid tumor types including locally-advanced and metastatic breast cancer as well as prostate cancer. The MTD has been established ranging from 70 mg twice daily to 180 mg once daily. Best clinical responses have included PRs in 1–5% and stable disease in 5–23%.23 The optimal biologic dose of dasatinib has not yet been determined in solid tumors. However, a dasatinib dose-optimization study was conducted in chronic phase CML that compared 100 mg daily, 70 mg twice daily, 140 mg daily, and 50 mg daily. The findings indicated that dasatinib 100 mg daily had the lowest rates of treatment interruption, reduction, and discontinuation and was the optimal dosing schedule.30
A trial of single-agent dasatinib (100 mg daily) in women with recurrent or persistent ovarian cancer has been performed. There were no responses with 11 (32.4%) having stable disease. Seven (20.6%) had PFS ≥ 6 months and the median PFS was 2.1 months. Grade 3 and 4 neutropenia and thrombocytopenia were not observed and there was only 1 case of grade 3 anemia (Personal communication, Dr. Russell J. Schilder). It does not appear that single-agent dasatinib has significant activity in an unselected population of women with ovarian cancer.
Dasatinib may be better used in combination with other agents given the reported in vitro synergistic and additive activity. While this trial was not designed to assess efficacy, the overall clinical benefit was highly encouraging: all evaluable patients had objective response or stable disease. The clinical benefit suggests that the combination of dasatinib with chemotherapy is worthy of further investigation. However, given the myelosuppression it may be better to combine dasatinib with one cytotoxic therapy in order to improve the tolerability. Furthermore a randomized placebo-controlled phase II clinical trial (OVERT-1) of another SRC inhibitor, saracatinib (AZD0530), in combination with paclitaxel and carboplatin in patients with platinum-sensitive ovarian cancer demonstrated no statistically significant difference in RR (53.4% vs. 51.7% in the saracatinib and placebo arms, respectively) or median PFS (8.3 vs 7.8 months, respectively).24 There are differences between saracatinib and dasatinib. Saracatinib is a dual-specific inhibitor of SRC and ABL. In contrast dasatinib inhibits SRC, BCR-ABL, c-KIT, EPHA2, PDGFβ and several other kinases. The key issue, however, is the use of a targeted agent in a unselected population. Our in vitro data indicates that SRC inhibition may be beneficial in those with tumors that exhibit a high probability of SRC deregulation or high SRC protein expression.11
Unfortunately we were unable to find a biomarker to identify women most likely to benefit from dasatinib. Despite the mandatory requirement for pre and post-treatment biopsies less than 50% of pre-treatment tissue specimens were adequate to yield sufficient RNA for analysis. Often post-treatment biopsies could not be obtained due to decreased tumor volume, clinical concerns regarding biopsy risks, or patient refusal. Although SRC expression was not correlated with response we did find several differentially regulated genes between responders and those with stable disease. Many of the genes such as cyclin D2 (CCND2)25; protein tyrosine phosphatase type IVA, member 3 (PTP4A3)26; connective tissue growth factor (CTGF)27 are involved in SRC family kinase functions and suggest that our findings are biologically plausible. Further study is certainly warranted to explore relevant biomarkers and identify a patient population most likely to benefit from the addition of dasatinib.
In conclusion, this is the first study to define the dose for combination dasatinib, paclitaxel and carboplatin that can be moved forward into future phase II or III studies. Future strategies include determining the optimal biologic dose of dasatinib. Lower doses of dasatinib may also decrease the hematologic toxicity and fatigue thus improving tolerability. Of utmost importance is the discovery of biomarkers to direct the use of targeted therapies.
Supplementary Material
Translational relevance.
Dasatinib is a multitargeted tyrosine kinase inhibitor that inhibits SRC-family kinases as well as BCR-ABL, DDR2, c-KIT, EPHA kinases, PDGFβ and others. Dasatinib has in vitro synergistic antiproliferative activity in combination with paclitaxel and carboplatin in certain ovarian cancer cell lines. We conducted a phase I trial of dasatinib in combination with paclitaxel and carboplatin in women with advanced and recurrent epithelial ovarian cancer. The triplet combination could be safely administered and demonstrated substantial clinical activity. Pharmacokinetic analysis showed that concurrent administration of dasatinib with paclitaxel did not significantly alter either dasatinib or paclitaxel. With the limited sample size, a biomarker to identify women most likely to benefit from dasatinib could not be detected. Given the observed clinical activity, further evaluation of dasatinib in combination with cytotoxic therapy is of interest, but identification of biomarkers to direct the use of dasatinib is of paramount importance.
Acknowledgments
We thank Dr. Lewis Strauss (Research & Development, Bristol-Myers Squibb) and Dr. Sun Ku Lee (Discovery Medicine and Clinical Pharmacology, Bristol-Myers Squibb) for their assistance; the research teams at Moffitt and Duke University Cancer Centers; the Phyllis Harrill Pruden family and our anonymous donors for their support; and all the women who participated on our clinical trial.
This trial was supported by 5K12-CA-100639-03 (Lyerly, Herbert PI), 07/01/05-07/31/08, NIH/NCI along with a research grant from Bristol-Myers Squibb, The Phyllis Harrill Pruden Cancer Research Fund, and an anonymous philanthropic research fund.
Footnotes
Conflict of Interest Statement: Angeles Alvarez Secord received grant funding from Bristol-Myers Squibb for this study, basic science research, and other clinical trials.
References
- 1.Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. Ca-Cancer J Clin. 2011;61:69–90. doi: 10.3322/caac.20107. [DOI] [PubMed] [Google Scholar]
- 2.Pengetnze Y, Steed M, Roby KF, Terranova PF, Taylor CC. Src tyrosine kinase promotes survival and resistance to chemotherapeutics in a mouse ovarian cancer cell line. Biochem Biophys Res Commun. 2003;309:377–83. doi: 10.1016/j.bbrc.2003.08.012. [DOI] [PubMed] [Google Scholar]
- 3.Chen T, Pengetnze Y, Taylor CC. Src inhibition enhances paclitaxel cytotoxicity in ovarian cancer cells by caspase-9-independent activation of caspase-3. Mol Cancer Ther. 2005;4:217–24. [PubMed] [Google Scholar]
- 4.Teoh D, Ayeni TA, Rubatt JM, Adams DJ, Grace L, Starr MD, et al. Dasatinib (BMS-35482) has synergistic activity with paclitaxel and carboplatin in ovarian cancer cells. Gynecol Oncol. 2011;121:187–92. doi: 10.1016/j.ygyno.2010.11.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.George JA, Chen T, Taylor CC. Src tyrosine kinase and multidrug resistance protein-1 inhibitions act independently but cooperatively to restore paclitaxel sensitivity to paclitaxel-resistant ovarian cancer cells. Cancer Res. 2005;65:10381–8. doi: 10.1158/0008-5472.CAN-05-1822. [DOI] [PubMed] [Google Scholar]
- 6.Wiener JR, Nakano K, Kruzelock RP, Bucana CD, Bast RC, Gallick GE. Decreased Src tyrosine kinase activity inhibits malignant human ovarian cancer tumor growth in a nude mouse model. Clin Cancer Research. 1999;5:2164–70. [PubMed] [Google Scholar]
- 7.Han LY, Landen CN, Trevino JG, Halder J, Lin YG, Kamat AA, et al. Antiangiogenic and antitumor effects of SRC inhibition in ovarian carcinoma. Cancer Res. 2006;66:8633–9. doi: 10.1158/0008-5472.CAN-06-1410. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Lombardo LJ, Lee FY, Chen P, Norris D, Barrish JC, Behnia K, et al. Discovery of N-(2-chloro-6-methyl- phenyl)-2-(6-(4-(2-hydroxyethyl)-piperazin-1-yl)-2-methylpyrimidin-4-ylamino)thiazole-5-carboxamide (BMS-354825), a dual Src/Abl kinase inhibitor with potent antitumor activity in preclinical assays. J Med Chem. 2004;47:6658–61. doi: 10.1021/jm049486a. [DOI] [PubMed] [Google Scholar]
- 9.Therasse P, Arbuck SG, Eisenhauer EA, Wanders J, Kaplan RS, Rubinstein L, et al. New guidelines to evaluate the response to treatment in solid tumors. J Natl Cancer Inst. 2000;92:205–16. doi: 10.1093/jnci/92.3.205. [DOI] [PubMed] [Google Scholar]
- 10.Johnson FM, Agrawal S, Burris H, Rosen L, Dhillon N, Hong D, et al. Phase 1 pharmacokinetic and drug-interaction study of dasatinib in patients with advanced solid tumors. Cancer. 2010;116:1582–91. doi: 10.1002/cncr.24927. [DOI] [PubMed] [Google Scholar]
- 11.National Cancer Institute [Internet]. U.S. National Institutes of Health: Center for Cancer Research. cited 2011 [2012 Apr 26]. Available from: http://nciarray.nci.nih.gov/reference/
- 12.Irizarry RABB, Collin F, Cope LM, Hobbs B, Speed TP. Summaries of Affymetrix GeneChip probe level data. Nucleic Acids Res. 2003;31:e15. doi: 10.1093/nar/gng015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Smyth GK. Limma: Linear Models for Microarray Data. In: Gentleman R, Carey V, Huber W, Irizarry RA, Dudoit S, editors. Bioinformatics and Computational Biology Solutions Using R and Bioconductor. New York: Springer; 2005. pp. 397–420. [Google Scholar]
- 14.Benjamini Y, Yekutieli D. False discovery rate-adjusted multiple confidence intervals for selected parameters. J Amer Statist Assoc. 2005;100:71–93. [Google Scholar]
- 15.Bild AH, Yao G, Chang JT, Wang Q, Potti A, Chasse D, et al. Oncogenic pathway signatures in human cancers as a guide to targeted therapies. Nature. 2006;439:353–7. doi: 10.1038/nature04296. [DOI] [PubMed] [Google Scholar]
- 16.Gatza ML, Lucas JE, Barry WT, Kim JW, Wang Q, Crawford MD, et al. A pathway-based classification of human breast cancer. Proc Natl Acad Sci U S A. 2010;107:6994–9. doi: 10.1073/pnas.0912708107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Konecny GE, Glas R, Dering J, Manivong K, Qi J, Finn RS, et al. Activity of the multikinase inhibitor dasatinib against ovarian cancer cells. Br J Cancer. 2009;101:1699–1708. doi: 10.1038/sj.bjc.6605381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Huang F, Reeves K, Han X, Fairchild C, Platero S, Wong TW, et al. Identification of candidate molecular markers predicting sensitivity in solid tumors to dasatinib: rationale for patient selection. Cancer Res. 2007;67:2226–38. doi: 10.1158/0008-5472.CAN-06-3633. [DOI] [PubMed] [Google Scholar]
- 19.Barry WT, Nobel AB, Wright FA. Significance analysis of functional categories in gene expression studies: a structured permutation approach. Bioinformatics. 2005;21:1943–9. doi: 10.1093/bioinformatics/bti260. [DOI] [PubMed] [Google Scholar]
- 20.Reich M, Liefeld T, Gould J, Lerner J, Tamayo P, Mesirov JP. GenePattern 2.0. Nat Genet. 2006;38:500–1. doi: 10.1038/ng0506-500. [DOI] [PubMed] [Google Scholar]
- 21.National Center for Biotechnology Information [Internet]. Bethesda (MD): Gene Expression Omnibus; 2012. [cited 2012 Apr 12]. Available from: http://www.ncbi.nlm.nih.gov/geo/query/acc.cgi?acc=GSE37180. [Google Scholar]
- 22.Rahman A, Korzekwa KR, Grogan J, Gonzalez FJ, Harris JW. Selective biotransformation of taxol to 6 alpha-hydroxytaxol by human cytochrome P450 2C8. Cancer Res. 1994;54:5543–6. [PubMed] [Google Scholar]
- 23.Development B-MSRa. Investigator Brochure Dasatinib BMS-354825, Version 102010.
- 24.Poole C, Lisyanskaya A, Rodenhuis S, Kristensen G, Pujade-Lauraine E, Cantarini M, et al. A randomized phase II clinical trial of the SRC inhibitor saracatinib (AZD0530) and carboplatin 1 paclitaxel (C1P) versus C1P in patients with advanced platinum-sensitive epithelial ovarian cancer. Ann Oncol. 2010;21 (Suppl 8):S313. [Google Scholar]
- 25.Dey A, She H, Kim L, Boruch A, Guris DL, Carlberg K, et al. Colony-stimulating factor-1 receptor utilizes multiple signaling pathways to induce cyclin D2 expression. Mol Biol Cell. 2000;11:3835–48. doi: 10.1091/mbc.11.11.3835. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Liang F, Liang J, Wang WQ, Sun JP, Udho E, Zhang ZY. PRL3 promotes cell invasion and proliferation by down-regulation of Csk leading to Src activation. J Biol Chem. 2007;282:5413–9. doi: 10.1074/jbc.M608940200. [DOI] [PubMed] [Google Scholar]
- 27.Zhang X, Arnott JA, Rehman S, Delong WG, Jr, Sanjay A, Safadi FF, et al. Src is a major signaling component for CTGF induction by TGF-beta1 in osteoblasts. J Cell Physiol. 2010;224:691–701. doi: 10.1002/jcp.22173. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.