

Abstract
Background:
Tramadol hydrochloride (HCl) and ketorolac tromethamine are analgesic drugs, which are commonly used in combination in postoperative pain management. According to some studies, metoclopramide and magnesium sulfate (MgSO4) as adjuvant agents can improve analgesia and decrease the need for other pain drugs.
Materials and Methods:
The chemical stability of tramadol HCl combined with ketorolac tromethamine and metoclopramide HCl has been studied using a stability-indicating high-performance liquid chromatographic assay method. Calibration curves were produced using linear regression of the peak area against concentration of each drug, with an r2 value ≥ 0.96. Our aim was to investigate the stability of admixture solution of tramadol HCl combined with ketorolac tromethamine and metoclopramide HCl for 48 h (25°C) and 5 days (5°C), with MgSO4, which has never been assessed.
Results:
Data obtained for admixtures prepared and stored at temperatures of 25°C and 5°C, show that all drugs have reached at least 98% of the initial concentration.
Conclusions:
For the purpose of pre-preparing drug admixtures to use with confidence, tramadol HCl infusions may be prepared in advance and then thawed before use in clinical units. On the basis of our results, the intravenous mixture of tramadol (7.69 mg/mL), metoclopramide (0.19 mg/mL), ketorolac (1.15 mg/mL), and magnesium sulfate (77 mg/mL) may be considered for a possible commercial formulation.
Keywords: Admixture, analgesia, ketorolac tromethamine, magnesium sulfate, metoclopramide hydrochloride, stability
INTRODUCTION
Appropriate management of moderate postoperative pain is well achieved associating several analgesic drugs with adjuvant agents through synergistic interaction. The potential advantage of this combined therapy is related to the minimization of the incidences of adverse effects of each drug and to the improvement of the outcome. Postoperative clinical situations, such as difficult patient extubation, respiratory depression due to opioids, and cardiovascular side effects, require a combined therapy to improve analgesia quality and decrease adverse effects of each drug when used alone.[1] This has led to administering pain drugs in continuous intravenous (IV) infusion with different mechanisms and sites of action, together with adjuvant agents.
Tramadol hydrochloride (HCl) and ketorolac tromethamine are analgesic drugs commonly used in combination in postoperative pain management.[2] Tramadol HCl is a synthetic, centrally acting analgesic with no anti-inflammatory activity and one of the most interesting and useful weak opioids for treatment of moderate to moderately severe pain with weak μ-receptor agonist properties and noradrenergic and serotonergic neurotransmission effects.[3–9]
Ketorolac tromethamine is a potent nonsteroidal anti-inflammatory drug (NSAID) with analgesic efficacy similar to opioids.[2,8–9] This drug is administered to treat moderate pain or, combined with reduced opioid doses, for severe pain.[10] According to some studies, metoclopramide HCl as an adjuvant agent can improve analgesia and decrease the need for other pain drugs; it is a dopamine and 5-HT receptor antagonist, commonly used as a prokinetic and antiemetic. Also, this has been recently investigated as an agent that can enhance the efficacy of analgesic drugs.[9,11–13] Some studies have also suggested a role of magnesium sulfate (MgSO4) as an adjuvant agent, an N-methyl-D-aspartate receptor antagonist, in the management of postoperative pain. The perioperative administration of IV MgSO 4 is associated with smaller analgesic requirements, and magnesium sulfate could be of interest as an adjuvant to postoperative analgesia.[14–16]
The aim of this study was to investigate the chemical stability of tramadol HCl combined with ketorolac tromethamine and metoclopramide HCl in solution for 48 h (25°C) and 5 days (5°C), with the presence of MgSO4.
MATERIALS AND METHODS
Preparation of stock solutions
Metoclopramide HCl (Metoclopramide Cloridrato Mayne Pharma, Biologici Italia Laboratories S.r.l., Milan, Italy) 2 mg/mL, tramadol HCl (Contramal; Grünenthal, GmbH, Stolberg, Germany) 20 mg/mL, and ketorolac tromethamine (Lixidol; Roche S.p.A., Milan, Italy) 6 mg/mL stock solutions were prepared in high-performance liquid chromatographic (HPLC)-grade deionized water and stored at 4°C during experimental assay. Well-defined volume samples were drawn from each stock solution, joined, and diluted in deionized water to produce 5 working standard solutions, with concentrations in the range of 0.5–1.5 μg/mL for metoclopramide HCl, 20–60 μg/mL for tramadol HCl, and 3–9 μg/mL for ketorolac tromethamine.
Every 48 h the working standard solutions were prepared from stock solutions and stored at 4°C. Limit of Quantitation (LOQ) values were found to be 1, 0.5, and 0.1 μg/mL for tramadol, ketorolac, and metoclopramide, respectively. Limit of Detection (LOD) values were 0.05, 0.2, and 0.1 μg/mL for tramadol, ketorolac, and metoclopramide. Precision and accuracy were determined on spiked samples at 4 concentrations with respect to a calibration graph prepared every day (n = 3). The precision of the method was evaluated as the intra- and interday Relative Standard Deviation (RSD) of the measured peak areas by assaying spiked samples at 4 different concentrations. All samples for these purposes were freshly prepared, including preparing the standard solution from the same stock solution.
Admixture preparation and analysis
Six drug admixtures were prepared by transferring the contents of one ampule of metoclopramide HCl, 4 ampules of tramadol HCl, 2 ampules of ketorolac tromethamine, and 4 ampules of MgSO4 (1 g/10 mL ampule, Magnesio Solfato Monico; Monico S.p.A., Venezia Mestre, Italy) to give each a final volume of 52 mL. All the solutions were prepared on different days, stored at 25°C and assessed over a period of 48 h. Solutions were stored in amber colored glass bottles with air-tight caps to protect them from direct light exposure. The nominal concentration of each drug in all prepared solutions was 0.19 mg/mL for metoclopramide HCl, 7.69 mg/mL for tramadol HCl, and 1.15 mg/mL for ketorolac tromethamine. All the drug admixtures were visually inspected immediately after preparation (0 h) and at 24 and 48 h against a black and white background to ensure any physical changes (eg, color, phase separation, precipitation).
A 100 μL sample was drawn from each solution at intervals of 0 (initial), 24, and 48 h and diluted to 20 mL with deionized water; we prepared solutions in triplicate at each time interval to have 54 samples. Twenty microliters of each sample was injected into the HPLC system to determine concentration of each drug.
As previously described, 6 drug admixtures were prepared on different days, stored at 5°C (refrigerated), assessed, and visually inspected at intervals of 0 (initial), 1, 3, and 5 days. A 100 μL of sample was drawn from each solution and diluted to 20 mL with deionized water; we prepared solutions in triplicate at each time interval to have 72 samples. Twenty microliters of each sample was injected into the HPLC system to determine concentration of each drug.
High-performance liquid chromatography
The HPLC method developed by Küçük et al was modified for use in this study.[17–18] The instrumentation included a binary pump (Model G1312A; Agilent Technologies; Hewlett-Packard, Waldbronn, Germany) and an ultraviolet (UV)–variable wavelength detector (Model G1314A; Agilent). At the beginning of our study, we looked for the maximum UV absorption wavelength for each drug solution on the basis of UV spectra for each solution. As we used UV–variable wavelength detector, and metoclopramide and tramadol retention times were very close reciprocally, we found that 271 nm was the best wavelength for both drugs to have good sensitivity and maximum signal/noise ratio. For ketorolac drug solutions, we found that 323 nm was the best absorption wavelength. Separation was achieved using a reversed-phase C18 5 μm particle size column (Luna C18 (2) 100A, 150 × 4.6 mm; Chemtek Analytica Srl, Anzola Emilia (BO), Italy), equipped with a 2-cm precolumn, which was maintained at 25°C with a column temperature controller (Thermosphere TS-130; Phenomenex, Torrance, California). HPLC-gradient analysis were performed using the following mobile phase: 0.01 M phosphate buffer, potassium dihydrogen phosphate [KH2PO4] ultra for molecular biology (Fluka and Riedel-de Haën, Buchs SG, Switzerland) and acetonitrile (Sigma-Aldrich Supelco, Bellefonte, Pennsylvania) (75:25, v/v) with the addition of 0.1% triethylamine, adjusted to pH 3 with phosphoric acid (solvent A) and H2O–acetonitrile (50:50, v/v, solvent B). The elution-gradient program was 0–6 min 0% B, 6–10 min 80% B, 10–15 min 0% B [Table 1].
Table 1.
The elution-gradient program
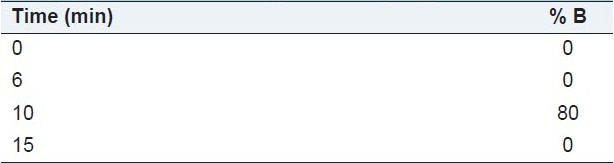
Each mobile phase was prepared fresh daily, filtered through a 0.45 μm × 47 mm nylon membrane filter (Supelco, Bellefonte, Pennsylvania Nylon 66 Filter Membranes pore size 0.20 μm, diameter 47 mm), and degassed ultrasonically for 20 min before use. The flow rate was 1 mL/min, and the injected volume was 20 μL. The run time was 15 min and the approximate retention times for metoclopramide, tramadol, and ketorolac were 2.8, 3.4, and 13.4 min, respectively [Figure 1].
Figure 1.
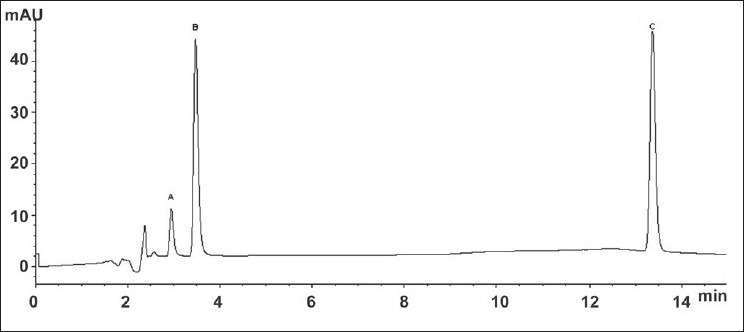
A typical HPLC–UV chromatogram of metoclopramide hydrochloride (a), tramadol hydrochloride (b), and ketorolac tromethamine (c), eluted at 2.8, 3.4, and 13.4 min, respectively.
Data analysis
Calibration curves were produced using linear regression of the peak area against concentration of each drug [Table 2]. We obtained 5 calibration curves for each drug and all the curves were linear over the concentration ranges considered for each drug: metoclopramide HCl r2 = 0.991; tramadol HCl r2 = 0.995; ketorolac tromethamine r2 = 0.961. The results were averaged and analyzed by linear simple regression model of y = mx + q by the least-squares method. The t test was used to examine the concentration difference at each time, and the significance level of α error was less than 0.001.
Table 2.
Linear simple regression model (y = mx + q) by the least-squares method

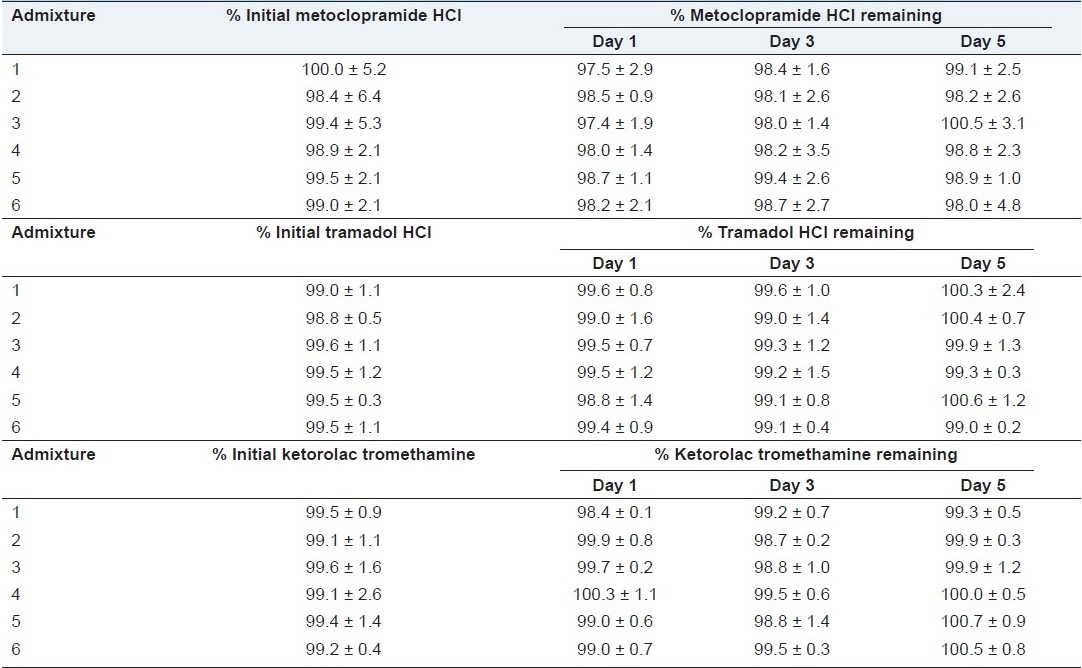
All the data reported in Tables 3 and 4 were submitted to ANOVA and differences analyzed by Tukey's honestly significant differences test. No significant admixture and time-dependent effect interactions were observed (P ≥ 0.05).
Table 3.
Percentage ± %SD of metoclopramide hydrochloride, tramadol hydrochloride, and ketorolac tromethamine remaining in the admixtures with magnesium sulfate after storage at 25ŶC for 48 h
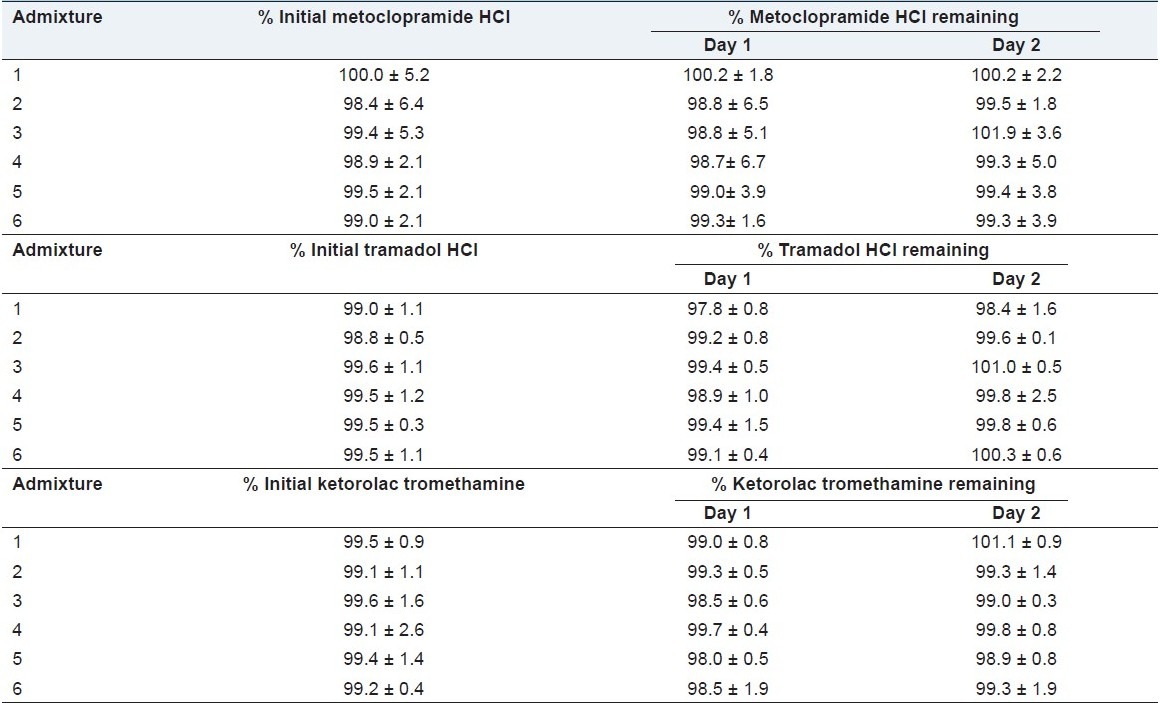
Table 4.
Percentage ± %SD of metoclopramide hydrochloride, tramadol hydrochloride, and ketorolac tromethamine remaining in the admixtures with magnesium sulfate stored at 5°C for 5 days
RESULTS AND DISCUSSION
At the Mediterranean Institute for Transplantation and Highly Specialized Therapies (ISMETT, Palermo, Italy) is already using an experimental protocol for the treatment of moderate to severe pain, which involves the administration of intravenous mixture of tramadol (7.69 mg/mL), metoclopramide (0.19 mg/mL), ketorolac (1.15 mg/mL), and magnesium sulfate (77 mg/mL). To use this drug combination is necessary that the drugs are compatible with each other and the mixture is stable over time.
Drugs stability was detected for solutions stored at 25°C and 5°C. Table 3 shows drugs solution concentration after storage period up to 48 h. The data obtained are in agreement with data reported in the literature regarding a mixture of tramadol, ketorolac, metoclopramide, and ranitidine in a solution for intravenous perfusion.[9]
Data reported in Table 4 show the remaining percentage of drug concentrations in all admixtures prepared and assessed over a period of 5 days. It is possible to observe constant percentage concentrations remaining for all the 3 drugs at 1, 3, and 5 days when stored at 5°C. We believe that the information has clinical utility in facilitating the preparation and dispensing of the tramadol, metoclopramide, ketorolac, and magnesium sulfate mixture in postoperative pain management. On the basis of our results, the mixture may be considered for a possible commercial formulation, at the concentrations listed.
CONCLUSIONS
In this study, precise and accurate HPLC method suitable for stability evaluation of tramadol HCl combined with ketorolac tromethamine and metoclopramide HCl is described. The physical appearance of the solutions remained constant during the study period, without the formation of any visible discoloration, cloudiness, or precipitation. In admixtures containing MgSO4 and stored at 25°C, each drug, at the same time, reached at least 98% of the initial concentration during 48 h. Solutions prepared adding MgSO4 assessed over a period of 5 days at 5°C show the lower confidence limit of the estimated regression line of the concentration at 98% of the initial concentration. Within these limits, for the purpose of pre-preparing drug admixtures to use with confidence, tramadol HCl infusions may be prepared in advance and then thawed before use in clinical units. Moreover, information about the chemical stability of the drugs could be utilized in further investigations focused on IV infusion solutions.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Joris J, Kaba A, Lamy M. Transition between anesthesia and post-operative analgesia: Relevance of intra-operative administration of analgesics. Acta Anaesthesiol Belg. 2001;52:271–9. [PubMed] [Google Scholar]
- 2.López-Muñoz FJ, Díaz-Reval MI, Terrón JA, Déciga-Campos M. Analysis of the analgesic interactions between ketorolac and tramadol during arthritic nociception in rat. Eur J Pharmacol. 2004;484:157–65. doi: 10.1016/j.ejphar.2003.11.005. [DOI] [PubMed] [Google Scholar]
- 3.Lehmann KA. Tramadol in acute pain. Drugs. 1997;53:25–33. doi: 10.2165/00003495-199700532-00007. [DOI] [PubMed] [Google Scholar]
- 4.Klotz U. Tramadol-the impact of its pharmacokinetic and pharmacodynamic properties on the clinical management of pain. Arzneimittelforschung. 2003;53:681–7. doi: 10.1055/s-0031-1299812. [DOI] [PubMed] [Google Scholar]
- 5.Abanmy NO, Zaghloul IY, Radwan MA. Compatibility of tramadol hydrochloride injection with selected drugs and solutions. Am J Health Syst Pharm. 2005;62:1299–302. doi: 10.1093/ajhp/62.12.1299. [DOI] [PubMed] [Google Scholar]
- 6.Barcia E, Martín A, Azuara ML, Sánchez Negro S. Tramadol and Hyoscine N-bromide combined in infusion solutions: Compatibility and stability. Support Care Cancer. 2007;15:57–62. doi: 10.1007/s00520-006-0101-2. [DOI] [PubMed] [Google Scholar]
- 7.Scott LJ, Perry CM. Tramadol: A review of its use in perioperative pain. Drugs. 2000;60(1):39–45. doi: 10.2165/00003495-200060010-00008. [DOI] [PubMed] [Google Scholar]
- 8.Tzu FL, Feng-Sheng L, Wei-Han C, Yu-Chang Y, Chih-Peng L, Shou-Zen F, et al. Compatibility and stability of binary mixtures of ketorolac tromethamine and tramadol hydrochloride injection concentrate and diluted infusion solution. Acta Anaesthesiol Taiwan. 2010;48:117–21. doi: 10.1016/S1875-4597(10)60042-2. [DOI] [PubMed] [Google Scholar]
- 9.Cabrera J, Mancuso M, Cabrera-Fránquiz F, Limiñana J, Díez A. Stability and compatibility of the mixture of tramadol, ketorolac, metoclopramide and ranitidine in a solution for intravenous perfusion. Farm Hosp. 2010 doi: 10.1016/j.farma.2010.01.007. [DOI] [PubMed] [Google Scholar]
- 10.World Health Organization. Care pain relief and palliative care. Technical report series no 804. 1990. [accessed on 2009 Oct 1]. Available from: http://www.who.int/cancer/palliative . [PubMed]
- 11.Ceyhan A, Ustun H, Altunatmaz K, Ide T, Unal N. Is metoclopramide an alternative to tramadol in management of post-operative pain? An experimental study. J Vet Med A Physiol Pathol Clin Med. 2005;52:249–53. doi: 10.1111/j.1439-0442.2005.00719.x. [DOI] [PubMed] [Google Scholar]
- 12.Gibbs RD, Movinsky BA, Pellegrini J, Vacchiano CA. The morphine-sparing effect of metoclopramide on postoperative laparoscopic tubal ligation patients. AANA J. 2002;70:27–32. [PubMed] [Google Scholar]
- 13.Majedi H, Rabiee M, Khan ZH, Hassannasab B. A comparison of metoclopramide and lidocaine for preventing pain on injection of diazepam. Anaesth Analg. 2002;95:1297–9. doi: 10.1097/00000539-200211000-00036. [DOI] [PubMed] [Google Scholar]
- 14.Unlügenç H, Gündüz M, Ozalevli M, Akman H. A comparative study on the analgesic effect of tramadol, tramadol plus magnesium, and tramadol plus ketamine for postoperative pain management alter major abdominal surgery. Acta Anaesthesiol Scand. 2002;46:1025–30. doi: 10.1034/j.1399-6576.2002.460817.x. [DOI] [PubMed] [Google Scholar]
- 15.Tramer MR, Schneider J, Marti RA, Rifat K. Role of magnesium sulfate in postoperative analgesia. Anesthesiology. 1996;84:340–7. doi: 10.1097/00000542-199602000-00011. [DOI] [PubMed] [Google Scholar]
- 16.Koinig H, Wallner T, Marhofer P, Andel H, Hörauf K, Mayer N. Magnesium sulfate reduces intra- and postoperative analgesic requirements. Anesth Analg. 1998;87:206–10. doi: 10.1097/00000539-199807000-00042. [DOI] [PubMed] [Google Scholar]
- 17.Küçük A, Kadioðlu Y. Determination of tramadol hydrochloride in ampoule dosage forms by using UV spectrophotometric and HPLC-DAD methods in methanol and water media. IL Farmaco. 2005;60:163–9. doi: 10.1016/j.farmac.2004.12.002. [DOI] [PubMed] [Google Scholar]
- 18.Küçük A, Kadioğlu Y, Çelebi F. Investigation of the pharmacokinetics and determination of tramadol in Rabbit plasma by a high-performance liquid chromatography-diode array detector method using liquid-liquid extraction. J Chromatogr B Analyt Technol Biomed Life Sci. 2005;816:203–8. doi: 10.1016/j.jchromb.2004.11.031. [DOI] [PubMed] [Google Scholar]