

Abstract
Purpose
The current study was conducted to ascertain whether the effects of nativity (i.e., U.S. born vs. immigrant) on Hispanic adolescent substance use is mediated by ecological processes such as family functioning, school connectedness, and perceived peer substance use.
Methods
The effects of family, peer, and school processes on adolescent substance use were examined in a nationally representative sample of 742 (358 male, 384 female) Hispanic youth (mean age = 15.9; SD = 1.8).
Results
Results from a structural equation model indicated that the higher rates of substance use among U.S.-born Hispanics (compared with foreign-born Hispanics) are partially mediated by perceived peer substance use (as measured by the adolescent). The results also showed that perceived peer substance use and school connectedness mediate the relationship between family processes and substance use, suggesting that family processes may offset some of the deleterious effects of negative peer selection on adolescent substance use.
Conclusion
These findings imply that public health behavioral interventions to prevent substance use among both U.S.-born and foreign-born Hispanics may need to attend to multiple ecological processes, including family, school, and peers.
Keywords: Substance use, Hispanic, Adolescents, Nativity, Immigrant
Cigarette smoking, alcohol, and illicit drug use represent important public health problems facing American youth [1]. However, these problems are not evenly distributed across ethnic groups. According to national population-based studies, Hispanic adolescents report higher rates of cigarette use, alcohol use, and use of most categories of illicit drug use than non-Hispanic white and African American adolescents [1]. This health disparity is especially alarming given that Hispanics represent the largest and fastest growing minority population in the United States [2]. It is expected that by 2050, Hispanics will comprise 24% of all the U.S. population [3]. Furthermore, Hispanics are a young population, with nearly 40% under age 20 [4]. Because of the large and growing population of Hispanic youth, decreasing behavioral health risks such as cigarette, alcohol, and drug use in this population is of considerable public health importance. Efforts to understand the prevalence and etiology of cigarette, alcohol, and drug use, among Hispanic adolescents are challenged by the heterogeneity within the Hispanic population. Studies attempting to identify risk and protective processes for substance use in Hispanics need to consider the heterogeneity of this population [5,6].
Nativity status (U.S. born vs. immigrant) [7] is a primary demographic source of variation in the Hispanic population. Previous studies have shown that U.S.-born Hispanics report higher rates of cigarette, alcohol, and drug use than their immigrant counterparts [8-11]. Some studies have examined reasons explaining why U.S.-born Hispanics are more likely to report substance use than their foreign-born counterparts. For example, there is a growing body of literature describing the Immigrant Paradox [11]: the tendency for foreign-born Hispanics, who would be expected to show poorer signs of health because of immigration and life disruptions, to report more favorable health indicators than U.S.-born Hispanics. Potential explanations for the Immigrant Paradox include the deterioration of cultural and Hispanic family values, attitudes, and behaviors [6], and the increased exposure to substances in the United States than in the immigrant host country [12]. Social–ecological processes such as school, peer, and family processes may also explain, at least in part, the Immigrant Paradox [5,7,13].
It should be noted, however, that these studies conducted to examine the Immigrant Paradox have been sampled only from specific areas of the United States. Because different segments of the Hispanic population have settled in different parts of the country [14], a nationally representative sample would be most likely to provide authoritative evidence related to the Hispanic Immigrant Paradox. To our knowledge, however, no studies have used nationally representative samples to examine whether ecological processes such as family functioning, school connectedness, and peers partially explain the Immigrant Paradox in a prospective cohort design. A number of studies, however, have documented the direct relationships of family functioning, school connectedness, and peer drug use to substance use in adolescents in general, and in Hispanic adolescents in particular (see [5] for a review). Positive family functioning, bonding to and success in school, and avoidance of substance using peers have been identified as protective against substance use in both general population and Hispanic adolescents [5,15-17]. Furthermore, a recent study by Galaif and colleagues [18] found that U.S.-born Hispanics had more deviant peers, poorer family functioning, and less school connectedness than immigrant Hispanics. Thus, these processes might help explain why U.S.-born Hispanics report higher rates of substance use than their immigrant counterparts. Therefore, the purpose of the present study was to determine whether, and to what extent, family functioning (defined as parental involvement and family connectedness), school connectedness, and peer substance may partially mediate the effects of nativity and Hispanic adolescent substance use (see Figure 1).
Figure 1.
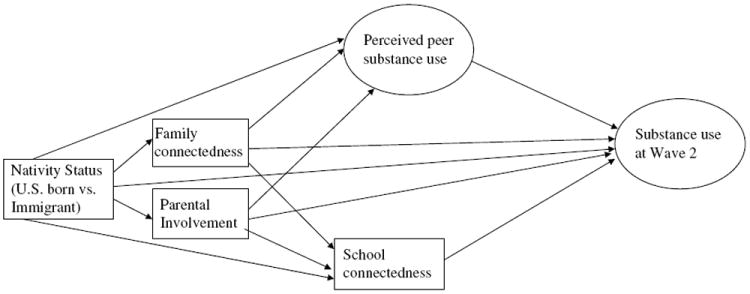
Hypothesized ecological predictors of hispanic adolescent substance use.
These ecological processes (i.e., family functioning, school connectedness, and peer substance use) were chosen as potential mediators for the association between nativity status and adolescent substance use, because they are central to ecodevelopmental theory [13,19]. Ecodevelopmental theory is a conceptual model that describes the interconnections among various sources of risk and protection in adolescents’ lives. Microsystems, which represent contexts in which the adolescent participates directly, such as the family, school, and peers, have by far the strongest effects on adolescent development (e.g., [20]), and hence, are the focus of the present study. Ecodevelopmental processes such as parental involvement, family connectedness, peer substance use, and school connectedness have been found to be related to adolescent substance use [13,17].
Method
Study design
The present study analyzed data from the National Longitudinal Study of Adolescent Health, commonly referred to as Add Health. Add Health is a school-based, prospective, nationally representative cohort study of adolescents in grades 7 through 12. It was designed to examine the effects of social influences on health-related behaviors such as alcohol, cigarette, and drug use. The Add Health dataset consists of three waves. Wave 1 data collection occurred in 1994 and 1995 and included in-school interviews of 90,118 adolescents in grades 7 through 12. Of those adolescents, 13,143 completed home-based interviews. Substance use data were collected during these in-home interviews. Wave 2 consisted of follow up in-home interviews 1 year later. Wave 3, conducted in 2001 and 2002 (i.e., 5 to 6 years after the Wave 2 data), followed the adolescent participants into emerging adulthood. Because the focus of the present study is on adolescents (and not on emerging adulthood), the Wave 3 data were not used in the present study. With regard to the sampling frame, all high schools in the U.S. that had an 11th grade and a minimum enrollment of 30 students were eligible for participation. Of the 26,666 eligible schools, 132 were randomly selected with unequal probability. Implicit stratification and systematic sampling methods ensured that the schools selected were representative of all U.S. high schools with respect to school size, school type, U.S. region, location, and percentage of white students. The response rates for the Wave 1 and Wave 2 surveys were 78.9% and 88.2%, respectively. Additional details regarding the study design, including sampling frame, for the Add Health study can be found at http://www.cpc.unc.edu/projects/addhealth/design.
Participants
The present study used the Wave 1 and Wave 2 Add Health public use data set, distributed by Sociometrics Corporation (http://www.socio.com). A total of 742 participants (358 boys, 384 girls) who identified themselves as Hispanic or Latino during the Wave 1 survey and completed the nativity status (i.e., U.S. born vs. foreign born) item were included in the analyses. At Wave 1, the majority of the participants solely self-identified as Mexican (55.6%), Puerto Rican (13.0%), or Central/South American (12.0%). Of the 742 participants, 73.7% were U.S. born, whereas 26.3% were foreign born. Participants’ average age was 15.9 years (SD = 1.8 years). A total of 17.9% of adolescents’ families were on some sort of public assistance.
Measures
Family functioning at Wave 1 was assessed using two indicators: family connectedness and parental involvement. The 11-item family connectedness subscale (Cronbach’s α = .88) assesses the extent to which adolescents perceive their mother and father as warm, loving, and caring, as well as adolescents’ overall satisfaction with their relationships with their mother, father, and other family members. Each item is rated on a five-point Likert scale ranging from “strongly agree” to “strongly disagree” or from “not at all” to “very much” (the labels for the endpoints vary as a function of item content). Consistent with prior research [21,22], the sum of the 11 items is used as a single subscale in the analyses. The 20-item parent–adolescent activities subscale assesses the extent of parental involvement in various activities with the adolescent during the 4 weeks prior to assessment. The activities listed include going shopping, playing a sport, and attending a religious service or churchrelated event. Each item is binary, where 0 indicates that the parent did not participate in the indicated activity with their adolescent and 1 indicates that the parent did participate in the activity with their adolescent. A single scale consisting of the sum of the counts was used in the analyses.
School connectedness at Wave 1 was assessed using six items. These items asses whether adolescents feel they are connected/bonded to their school and to their teachers, whether adolescents feel safe at school, and whether adolescents feel their teachers are treating them fairly. Adolescents responded on a five-point Likert scale ranging from “strongly disagree” to “strongly agree” or “not at all” to “very much.” Cronbach’s α in the present sample is .77.
Adolescent’s report of their peers’ substance use at Wave 1 was assessed using three items. Adolescents were asked whether any of their three best friends (a) smoked at least 1 cigarette a day (perceived peer cigarette use), (b) drank alcohol at least once a month (perceived peer alcohol use), and (c) used marijuana at least once a month (perceived peer drug use). Details on how these items were used in the analyses can be found in the “Adolescent Substance Use and Perceived Peer Substance Use Measurement Models” section below.
Adolescent’s own substance use at Wave 1 was measured using three items: (a) ever tried a cigarette; (b) ever drank beer, wine, or liquor (not just a sip or a taste of someone else’s drink) more than two or three times; and (c) ever used marijuana. During their Wave 2 interview (i.e., 1 year after the Wave 1 interview), adolescents responded whether they had (a) tried a cigarette since their Wave 1 interview; (b) drank beer, wine, or liquor (not just a sip or a taste of someone else’s drink) more than two or three times since their Wave 1 interview; or (c) used marijuana since their Wave 1 interview. Because data on illicit drugs (other than marijuana use) were not collected for perceived peer substance use and to have parallel measures for perceived peer substance use and adolescent substance use, we only included marijuana use (in addition to alcohol and cigarette use) for the adolescent substance use measure. Details on how these items were used in the analyses can be found in the “Adolescent Substance Use and Perceived Peer Substance Use Measurement Models” section below.
Results
Descriptive statistics and bivariate correlations
Descriptive statistics and bivariate correlations for the ecological processes and substance use variables can be found in Table 1 and Table 2, respectively.
Table 1.
Comparisons of demographic characteristics and ecological predictors by nativity status
| U.S. born (n = 546) | Immigrant (n = 196) | Total | |||
|---|---|---|---|---|---|
|
| |||||
| Percent* | χ2(1) | p | |||
| Gender | 6.04 | .50 | |||
| Male | 50.9% | 47.4% | 50.0% | ||
| Female | 49.1% | 52.6% | 50.0% | ||
| Public assistance | 18.7% | 15.8% | 6.84 | .37 | 17.9% |
| Perceived peer substance use | 72.1% | 49.9% | 268.3 | <.001 | 66.3% |
| Mean (SD)* | F (1, 131) | p | |||
| Age | 15.7 (1.8) | 16.4 (1.7) | 16.6 | .0001 | 15.9 (1.8) |
| Family connectedness | 46.8 (6.6) | 46.1 (6.9) | 1.8 | .18 | 46.6 (6.6) |
| Parental involvement | 5.4 (3.4) | 5.2 (3.2) | 0.5 | .48 | 5.3 (3.3) |
| School connectedness | 21.8 (4.4) | 22.8 (4.0) | 7.2 | .0081 | 22.1 (4.3) |
Analyses used weighted data to take account for the clustered sampling design.
Table 2.
Means (or percentages), standard deviations, and correlations for the ecological processes and substance use variables
| Variable | Mean or percentage | SDa | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Family connectedness | 46.6 | 6.6 | 1.00 | ||||||||
| 2. Parental involvement | 5.3 | 3.3 | 0.29* | 1.00 | |||||||
| 3. School connectedness | 22.1 | 4.3 | 0.42* | 0.18* | 1.00 | ||||||
| 4. Peer marijuana use | 36.0% | −0.19* | −0.09* | −0.29* | 1.00 | ||||||
| 5. Peer alcohol use | 52.8% | −0.23* | −0.07* | −0.24* | 0.67* | 1.00 | |||||
| 6. Peer cigarette use | 39.7% | −0.14* | −0.15* | −0.34* | 0.57* | 0.61* | 1.00 | ||||
| 7. Adolescent marijuana use at Wave 2 | 28.2% | −0.13* | −0.06* | −0.23* | 0.61* | 0.40* | 0.38* | 1.00 | |||
| 8. Adolescent cigarette use at Wave 2 | 39.2% | −0.14* | −0.06* | −0.18* | 0.48* | 0.35* | 0.38* | 0.74* | 1.00 | ||
| 9. Adolescent alcohol use at Wave 2 | 49.9% | −0.04* | −0.001 | −0.13* | 0.40* | 0.43* | 0.27* | 0.58* | 0.49* | 1.00 |
We do not report SD for percentages.
p < .001.
Differences between U.S.-born and foreign-born adolescents
Substance use
STATA version 9.0 was first used to calculate the weighted cigarette, alcohol, and marijuana use prevalence rates for both the U.S.- and foreign-born Hispanics at Wave 1 and Wave 2. Rao-Scott chi-square tests were then used to compare whether rates of lifetime (measured during Wave 1) and past year (measured during Wave 2) cigarette, alcohol, marijuana, and substance use differed between immigrant and U.S.-born Hispanic youth.
Results indicated that both lifetime, Wave 1: χ2(1) = 319.4, p < .001, and past year, Wave 2: χ2(1) = 142.7, p < .01, overall substance use rates (i.e., alcohol, cigarette, or marijuana use) were significantly higher among U.S.-born than immigrant Hispanic youth (Figure 2). For example, at the time of the Wave 1 assessment, 75.7% of U.S.-born youth reported having ever used cigarettes, alcohol, or marijuana, compared to 52.4% of immigrant youth. Furthermore, compared to foreign born youth, U.S.-born youth reported higher rates of lifetime cigarette use, χ2(1) = 228.1, p < .001, lifetime alcohol use, χ2(1) = 340.4, p < .001, and lifetime marijuana use, χ2(1) = 265.2, p < .001. As noted in Figure 2, the prevalence estimates for lifetime cigarette use, alcohol use, and marijuana use for U.S.-born youth were 58.5%, 63.4%, and 33.3%, respectively, compared to 37.2%, 37.5%, and 12.5% for foreign-born youth. Similarly at Wave 2, U.S.-born youth reported higher rates of past year cigarette use, χ2(1) = 98.9, p < .01, alcohol use, χ2(1) = 109.8, p < .01, and marijuana use, χ2(1) = 202.7, p < .001, than did immigrant youth. As shown in Figure 2, the prevalence estimates for past year cigarette use, alcohol use, and marijuana use for U.S.-born youth (at Wave 2) were 43.3%, 54.3%, and 33.6%, respectively, compared to 27.1%, 36.8%, and 12.2% for immigrant youth.
Figure 2.
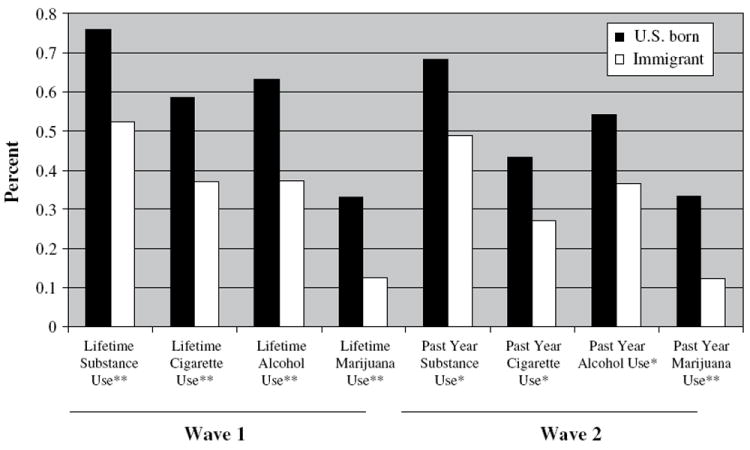
Substance use prevalence estimates for U.S.-born and immigrant Hispanic youth.
* p<0.01; **p<0.001.
Social–contextual functioning
Weighted mean comparisons were conducted to determine whether family connectedness, parental involvement, and school connectedness at Wave 1 differed between U.S.-born and immigrant Hispanic youth. Rao-Scott chi-square tests were conducted to determine whether perceived peer substance use differed between U.S.-born and foreign-born Hispanic youth.
Significant differences emerged for both school connectedness and perceived peer substance use, with U.S. born reporting less school connectedness and more peer using substances. No significant differences between immigrant and U.S.-born youth emerged for family connectedness and parental involvement (Table 1).
Adolescent substance use and perceived peer substance use measurement models
The next step of the analysis was to test the hypothesized ecological model depicted in Figure 1. First, measurement models were estimated to ascertain the feasibility of collapsing multiple binary indicators of adolescent substance use and perceived peer substance use into two separate measurement models (one for substance use and a second for perceived peer substance use) by conducting confirmatory factor analyses using Mplus version 5.1. Although both the adolescent substance use and perceived substance use measurement models were just identified (and hence model fit statistics were not available), results indicated that all three adolescent substance use and all three perceived substance use indicators loaded significantly onto their respective latent constructs. The standardized loadings were .62, .80, and .93 for adolescent alcohol use, adolescent cigarette use, and adolescent marijuana use. The standardized loadings were .85, .72, and .79 for perceived peer alcohol use, perceived peer cigarette use, and perceived peer marijuana use. The perceived peer substance use and adolescent substance use latent variables are represented by circles in Figures 1 and 3.
Figure 3.
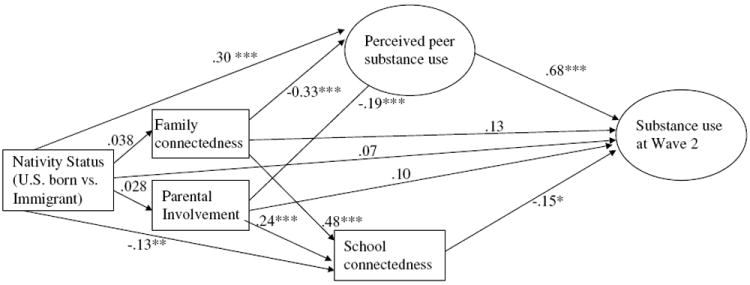
Model of the Wave 1 ecological predictors of Hispanic adolescent substance use at Wave 2. Note. ***p < .001; **p < .01; *p < .05. χ2(9) = 33.5, p <0.01; CFI = .94; RMSEA = 0.02. Note: We controlled for both gender and lifetime substance use at Wave 1. These control variables were not significantly related to the outcome and hence were not included in the figure.
Structural equation models
We estimated the hypothesized structural equation model (Figure 1), controlling for gender and adolescent lifetime substance use at Wave 1, to ascertain the hypothesized relationships between (a) nativity, family functioning (i.e., family connectedness and parental involvement), perceived peer substance use, and school connectedness (measured at Wave 1) and past-year adolescent substance use at Wave 2. The fit of this model to the data was evaluated primarily in terms of the comparative fit index (CFI) and the root-meansquare error of approximation (RMSEA). The chi-square statistic is reported but is not used in interpretation, given that it often indicates significant deviations even when these deviations are quite small [23]. CFI values of .95 or greater, and RMSEA values of .06 or less, are indicative of good model fit [24].
The model provided an adequate fit to the data, χ2 (9) = 33.5, p < .01; CFI = .94; RMSEA = .02. To explore the effects of social–ecological variables within the overall model, we examined the path coefficients for each set of direct and indirect relationships. The results indicated (Figure 3) that perceived peer substance use (B = .68, p < .001) was positively related to adolescent substance use at Wave 2, whereas school connectedness was negatively related to adolescent substance use (B = −.15, p < .05). Neither nativity (B = 0.07, ns), family connectedness (B = 0.13, ns), nor parental involvement (B = 0.10, ns) were significantly related to adolescent substance use.
It is worthy of note that nativity was significantly predictive of substance use at the bivariate level (Figure 2) but was no longer significant when the social–ecological variables were included in the model. This suggests that the effects of nativity on substance use (i.e., the Immigrant Paradox) may have been mediated by one or more of the social–contextual variables in the model. As a result, as a final step of analysis, we tested this possibility empirically. We used the asymmetric distribution of products tests [25] to evaluate whether the effects of nativity status and substance use were mediated by (a) perceived peer substance use, (b) school connectedness, (c) family connectedness, and (d) parental involvement. This test constructs a 95% confidence interval around the product of the two unstandardized path coefficients that comprise each mediating pathway. If the confidence interval for a given product does not include zero, then partial mediation is assumed. This method is more accurate and statistically powerful [26] than traditional methods of testing for mediation.
The indirect path between nativity and substance use through perceived peer substance use was significant (unstandardized point estimate: 0.446; 95% confidence interval [CI ] = 0.250 to 0.642). None of the other indirect paths involving nativity and substance use reached significance: (a) family connectedness, unstandardized point estimate = −0.011; 95% CI = −0.014 to 0.035; (b) parental involvement, unstandardized point estimate = 0.006; 95% CI = −0.014 to 0.027; and (c) school connectedness, unstandardized point estimate = 0.042; 95% CI = −0.006 to 0.089). As a result, we concluded that only perceived peer substance use mediated the effect of nativity on substance use.
Post hoc mediation analyses
Although family connectedness and parental involvement were not directly related to adolescent substance use, we sought to examine whether family connectedness and parental involvement may have been indirectly related to substance use through perceived peer substance use and school connectedness. Post hoc mediation analyses were conducted using the asymmetric distribution of products test. Results indicated two significant mediators of the effect of family connectedness on substance use: perceived peer substance use (unstandardized point estimate = −0.033; 95% CI = −0.045 to −0.021) and school connectedness (unstandardized point estimate = −0.011; 95% CI = −0.020 to −0.002). Results also indicated two significant mediators of the effect of parental involvement on substance use: perceived peer substance use (unstandardized point estimate = −0.037; 95% CI = −0.058 to −0.015) and school connectedness (unstandardized point estimate = −0.011; 95% CI = −0.020 to −0.001).
Discussion
The objective of the current study was to determine whether, and to what extent, ecological processes such as family connectedness, parental involvement, perceived peer substance use, and school connectedness can partially explain the differences in substance use between U.S.-born and immigrant Hispanic adolescents. Such differences represent the “Immigrant Paradox,” whereby immigrants evidence more favorable health outcomes than their U.S.-born counterparts.
As anticipated, the Immigrant Paradox emerged in the present study: immigrant adolescents were significantly less likely to report using cigarettes, alcohol, or marijuana compared to U.S.-born adolescents. This effect of nativity was mediated by perceived peer substance use. Specifically, we found that U.S.-born Hispanic youth were more likely to associate with substance using peers than were foreign-born youth, and consequently, U.S.-born Hispanic youth were more likely to report using substances themselves 1 year later. We also found that perceived peer substance use and school connectedness were directly associated with substance use. This relationship suggests that school bonding and affiliation is protective against adolescent substance use beyond simply discouraging adolescents from affiliating with substance-using peers [17]. The finding that perceived peer substance use was directly related to substance use is consistent with much of the existing literature on non-Hispanic white [27] and Hispanic [17,28] samples, which suggests that the peer context is most proximally related to substance use, whereas other contexts such as the family and peer are less proximal at this time of development. At least two other studies have reported similar findings [29,30]. However, these two other studies have been limited by sampling a nonrepresentative sample of Hispanics in the United States.
Although we did not find a direct relationship between parental connectedness and substance use or between parental involvement and substance use, we did find that perceived peer substance use and school connectedness mediated the relationship between family connectedness and substance use as well as between parental involvement and substance use. This finding is consistent with prior work [31], and extends past research by examining the role of multiple contexts (peer and school) as potential mediators of the relationship between family processes and substance use and by modeling relationships to substance use over time. Coupled with our finding that the Immigrant Paradox, at least with regard to substance use, is explained (to some extent) by family processes (i.e., parental involvement, family connectedness) and affiliation with peers whom the adolescent perceives as using substances, the protective effects of family processes suggest that family processes such as parental involvement and family connectedness may help to counteract the Immigrant Paradox. Specifically, improving family connectedness and parental involvement may help to offset the effects of nativity on affiliation with perceived substance-using peers, and may therefore help to reduce risks for substance use in U.S.-born Hispanic adolescents. However, given that all of the mediators were assessed at the same point in time, future research should replicate these findings before definitive conclusions can be made. Nonetheless, the present findings suggest that family strengthening programs may represent one way to intervene to prevent substance use in U.S.-born Hispanic adolescents [5]. Indeed, previous research has found that behavioral interventions designed to improve family processes in Hispanic families may lead to reductions in substance use, both among immigrant and U.S.-born Hispanic adolescents [32].
Study limitations and strengths
The present results should be interpreted in light of several important limitations. First, this study, and most of the Add Health data as a whole, relies exclusively on self-report measures. Independent reports of family connectedness and parental involvement (e.g., observational tasks) and of substance use (e.g., biological assays) were not available. A second limitation is that both peer substance use and adolescent substance use were reported solely by the adolescent. Consequently, it is possible that the association between (perceived) peer substance use and adolescent substance use may have been inflated by the tendency for adolescents to assume that they and their peers are engaging in similar degrees of substance use (e.g., [33]). Third, the current study examined the prospective association of ecological processes and substance use among a nationally representative sample of Hispanic youth of data collected between 1994 and 1996. There is evidence that demonstrates that the prevalence of substance use among all adolescents (including Hispanics) has declined in the past decade. Additionally, patterns of drug use may have changed in the past 15 years, with drugs such as ecstasy and methamphetamines becoming popular in the late 1990s [1]. Furthermore, there has been massive migration from Latin America to the United States, and this wave of newer immigrants may not necessarily be reflective of the older immigrants. However, more recent cohorts of nationally representative Hispanic samples (with data on family, school, and peer processes) are not available. Nonetheless, the ecological processes associated with substance use progression are still relevant. A final limitation is that, given the moderate sample size, we were not able to stratify the analyses by country of origin or gender. Such research is important to continue exploring the effects of nativity on adolescent substance use. The present study is also characterized by several strengths, including the prospective cohort design, the wide range of social–ecological processes measured, and the nationally representative sample. Another strength of the present study is that we examine both the direct and indirect effects of nativity on Hispanic adolescent substance use.
Conclusions and Implications for Public Health
Despite these limitations, the present study has identified a potential mechanism of ecological processes (although it is important to note that there may be others) that may help to explain the Immigrant Paradox. It appears that immigrant adolescents may be less likely to affiliate with substanceusing peers, and that elements of family functioning may help to offset the effects of nativity on affiliation with substance-using peers, and may therefore help to reduce substance use rates in U.S.-born Hispanic adolescents. In the recent past a call has been made to increase research efforts to understand the etiology of substance use in U.S.- born Hispanic youth and to develop and evaluate prevention interventions for this population based on basic epidemiological research [6]. At the minimum, the findings presented in this study suggest that behavioral interventions to prevent substance use in U.S.-born Hispanic youth should attend to multiple ecological processes, including family and peers. Such interventions have already shown promise in preventing substance use among U.S.-born and foreign-born youth [32-34].
Acknowledgments
This research uses data from Add Health, a program project designed by J. Richard Udry, Peter S. Bearman, and Kathleen Mullan Harris, and funded by grant P01-HD31921 from the National Institute of Child Health and Human Development, with cooperative funding from 17 other agencies. Special acknowledgment is due Ronald R. Rindfuss and Barbara Entwisle for assistance in the original design. Persons interested in obtaining data files from Add Health should contact Add Health, Carolina Population Center, 123 W. Franklin Street, Chapel Hill, NC 27516-2524 (www.cpc.unc.edu/addhealth/contact.html).
References
- 1.Johnston LD, O’Malley PM, Bachman JG, et al. Monitoring the Future: National Results on Adolescent Drug Use: Overview of Key Findings 2006. Bethesda, MD: National Institute on Drug Abuse; 2007. NIH Publication No. 07-6202. [Google Scholar]
- 2.Marotta SA, Garcia JG. Latinos in the United States in 2000. Hispanic J Behav Sci. 2003;25(1):13–34. [Google Scholar]
- 3.Census Bureau. Census Bureau Projects Tripling of Hispanic and Asian Populations in 50 Years; Non-Hispanic Whites May Drop To Half of Total Population. [April 17, 2008]; Available at http://www.census.gov/Press-Release/www/releases/archives/population/001720.html.
- 4.Ramirez RR, de la Cruz GP. The Hispanic Population in the United States: March 2002. Washington, DC: US Department of Commerce, Bureau of the Census, Economics and Statistics Administration; 2003. [Google Scholar]
- 5.Prado G, Szapocnik J, Schwartz S, et al. Drug abuse prevalence, etiology, prevention, and treatment in Hispanic adolescents: a cultural perspective. J Drug Issues. 2008;22:5–36. [Google Scholar]
- 6.Szapocnik J, Prado G, Burlew AK, et al. Drug abuse in African American and Hispanic adolescents: culture, development, and behavior. Annu Rev Clin Psychol. 2007;3:77–105. doi: 10.1146/annurev.clinpsy.3.022806.091408. [DOI] [PubMed] [Google Scholar]
- 7.Pantin H, Prado G, Schwartz SJ, Sullivan S. Methodological challenges in designing efficacious drug abuse and HIV preventive interventions for Hispanic adolescents subgroups. J Urban Health. 2005;82(2):iii92–102. doi: 10.1093/jurban/jti067. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Blake S, Amaro H, Schwartz P, et al. A review of substance abuse prevention interventions for young adolescent girls. J Early Adolesc. 2001;21(3):294–324. [Google Scholar]
- 9.Hussey JM, Hallfors DD, Waller MW, et al. Sexual behavior and drug use among Asian and Latino adolescents: association with immigrant status. J Immigr Minor Health. 2007;9(2):85–94. doi: 10.1007/s10903-006-9020-z. [DOI] [PubMed] [Google Scholar]
- 10.Springer A, Kelder SH, Orpinas P, et al. A cross-national comparison of youth risk behaviors in Latino secondary school students living in El Salvador and the USA. Ethn Health. 2007;12(1):69–88. doi: 10.1080/13557850601002155. [DOI] [PubMed] [Google Scholar]
- 11.Vega W, Alderete E, Kolody B, et al. Illicit drug use among Mexicans and Mexican Americans in California: the effects of gender and acculturation. Addiction. 1998;93(12):1839–50. doi: 10.1046/j.1360-0443.1998.931218399.x. [DOI] [PubMed] [Google Scholar]
- 12.Vega WA, Gil AG, Kolody B. What do we know about latino drug use? Methodological evaluation of state databases. Hispanic J Behav Sci. 2002;24(4):395–408. [Google Scholar]
- 13.Prado G, Schwartz S, Maldonado-Molina M, et al. Ecodevelopmental × intrapersonal risk: substance use and sexual behavior in Hispanic adolescents. Health Educ Behav. 2008 doi: 10.1177/1090198107311278. Epub ahead of print. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Paez MM, Suarez MM. Latinos: Remaking America. Berkeley, CA: University of California Press; 2002. [Google Scholar]
- 15.Barrera M, Biglan A, Ary D, Li F. Replication of a problem behavior model with American Indian, Hispanic, and Caucasian youth. J Early Adolesc. 2001;21(2):133–57. [Google Scholar]
- 16.Dishion TJ, Capaldi DM, Yoerger K. Middle childhood antecedents to progressions in male adolescent substance abuse: an ecological analysis of risk and protection. J Adolesc Res. 1999;14:175–205. [Google Scholar]
- 17.Lopez B, Schwartz S, Prado G, et al. Correlates of early alcohol and drug use in Hispanic adolescents: examining the role of ADHD with comorbid conduct disorder, family, school, and peers. J Clin Child Adolesc Psychol. doi: 10.1080/15374410802359676. in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Galaif ER, Newcomb M, Vega W, et al. Protective and risk influences of drug use among a multiethnic sample of adolescent boys. J Drug Educ. 2007;37(3):249–76. doi: 10.2190/DE.37.3.c. [DOI] [PubMed] [Google Scholar]
- 19.Pantin H, Schwartz SJ, Sullivan S, Prado G, Szapocznik J. Ecodevelopmental HIV prevention programs for Hispanic immigrant adolescents. Am J Orthopsychiatry. 2004;74:545–58. doi: 10.1037/0002-9432.74.4.545. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Coatsworth J, Pantin H, Szapocznik J. Familias unidas: a family-centered ecodevelopmental intervention to reduce risk for problem behavior among Hispanic adolescents. Clin Child Fam Psychol Rev. 2002;5(2):113–32. doi: 10.1023/a:1015420503275. [DOI] [PubMed] [Google Scholar]
- 21.Henrich CC, Brookmeyer KA, Shahar G. Weapon violence in adolescence: parent and school connectedness as protective factors. J Adolesc Health. 2005;37(4):306–12. doi: 10.1016/j.jadohealth.2005.03.022. [DOI] [PubMed] [Google Scholar]
- 22.Sieving RE, Beuhring T, Resnick MD, et al. Development of adolescent self-report measures from the National Longitudinal Study of Adolescent Health. J Adolesc Health. 2001;28(1):73–81. doi: 10.1016/s1054-139x(00)00155-5. [DOI] [PubMed] [Google Scholar]
- 23.Kline RB. Fundamental Concepts. Washington, DC: American Psychological Association; 2006. [Google Scholar]
- 24.Byrne BM. Structural Equation Modeling with AMOS: Basic Concepts, Applications, and Programming. Mahwah, NJ: Lawrence Erlbaum; 2001. [Google Scholar]
- 25.MacKinnon DP, Lockwood CM, Williams J. Confidence limits for the indirect effect: distribution of the product and resampling methods. Multivariate Behav Res. 2004;39:99–128. doi: 10.1207/s15327906mbr3901_4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Fritz MS, MacKinnon DP. Required sample size to detect the mediated effect. Psychol Sci. 2007;18(3):233–9. doi: 10.1111/j.1467-9280.2007.01882.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Dishion TJ, Nelson SE, Bullock BM. Premature adolescent autonomy: parent disengagement and deviant peer process in the amplification of problem behaviour. J Adolesc. 2004;27(5):515–30. doi: 10.1016/j.adolescence.2004.06.005. [DOI] [PubMed] [Google Scholar]
- 28.Schwartz SJ, Coatsworth JD, Pantin H, Prado G, Sharp EH, Szapocznik J. The role of ecodevelopmental context and self-concept in depressive and externalizing symptoms in Hispanic adolescents. Int J Behav Dev. 2006;30(4):359. [Google Scholar]
- 29.Epstein JA, Doyle M, Botvin GJ. A mediational model of the relationship between linguistic acculturation and polydrug use among Hispanic adolescents. Psychol Rep. 2003;93:859–66. doi: 10.2466/pr0.2003.93.3.859. [DOI] [PubMed] [Google Scholar]
- 30.Swaim RC, Bates SC, Chavez EL. Structural equation socialization model of substance use among Mexican–American and White non-Hispanic school dropouts. J Adolesc Health. 1998;23(3):128–38. doi: 10.1016/s1054-139x(98)00068-8. [DOI] [PubMed] [Google Scholar]
- 31.Drabick DAG, Gadow KD, Sprafkin J. Co-occurrence of CD and depression in clinic-based sample of boys with ADHD. J Child Psychol Psychiatry. 2006;47:766–74. doi: 10.1111/j.1469-7610.2006.01625.x. [DOI] [PubMed] [Google Scholar]
- 32.Prado G, Pantin H, Briones E, et al. A randomized controlled trial of a family-centered intervention in preventing substance use and HIV risk behaviors in Hispanic adolescents. J Consult Clin Psychol. 2007;75(6):914–26. doi: 10.1037/0022-006X.75.6.914. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Bauman KE, Ennett ST, Foshee VA, Pemberton M, Hicks K. Correlates of participation in a family-directed tobacco and alcohol prevention program for adolescents. Health Educ Behav. 2001;28(4):440–61. doi: 10.1177/109019810102800406. [DOI] [PubMed] [Google Scholar]
- 34.Martinez CR, Jr, Eddy JM. Effects of culturally adapted parent management training on Latino youth behavioral health outcomes. J Consult Clin Psychol. 2005;73(5):841–51. doi: 10.1037/0022-006X.73.5.841. [DOI] [PubMed] [Google Scholar]