

Abstract
Gingival enlargement is a common finding in a routine dental practice. Though it has many etiological factors, enlargement due to drugs which are administered to treat the systemic problems is of major concern which needs attention. Here, we present a case of nifedipine-induced gingival enlargement and discuss the reason for the enlargement.
KEY WORDS: Gingival enlargement, nifedipine, oral hygeine
Gingival enlargement is a clinical representation of gingival or periodontal diseases. The enlargement of gingiva is associated with more than 20 drugs used for various diseases.[1]
Nifedipine is one of the commonest antihypertensive drugs (calcium channel blockers) used to treat hypertension and some forms of angina. Though it has various side effects, gingival enlargement is the most attended side effect which is of great importance in dentistry. Nifedipine-induced gingival enlargement was first reported in 1984.[2] Various factors were attributed for the overgrowth of gingiva in nifedipine-induced hyperplasia, which include high plaque index (poor oral hygiene), high dose of the drug, genetic factors, individual susceptibility, and interaction between drugs and metabolites with the fibroblasts of gingiva.[3] Here, we present a case with gingival enlargement in two quadrants where few teeth are present, while the other quadrants which were edentulous showed no changes.
Case Report
A 65-year-old male reported to the clinic with a complaint of enlarged gums in relation to the right side upper and lower jaw for the past 2 years. His past medical history revealed that he was hypertensive and was taking Tab. nifedipine 30 mg BID for the past 3 years, as prescribed by his physician. History of the presenting illness revealed that the patient noticed the swelling which started before 2 years and progressed to the present stage. On intraoral examination, there was bulbous enlargement of the gingival mucosa in relation to 13, 14, 44, and 45; surface was lobulated and reddish pink in color [Figure 1]. On palpation, it was nontender and firm in consistency. Assessment of plaque accumulation was done using Silness and Loe plaque index (1964) which gave in a score of 3 (marking abundance of soft matter within the gingival pocket and/or on the tooth and gingival margin). Assessment of gingival inflammation was made using gingival index of Silness and Loe (1963), which gave a score of 1 (which includes mild inflammation, slight change in color, slight edema, and no bleeding on palpation). The gingival hyperplasia was graded by using Angelopoulos and Goaz (1972) criteria, which was graded as grade I (which presents with hyperplastic gingiva extending to the cervical third or less of the anatomic crown).
Figure 1.

Intra oral picture showing the bulbous enlargement of the gingival mucosa in relation to 13, 14, 44,and 45
Discussion
Gingival enlargement due to drugs like nifedipine has various untenable causes. There are various theories postulated in the pathogenesis of gingival enlargement due to nifedipine. Among the antihypertensives, nifedipine showed higher prevalence of gingival enlargement.[4] It starts as an enlargement of interdental papilla and later turns into a lobulated mass or nodules. It may also extend over the crown and reach occlusal heights, thereby interfering with mastication. These growths may aggravate the plaque accumulation and an increase in pocket depth formation, which adds to the problem.
Factors like age, genetic predisposition, pharmacological actions, dose, plaque, and oral hygiene have been attributed for gingival enlargement in nifedipine-induced gingival enlargement. The age is indirectly proportional to the severity of the enlargement. Younger age people show more enlargement because they have greater fibroblastic metabolism and hormonal change than the elderly.[5]
Other factors like increased production of heparin sulfate glycosaminoglycan (HSPG), basic fibroblast growth factor (bFGF), and transforming growth factor-beta (TGF-β) were found to be increased in nifedipine- and phenytoin-induced gingival hyperplasia.[6]
Calcium antagonists like nifedipine block the influx of calcium ions, thereby affecting homeostasis of collagen. The synthesis and degradation of the collagen being altered lead to the abnormal growth.[7] With these factors, an ambiguity exists among different researchers in the pathogenesis and progression of gingival enlargement in nifedipine. Our case showed gingival enlargement where teeth were present. Obviously, the teeth with high plaque index were a key factor in the pathogenesis and progression of the disease in our case. In correlation with this, the edentulous areas did not show any enlargement, which proves that plaque is an essential factor in gingival enlargement due to nifedipine. The same observation was reported by Eslami et al.[8] that edentulous areas did not show signs of enlargement. The other adding features like inflammation and dose of drug accentuate the problem. The histopathology of our patient showed increased plasma cells and the other chronic inflammatory cells, proving plaque to have an inflammatory effect on gingiva resulting in gingival enlargement [Figure 2]. Eslami et al., in their study on 200 patients taking nifedipine, found gingival enlargement in patients with poor oral hygiene and high plaque index.[8]
Figure 2.
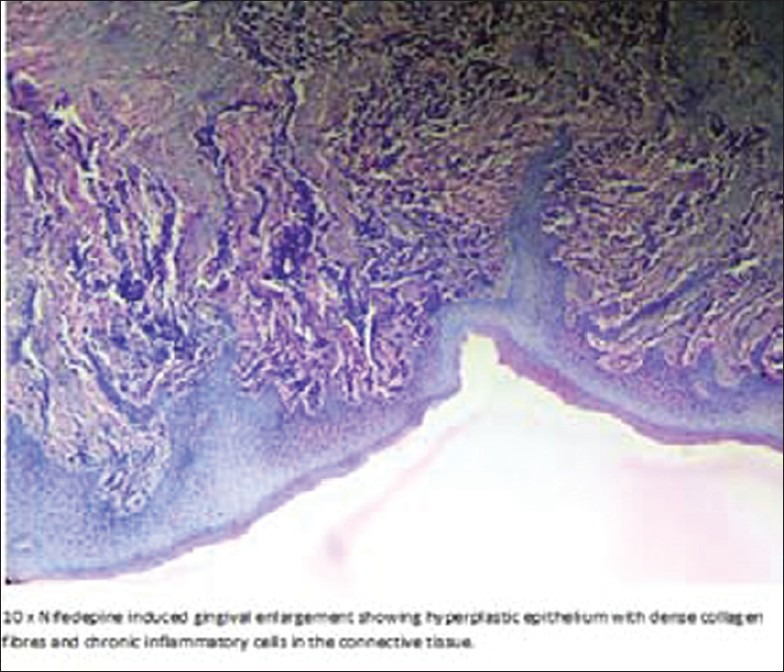
10× Histopathology showing hyperplastic epithelium with dense collagen fibres and chronic inflammatory cells in the connective tissue
The dose of the drug also has an impact on gingival oral growth. Ellis et al.[9] reported 15–316 times increase in nifedipine in the gingival crevicular fluid compared to plasma. They also found that the higher concentration of nifedipine in the gingival crevicular fluid could increase the severity of gingival enlargement.
From earlier studies, it was obvious that good oral hygiene and drug dose were the main factors in gingival enlargement. Gingival hyperplasia was substantially reduced by applying proper prophylactic method accompanied by plaque control measures.[10]
Lu et al. concluded that nifedipine-induced gingival enlargement can be prevented by periodontal treatment along with anti-inflammatory drugs like anti–IL-I β (interleukin-I beta).[11]
It was obvious from our case that poor oral hygiene along with drug dose can increase the gingival growth. Physicians are oblivious while prescribing nifedipine for patients with poor oral hygiene. It should be mandatory that a physician should have a dental opinion before prescribing nifedipine to the patients. Patients with nifedipine therapy need prophylaxis at least once in 3 months and also should have meticulous plaque control measures. It was also proved that increased drug dosage showed increased gingival enlargement, so the physician can consider altering the dose of nifedipine or combine it with other antihypertensives or substitute with other drugs.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Barclay S, Thomason JM, Idle JR, Seymoue RA. The incidence and severity of nifedipine induced gingival overgrowth. J Clin Periodontol. 1992;19:311–4. doi: 10.1111/j.1600-051x.1992.tb00650.x. [DOI] [PubMed] [Google Scholar]
- 2.Ellis JS, Monkman SC, Seymour RA, Idle JR. Determination of Nifedipine in gingival crevicular fluid: A capillary gas chromatographic method for Nifedipine in microlitre volumes of biological fluid. J Chromatogr. 1993;621:95–101. doi: 10.1016/0378-4347(93)80081-e. [DOI] [PubMed] [Google Scholar]
- 3.Eslami M, Baghaii F, Jalayer Nadery N. An Investigation on gingival hyperplasia induced by nifedipine. J Dent (Tehran) 2004;1:33–7. [Google Scholar]
- 4.Gelfand EW, Cheung RK, Grinstein S, Mills G. Characterization of the role for calcium influx in nitrogen-induced triggering of human T-cells. Identification of calcium-dependent and calcium-independent signals. Eur J Immunol. 1986;16:907–11. doi: 10.1002/eji.1830160806. [DOI] [PubMed] [Google Scholar]
- 5.Lu H-K, Chou H-P, Li C-L, Wang M-Y, Wang L-F. Stimulation of Cells Derived from Nifedipine-induced Gingival Overgrowth with Porphyromonas gingivalis Lipopolysaccharide, and Interleukin-1β. J Dent Res. 2007;86:1100–4. doi: 10.1177/154405910708601115. [DOI] [PubMed] [Google Scholar]
- 6.Hancock RH, Swan PH. Nifedipine- induced gingival over growth - Report of a case treated by controlling plaque. J Clin Periodontol. 1992;19:12–4. doi: 10.1111/j.1600-051x.1992.tb01141.x. [DOI] [PubMed] [Google Scholar]
- 7.Lederman D, Lumerman H, Reuben S, Freedman PD. Gingival hyperplasia associated with nifedipine therapy. Oral Surg Oral Med Oral Pathol. 1984;57:620–2. doi: 10.1016/0030-4220(84)90283-4. [DOI] [PubMed] [Google Scholar]
- 8.Margiotta V, Pizzo I, Pizzo G, Barbaro A. Cyclosporine and nifedipine induced gingival overgrowth in renal transplant patients: Correlations with periodontal and pharmacological parameters, and HLA-antigens. J Oral Pathol Med. 1996;25:128–34. doi: 10.1111/j.1600-0714.1996.tb00207.x. [DOI] [PubMed] [Google Scholar]
- 9.Rees TD, Levine RA. Systemic drugs as a risk factor for periodontal disease initiation and progression. Compend Contin Educ Dent. 1995;16:20–42. [PubMed] [Google Scholar]
- 10.Saito K, Mori S, Iwakura M, Sakamoto S. Immunohistochemical localization of transforming growth factor beta, b-FGF and HsgG in gingival hyperplasia induced by Nifedipine and phenytoin. J Periodontal Res. 1996;31:545–55. doi: 10.1111/j.1600-0765.1996.tb00519.x. [DOI] [PubMed] [Google Scholar]
- 11.Seymour RA, Thomason JM, Ellis JS. The pathogenesis of drug-induced gingival overgrowth. J Clin Periodontol. 1996;23:165–75. doi: 10.1111/j.1600-051x.1996.tb02072.x. [DOI] [PubMed] [Google Scholar]