

Abstract
The primary objective of endodontic therapy is to achieve a three-dimensional obturation of the root canal space after adequate preparation of the canal space to remove the tissue debris, microorganisms, and their byproducts. Anatomical variations have frequently been encountered in endodontic practice and have to be adequately managed by the clinician. Missed roots and canals are a major reason for failure of therapy. Technological advances have given the clinician ample opportunity to identify and treat these aberrations successfully. The present report describes a left mandibular second permanent molar requiring root canal treatment, found to have three separate canals in the mesial root. This case demonstrates a rare anatomical configuration and emphasizes the need for the clinician to be aware of and look out for such variations and use adequate diagnostic methodologies prior to and during therapy to detect such variations. The possibility of additional canals, whenever in doubt, should be explored with the assistance of technologies such as those of magnification and illumination and various diagnostic aids. Operator experience has also shown to be a key factor in negotiation and management of these aberrant canal configurations.
KEY WORDS: Elusive canal, mandibular second molar, middle mesial canals, missed canals, root canal anatomy
The primary objective of root canal therapy is to obtain a hermetic seal of the root canal space. Missed canals and spaces within the root canal system may contain microorganisms and their byproducts and may contribute to failure of therapy. A missed canal is neither debrided nor thoroughly sealed, and thus may result in the development or persistence of periapical inflammation.[1]
Therefore, the aim of successful endodontic therapy is to thoroughly debride the canal system of organic substrate, infected pulp tissue, and microorganisms and to three-dimensionally seal the root canal space. Various diagnostic aids and procedures allow us to more thoroughly address the complexities of the root canal system.
There are reports of unusual canal anatomy associated with all teeth, and the mandibular second molars are no exception. Literature on mandibular second molar teeth indicates a variety of different patterns, ranging from single canal with single apical foramen to five canals with four apical foramina.[2] C-shaped canal systems in mandibular second molars have also been reported by various authors.[3–6] The middle mesial canal has been more commonly located in mandibular first molars[7–9] and rarely in mandibular second molars.[10] The clinician must have a thorough understanding of the anatomy of the root canal system and of common variations from normal for a given tooth.
Pomeranz et al. reported the incidence of three canals in the mesial root of the mandibular molars.[7] Reuben et al.[1] evaluated root canal morphology of 125 extracted mandibular first molars in an Indian population by using spiral computed tomography (SCT) and they did not find mandibular molar mesial roots with three canals. Ahmed et al. did a study in Sudanese population using a clearing technique and found that the prevalence of three mesial canals was 4% in mandibular first molars and 10% in mandibular second molars.[11]
Aminsobhani et al.[12] studied the occurrence and location of the middle mesial canal in mandibular first and second molars in relation to other two mesial canals that were treated in private practice and observed that middle mesial canal was located in the middle of the distance between the mesiobuccal and mesiolingual canals. This canal configuration was found in 6 second lower molars and 21 first molars. Middle mesial canal in all of the cases joined to mesiobuccal or mesiolingual canals. None of the teeth consisted of three independent canals with three apical foramina. Beatty and krell[13] described a mandibular first and second molar with three independent canals in the mesial root. The present case is a rare report of root canal therapy in a mandibular second molar containing three independent canals in its mesial root.
Case Report
A 30-year-old male patient reported to the Department of Conservative Dentistry and Endodontics with decayed tooth and associated pain over his left mandibular region. Intraoral examination revealed class I deep carious lesion in 37. The tooth exhibited no mobility, was mildly tender to percussion, and gave a negative response to heat test and a mild reaction to an electric pulp tester. The preoperative diagnostic radiograph of 37 [Figure 1] revealed a deep carious lesion involving the pulp with widening of the apical periodontal ligament space. A provisional diagnosis of necrotic pulp with apical periodontitis was made and endodontic treatment was scheduled.
Figure 1.
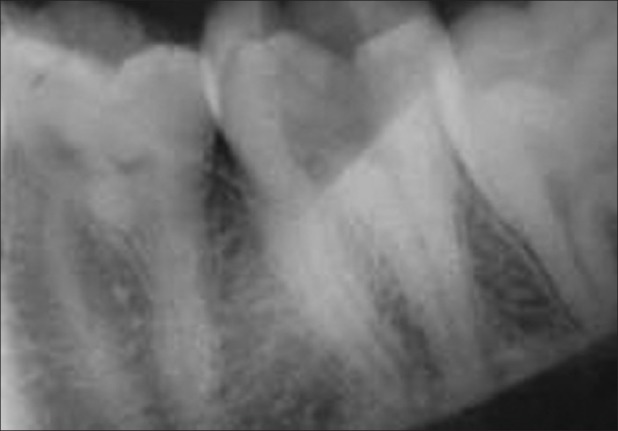
Preoperative radiograph of 37
After administration of local anesthesia and rubber dam isolation, the carious lesion was removed and an adequate endodontic access made. Inspection of the pulp chamber floor showed orifices corresponding to mesiobuccal, mesiolingual, and distal canals [Figure 2]. On careful examination of the groove between the mesiobuccal and mesiolingual canal orifices, the middle mesial canal orifice was identified and the canal subsequently negotiated [Figure 3].
Figure 2.

Intraoral mirror image of 37 with three canals in mesial root
Figure 3.

Intraoral mirror image of 37 with three canals in mesial root
The working lengths were established with an electronic apex locator, and size 10 K files of 21 mm length (Dentsply, Maillefer, Ballaigues, Switzerland) were used to confirm three canals in the mesial root radiographically [Figure 4]. The working length measurement radiograph showed three independent mesial root canals. The canals were instrumented with stainless steel hand instruments – K files of 21 mm length (Dentsply, Maillefer) – and the orifices were shaped with Gates Glidden drills.
Figure 4.

Working length radiograph
Irrigation was done with copious amounts of 3% sodium hypochlorite (Nice chemicals Pvt. Ltd., Cochin, India) and 17% ethylenediaminetetraacetic acid (EDTA; Pulpdent Corporation, Massachusets, USA). The canals after preparation were finally flushed with sterile saline, dried with sterile paper points, and a calcium hydroxide dressing was given. At the subsequent visit after a week, the tooth was asymptomatic and was obturated with gutta percha cones (Dentsply, Maillefer) using AH-Plus sealer (Dentsply DeTrey GmbH, Konstanz, Germany) [Figures 5 and 6].
Figure 5.

37 With master cone
Figure 6.

Post-obturation radiograph of 37
The patient experienced no postoperative sequelae and an appropriate post-endodontic restoration was performed in a subsequent appointment to ensure an adequate coronal seal.
Discussion
There are number of reports that reveal the anatomic variations of root canals in mandibular molars.[1] The presence of a third canal (middle mesial) in the mesial root of the mandibular molars has been reported to have an incidence of 0.95–15%.[1,10,11,14] Although many authors have agreed on the presence of three foramina in the mesial root, only a few have reported the presence of three independent canals, which presents itself as a rare anatomic variant.[15] This additional canal may be independent with a separate foramen or the additional canal may have a separate foramen and join apically with either the mesiobuccal or the mesiolingual canal.[16,17] The clinician should accurately observe the pulp chamber floor to locate possible canal orifices. Pulp chamber floor and wall anatomy provide a guide to determine the root canal morphology. Krasner and Rankow[18–21] made a rational approach to study the relationship of the pulp chamber to the clinical crown and the pulp chamber floor. Their observations, presented in the form of laws, are valuable aids to the clinician searching for elusive canals. Failure to identify extra canals and to recognize any unusual canal configuration is implicated as one of the most common reasons for the failure of endodontic therapy.[22–24] A round bur or an ultrasonic tip can be used for removal of any protuberance from the mesial axial wall, which would prevent direct access to the developmental groove between mesiobuccal and mesiolingual orifices. This developmental groove should be carefully checked with the sharp tip of an endodontic explorer. If depression or orifices are located, the groove can be troughed with ultrasonic tips at its mesial aspect until a small file can negotiate this intermediate canal (Vertucci, 2005).[1,25,26]
Radiographic examination using conventional intraoral periapical views is important for the evaluation of the canal configuration. However, it has its inherent limitation to assess the root canal system completely. Digital radiography at different angles with subsequent image analysis can be used effectively. Computed tomography (CT) imaging has been widely used in medicine since the 1970s and was introduced in the endodontic field in 1990.[27] Recently, cone beam CT (CBCT) imaging has been shown to provide comparable images at reduced dose and costs to be considered as an alternative to multidetector CT imaging in endodontics. Cotton et al.[28] reported a number of useful applications of CBCT imaging in endodontics. La et al. in 2010[29] suggested clinical detection and management of an independent middle mesial canal in mandibular first molar by using CBCT imaging. CBCT imaging prior to initiation of therapy can be done for accurate diagnosis and management of the unusual canal morphology.
Various diagnostic aids like dyes, champagne bubble test, ultrasonics, micro openers and trans-illumination aids, irrigators to improve pulp chamber visibility (Stropko) and observing the chamber for bleeding spots could be used by the clinician as an effective means to locate additional canal orifices.
Newer technologies, such as the dental operating microscope and dental loupes, offer magnification and illumination of the operating field and substantially improve the visualization of root canal orifices (De Carvalho).[28] The present report confirms that the third canal in the mesial root of mandibular second molar does occur and must be sought along the line between the two mesial canals after accessing the pulp chamber and any cervical stenosis in this zone that might cover the opening of the canals, using burs or ultrasonic tips.[30–33]
Conclusion
Identification of these extra canals and their instrumentation is one of the key factors in the prevention of unsuccessful treatment outcomes. In addition to the various diagnostic aids, operator experience has also been identified as a key factor in locating these aberrant canals. The clinician should be aware of the incidence of this type of variation in the mandibular second molar tooth and perform a preoperative radiological assessment from different angles, a proper access preparation, and thorough examination of the pulp chamber to locate and debride all the canals. An accurate clinical evaluation of root canal number and morphology in mandibular second should be done using various diagnostic methodologies with magnification and illumination, which would pave the way for long-term success of endodontic therapy.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Reuben J, Velmurugan N, Kandaswamy D. The evaluation of root canal morphology of the mandibular first molar in an Indian population using spiral computed tomography scan: An in vitro study. J Endod. 2008;34:212–5. doi: 10.1016/j.joen.2007.11.018. [DOI] [PubMed] [Google Scholar]
- 2.Baugh D, Wallace J. Middle mesial canal of the mandibular first molar: A case report and literature review. J Endod. 2004;30:185–6. doi: 10.1097/00004770-200403000-00015. [DOI] [PubMed] [Google Scholar]
- 3.Bond JL, Hartwell GR, Donnelly JC, Portell FR. Clinical management of middle mesial root canals in mandibular molars. J Endod. 1988;14:312–4. doi: 10.1016/S0099-2399(88)80033-5. [DOI] [PubMed] [Google Scholar]
- 4.Cleghorn BM, Goodacre CJ, Christie WH. Morphology of teeth and their root canal system. In: Ingle JI, Backland LK, Baumgarthner JC, editors. Endodontics. 6th ed. Hamilton: BC Decker Incn; 2008. pp. 151–210. [Google Scholar]
- 5.Gulabivala K, Opasanon A, Ng YL, Alavi A. Root and canal morphology of Thai mandibular molars. Int Endod J. 2002;35:56–62. doi: 10.1046/j.1365-2591.2002.00452.x. [DOI] [PubMed] [Google Scholar]
- 6.Grossman IL, Oliet S, Del Rio E. Endodontic Practice. 11th ed. Philadelphia, PA: Leaand Fabringer; 1988. pp. 145–51. [Google Scholar]
- 7.Pomeranz HH, Eidelman DL, Goldberg MG. Treatment considerations of the middle mesial canal of mandibular first and second molars. J Endod. 1981;7:565–8. doi: 10.1016/S0099-2399(81)80216-6. [DOI] [PubMed] [Google Scholar]
- 8.Ricucci D. Three independent canals in the mesial root of a mandibular first molar. Endod Dent Traumatol. 1997;13:47–9. doi: 10.1111/j.1600-9657.1997.tb00010.x. [DOI] [PubMed] [Google Scholar]
- 9.Rahimi S, Shahi S, Lotfi M, Zand V, Abdolrahimi M, Es’haghi R, et al. Root canal configuration and prevalence of C-shaped canals in Mandibular second molars in an Iranian population. J Oral Sci. 2008;50:9–13. doi: 10.2334/josnusd.50.9. [DOI] [PubMed] [Google Scholar]
- 10.Sert S, Bayirli GS. Evaluation of the root canal configurations of the mandibular and maxillary permanent teeth by gender in the Turkish population. J Endod. 2004;30:391–8. doi: 10.1097/00004770-200406000-00004. [DOI] [PubMed] [Google Scholar]
- 11.Ahmed HA, Abu-bakr NH, Yahia NA, Ibrahim YE. Root and canal morphology of permanent mandibular molars in a Sudanese population. Int Endod J. 2007;40:766–71. doi: 10.1111/j.1365-2591.2007.1283.x. [DOI] [PubMed] [Google Scholar]
- 12.Aminsobhani M, Bolhari B, Shokouhinejad N, Ghorbanzadeh A, Ghabraei S, Rahmani MB. Mandibular first and second molars with three mesial canals: A case series – IEJ. 2010;5:36–9. [PMC free article] [PubMed] [Google Scholar]
- 13.Beatty RG, Krell K. Mandibular molars with five canals: Report of two cases. J Am Dent Assoc. 1987;114:802–4. doi: 10.14219/jada.archive.1987.0175. [DOI] [PubMed] [Google Scholar]
- 14.Manning SA. Root canal anatomy of mandibular second molars. Part I. Int Endod J. 1990;23:34–9. doi: 10.1111/j.1365-2591.1990.tb00800.x. [DOI] [PubMed] [Google Scholar]
- 15.Holtzmann L. Root canal treatment of a mandibular first molar with three mesial root canals. Int Endod J. 1997;30:422–3. doi: 10.1046/j.1365-2591.1997.00106.x. [DOI] [PubMed] [Google Scholar]
- 16.Cimilli H, Cimilli T, Mumcu G, Kartal N, Wesselink P. Spiral computed tomographic demonstration of C-shaped canals in mandibular second molars. Dentomaxillofac Radiol. 2005;34:164–7. doi: 10.1259/dmfr/64778606. [DOI] [PubMed] [Google Scholar]
- 17.Goel NK, Gill KS, Taneja JR. Study of root canals configuration in mandibular firstpermanent molar. J Indian Soc Pedod Prev Dent. 1991;8:12–4. [PubMed] [Google Scholar]
- 18.De Carvalho MC, Zuolo ML. Orifice locating with a microscope. J Endod. 2000;26:532–4. doi: 10.1097/00004770-200009000-00012. [DOI] [PubMed] [Google Scholar]
- 19.Krasner P, Rankow HJ. Anatomy of the pulp-chamber floor. J Endod. 2004;30:5–16. doi: 10.1097/00004770-200401000-00002. [DOI] [PubMed] [Google Scholar]
- 20.Maggiore C, Gallottini L, Resi JP. Mandibular first and second molar. The variability of roots and root canal system. Minerva Stomatol. 1998;47:409–16. [PubMed] [Google Scholar]
- 21.Martinez-Berna A. Badanelli P Mandibular first molar with six root canals. Journal of Endodontics. 1985;8:348–52. doi: 10.1016/S0099-2399(85)80043-1. [DOI] [PubMed] [Google Scholar]
- 22.Gao Y, Fan B, Cheung GS, Gutmann JL, Fan M. C-shaped canal system in mandibular second molars Part IV: 3-D morphological analysis and transverse measurement. J Endod. 2006;32:1062–5. doi: 10.1016/j.joen.2006.05.014. [DOI] [PubMed] [Google Scholar]
- 23.Min K. Clinical management of a mandibular first molar with multiple mesial canals: A case report. J Contemp Dent Pract. 2004;15(5):142–9. [PubMed] [Google Scholar]
- 24.Shahi S, Yavari HA, Rahimi S, Torkamani R. Root canal morphology of human mandibular first permanent molars in an Iranian population. JODDD. 2008;2:20–3. doi: 10.5681/joddd.2008.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Vertucci FJ. Root canal morphology and its relationship to endodontic procedures. Endod Topics. 2005;10:3–29. [Google Scholar]
- 26.Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol. 1984;58:589–99. doi: 10.1016/0030-4220(84)90085-9. [DOI] [PubMed] [Google Scholar]
- 27.Tachibana H, Matsumoto K. Applicability of X-ray computerized tomography in endodontics. Endod Dent Traumatol. 1990;6:16–20. doi: 10.1111/j.1600-9657.1990.tb00381.x. [DOI] [PubMed] [Google Scholar]
- 28.Cotton TP, Geisler TM, Holden DT, Schwartz SA, Schindler WG. Endodontic application of cone-bean volumetric tomography. J Endod. 2007;33:1121–32. doi: 10.1016/j.joen.2007.06.011. [DOI] [PubMed] [Google Scholar]
- 29.La SH, Jung DH, Kim EC, Min KS. Identification of Independent Middle Mesial Canal in Mandibular First Molar Using Cone-Beam Computed Tomography Imaging. J Endod. 2010;237:1–4. doi: 10.1016/j.joen.2009.11.008. [DOI] [PubMed] [Google Scholar]
- 30.Vertucci FJ, Williams RG. Root canal anatomy of the mandibular first molar. J N J Dent Assoc. 1974;48:27–8. [PubMed] [Google Scholar]
- 31.Walker RT. Root form and canal anatomy of mandibular first molars in a southern Chinese population. Dent Traumatol. 1988;4:19–22. doi: 10.1111/j.1600-9657.1988.tb00287.x. [DOI] [PubMed] [Google Scholar]
- 32.Weine F. The C-Shaped Mandibular Second Molar: Incidence and other Considerations. J Endod. 1998;24:72–6. doi: 10.1016/s0099-2399(98)80137-4. [DOI] [PubMed] [Google Scholar]
- 33.Fan W, Fan B, Gutmann JL, Fan M. Identification of a C-shaped canal system in mandibular second molars-Part III: Anatomic features revealed by digital substration radiography. J Endod. 2008;34:1187–90. doi: 10.1016/j.joen.2008.06.013. [DOI] [PubMed] [Google Scholar]