

Abstract
The use of ultrasonic vibrations for the cutting of bone was first introduced two decades ago. Piezoelectric surgery is a minimally invasive technique that lessens the risk of damage to surrounding soft tissues and important structures such as nerves, vessels, and mucosa. It also reduces damage to osteocytes and permits good survival of bony cells during harvesting of bone. Grafting with intraoral bone blocks is a good way to reconstruct severe horizontal and vertical bone resorption in future implants sites. The piezosurgery system creates an effective osteotomy with minimal or no trauma to soft tissue in contrast to conventional surgical burs or saws and minimizes a patient's psychological stress and fear during osteotomy under local anesthesia. The purpose of this article is to describe the harvesting of intraoral bone blocks using the piezoelectric surgery device.
KEY WORDS: Block bone graft, piezosurgery, ridge augmentation
The periodontally compromised anterior maxilla, with its thin buccal plate, is a challenging site for restoration. The adequate volume of bone is one of the critical factors for successful osseointegration and long-term retention of endosseous dental implants.[1,2] In such situations, osseous ridge augmentation procedures often are necessary for predictable implant therapy.[2] Autogenous bone remains the “gold standard” technique for grafting. To create the necessary osteotomy, clinicians have used variable surgical burs or saws; they cut bone very effectively, but can cause soft tissue lacerations or burns during osteotomy if the surgeon does not pay close attention. In addition, the noise and macrovibrations can cause fear and stress in patients when surgery is performed with local anesthesia.[3]
To overcome this, a novel surgical approach using piezoelectric device has been introduced in the field of periodontology and oral implantology. The purpose of this study is to describe the efficacy and safety of piezoelectric surgery during intraoral harvesting of bone blocks.
Case Report
A 19-year-old female sought treatment at our department complaining of a missing right maxillary incisor. Clinical and radiological (panoramic and periapical) examinations revealed that the alveolar ridge height was normal. Ridge mapping showed only 2 mm of bucco-lingual bone (Seibert class I defect) [Figures 1 and 2]. Adequate zone of keratinized gingiva was present. Bucco-lingual atrophy of the edentulous alveolar ridge made it impossible to place an implant in this area. It was decided to augment the alveolar crest horizontally. The mandibular symphysis area was selected as the donor site for augmentation.
Figure 1.

Preoperative buccal view
Figure 2.

Preoperative occlusal view
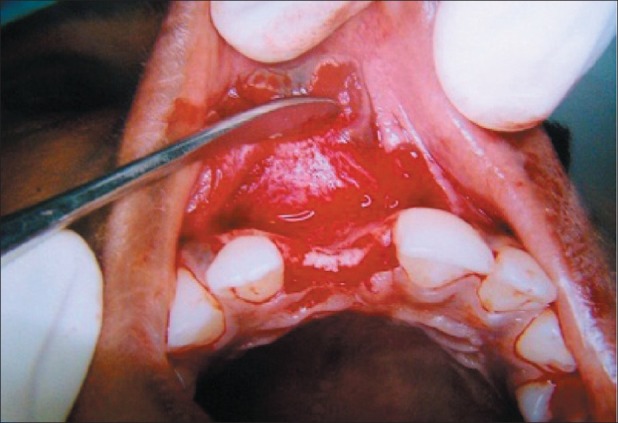
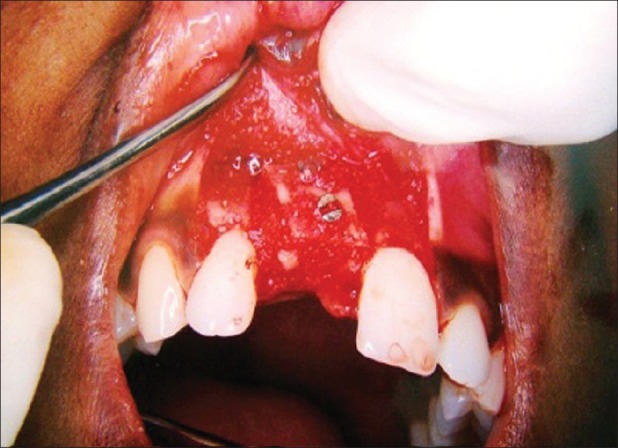
Under local anesthesia, access to surgical site was obtained by crestal incision and by mesial and distal vertical releasing incision on facial side [Figure 3]. A full thickness flap was raised to expose the defect [Figure 4]. Subsequently, a monocortical autogenous bone graft was obtained from the symphysis area of the mandible by using piezosurgery unit [Figures 5 and 6]. Before placing the autogenous graft onto the missing tooth area, the recipient site was perforated to induce vascularity. Then, block bone graft was placed in the recipient site and screwed with a 9-mm titanium miniplate screw [Figure 7], and small gaps in the edge of the autogenous bone graft was also filled [9/26/2012]. A tension-free suturing was done for primary closure of the elevated flap. Donor and recipient site were sutured using horizontal mattress suture with simple loop for proper closure of flap [Figures 9 and 10]. Medications prescribed for postoperative use by the patients included amoxicillin 500 mg and paracetamol 650 mg thrice a day for 5 days. Chlorhexidine mouthwash of 0.2% was prescribed for use after surgery.
Figure 3.

Crestal incision with mesial and distal vertical releasing incision
Figure 4.
After flap reflection
Figure 5.
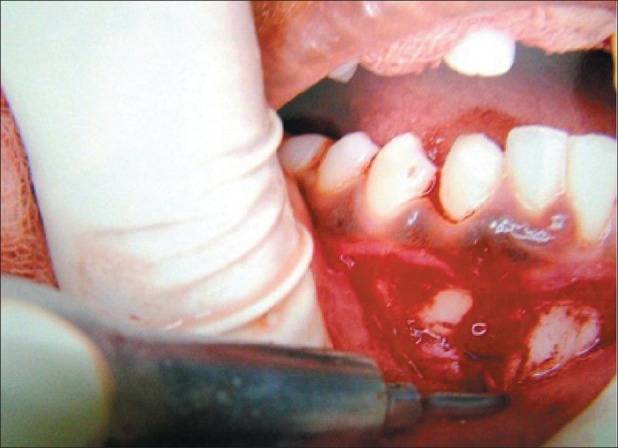
Harvesting of block bone graft by piezosurgery. We can see blood-free zone and good visibility
Figure 6.
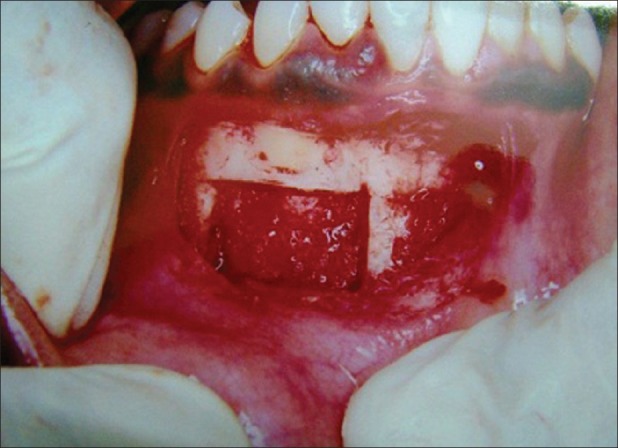
After harvesting of block bone graft
Figure 7.

Placement of graft to recipient site with miniplating screw
Figure 8.
Osseograft placed margins of block bone graft
Figure 9.

Suture of recipient site
Figure 10.

Suture of donor site
The patient was reviewed after a week. There was no postoperative swelling, less patient discomfort, and uneventful healing [Figures 11 and 12]. Six months postoperatively, bone mapping revealed that the patient gained bucco-lingual width of about 5 mm which was sufficient for implant placement.
Figure 11.

1-week postoperative occlusal view
Figure 12.

1-week postoperative buccal view
Discussion
Compared with traditional rotary instrumentation, piezosurgery requires much less hand pressure. This results in enhanced operator sensitivity and control, indicating that the clinician can develop a better feel and precision for the cutting action because of microvibration of cutting tip. The cutting action is less invasive, producing less collateral tissue damage, which results in better healing.[4,5] The piezosurgery system can split a very narrow ridge with minimal loss or perforation of bone.[3] Owing to its cavitation effect on physiological solutions (e.g. blood), piezosurgery creates a virtually bloodless surgical site that makes visibility in the working area much clearer than with conventional bone cutting instruments. Unlike conventional burs and micro saws, piezosurgery inserts do not become hot, which again reduces the risk of postoperative necrosis.[6] In addition, surgical access is easier in the deep oral cavity in comparison to surgical burs which use a straight handpiece. The piezosurgery device makes a precise and tactile-controlled osteotomy.
The ultrasounds of the piezosurgery unit have been developed specifically for cutting bone tissue and have the advantage of not working once they touch soft tissue (and therefore not causing any nerve damage). It can be used in sinus lift procedure to prevent Schneiderian membrane perforation.[7] High-frequency oscillations between 24,000 and 29,500 Hz, modulated with a low frequency between 10 and 60 Hz, enable efficient and controlled use and improve the healing of the tissue.
Piezoelectric surgery uses a specifically engineered surgical instrument characterized by a surgical power that is three times higher than that of normal ultrasonic instruments. This transfers a significantly higher working level ultrasound, and osteotomy can be performed even when the bone is highly mineralized. This allows the cut to be made quickly, and for this reason, excessive increases in bone temperature are impeded. Furthermore, the physiologic solution can easily cool down the bone.[7]
Conclusion
Piezoelectric surgery is an innovative device for general practitioners and experienced oral surgeons for implantology, periosurgery, endodontic surgery, and oral surgery. Compared to other osteotomy instruments, the advantages of ultrasonic surgical instruments are: 1) micrometric bone cut, 2) selective cut, and 3) clear surgical field. Its microvibrations cut hard tissue with precision and accuracy. Its microvibration cuts hard tissues with precision and reduces undesired bone cutting. Insignificant noise and vibrations compared to the ones by rotary bur or saw provide better comfort to patients.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Albrektsson T, Dahl E, Enbom L, Engevall S, Engquist B, Eriksson AR, et al. Osseointegrated oral implants: A Swedish multicenter study of 8139 consecutively inserted Nobelpharma implants. J Periodontol. 1990;59:287. doi: 10.1902/jop.1988.59.5.287. [DOI] [PubMed] [Google Scholar]
- 2.Brugnami F, Caiazzo A, Leone C. Local Intraoral Autologous Bone Harvesting for Dental Implant Treatment: Alternative Sources and Criteria of Choice. Keio J Med. 2009;58:24–8. doi: 10.2302/kjm.58.24. [DOI] [PubMed] [Google Scholar]
- 3.Sohn D-S, Ahn M-R, Lee WH, Yeo DS, Lim SY. Piezoelectric Osteotomy for Intraoral Harvesting of Bone Blocks. Int J Periodontics Restorative Dent. 2007;27:127–31. [PubMed] [Google Scholar]
- 4.Aro H, Kallioniemi H, Aho AJ, Kellokumgo-Lehtinen P. Ultrasonic device in bone cutting: A histological and scanning electron microscopical study. Acta Orthop Scand. 1981;52:5–10. doi: 10.3109/17453678108991750. [DOI] [PubMed] [Google Scholar]
- 5.Vercellotti T, Crovace A, Palermo A, Molfetta A. The piezoelectric osteotomy in orthopedics: Clinical and histological evaluations (Pilot study in animals) Mediterranean J Surg Med. 2001;9:89–96. [Google Scholar]
- 6.Horton JE, Tarpley TM, Jr, Wood LD. The healing of surgical defects in alveolar bone produced with ultrasonic instrumentation, chisel and rotary bur. Oral Surg Oral Med Oral Pathol. 1975;39:536–46. doi: 10.1016/0030-4220(75)90192-9. [DOI] [PubMed] [Google Scholar]
- 7.Vercellotti T, Paoli SD, Nevins M. The Piezoelectric Bony Window Osteotomy and Sinus Membrane Elevation: Introduction of a New Technique for Simplification of the Sinus Augmentation Procedure. Int J Periodontics Restorative Dent. 2001;21:561–7. [PubMed] [Google Scholar]