

Abstract
Background:
Hypodontia is the most common dental anomaly and might cause clinical complications. The aim of this study was to assess the prevalence and pattern of congenital missing in the permanent dentition dentition (excluding third molars), among Iranian orthodontic patients.
Materials and Methods:
In this descriptive cross-sectional study, all approved panoramic radiographs of 3374 orthodontic patients (aged 10 to 20 years old), who had visited the Orthodontic Departments of all Tehran Dentistry Universities and 10 private clinics during the years 1999 to 2009 were investigated, to establish the prevalence of hypodontia in the permanent dentition (excluding third molars). The data were analyzed using a chi-square test (α = 0.01).
Results:
Included were 2012 female and 1362 male patients. The prevalence of hypodontia was 5.21% (5.86% in females, 4.25% in males). The difference between the genders in terms of missing teeth was not significant (P = 0.202). A total of 298 teeth were missing (166 in females, 132 in males). The average of missing per individual was found to be 1.69 (1.40 missing for each girl, 2.32 for each boy). There was no significant difference between the number of missing teeth in males and females (P = 0.160). The most common missing teeth were maxillary lateral incisors (37.2%), mandibular second premolars (22.1%), and mandibular central incisors (10.7%). In both unilateral and bilateral hypodontia cases, the maxillary lateral had the highest prevalence of missing, followed by the mandibular second premolar. Missing was significantly more frequent (P = 0.001) in the maxilla (5.3%) compared to the mandible (3.5%).
Conclusion
Out of every 20 Iranian orthodontic patients, one might have some missing permanent teeth, needing early attention. Hypodontia was more prevalent in females (though not significantly) and in the maxilla. Although more females were affected, the number of missing per individual was greater in males.
Keywords: Hypodontia (congenital missing of teeth), permanent dentition, prevalence
INTRODUCTION
Hypodontia, or congenital missing (CM) of six teeth or less, has been reported as the most common dental anomaly.[1–3] It may detrimentally affect the aesthetics and function.[3–6] Additionally, it may accompany other conditions such as delayed eruption, tooth-size anomalies, retained primary teeth, ectopic canine eruption, and abnormal dental morphologies, such as, taurodontism and peg-shaped maxillary lateral incisors.[2,3,7–10]
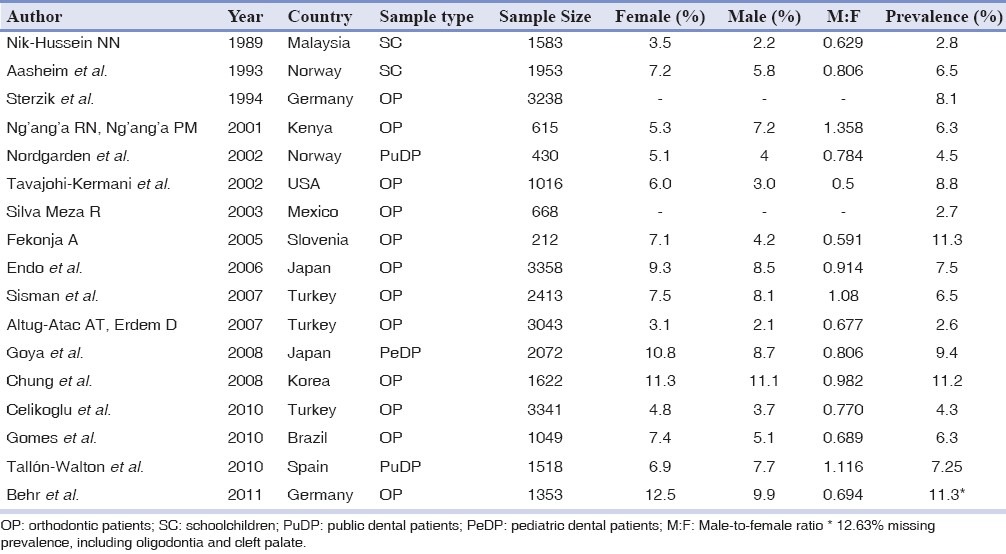
Absence of anterior teeth or CM of more than two teeth in the same quadrant may be an indication for the existence of a need for orthodontic treatment.[11,12] Therefore, investigating the prevalence of hypodontia is of significant clinical value, in terms of early diagnosis and effective treatment planning.[4,13] This would be essential in preventing complications of hypodontia, including periodontal damage, malocclusion, and lack of alveolar growth.[10,12,14] The literature consists of numerous studies on the prevalence of hypodontia (excluding third molars) in the permanent dentition, among different populations [Table 1],[1,3,6,8–10,12,13,15–23] reporting prevalence rates of up to 11.3%.[15,19] The differences in frequencies could be explained by the variety in samples with respect to measuring techniques—different methods of radiography and clinical examinations, age, gender, geographic or demographic profiles,[2,3,11,12] and ethnic backgrounds.[5,7,11] Evolutionary changes might as well contribute to the differences; some investigators suggested that hypodontia had increased in prevalence through time,[2,12] whereas, some studies do not support this.[10,11,24] It should be noted, however, that such a potential increase in frequency might as well be attributed, in part, to the advancements in diagnostic criteria and tools.[2] Despite numerous studies in this matter, the literature lacks comprehensive studies regarding hypodontia among the Iranian population. Hence, this study was performed to describe the prevalence and pattern of CM among 3374 Iranian orthodontic patients, during the years 1999 to 2009.
Table 1.
Prevalence of hypodontia in different populations
MATERIALS AND METHODS
This descriptive cross-sectional study was performed on Iranian patients of age 10 to 20 years. All the subjects were referred, between the years 1999 and 2009, to the dental schools of Tehran, in addition to 10 private orthodontic clinics, in Tehran (which had been selected based on cluster sampling) for orthodontic consultation and / or treatment. All available patient records filed during 1999 – 2009 at the mentioned clinics were evaluated. The exclusion criteria comprised the presence of oligodontia or anodontia, any syndromes, any history of systemic diseases, tooth extractions, trauma, poor image quality, or incomplete patient files. The study protocol was ethically approved by the research committees of all the involved universities.
The overall prevalence of hypodontia in the permanent dentition (excluding missing third molars), as well as its pattern of occurrence regarding the involved sides (left vs. right / anterior vs. posterior), tooth types, and gender were investigated twice by a dentist. Images that were difficult to interpret were assessed by an experienced orthodontist as well.
Reliability of the method
After four months, 315 difficult-to-interpret images and 1120 randomly selected cephalographs were evaluated by both observers. According to the Cohen's Kappa, there were 92% inter-observer (P < 0.001) and 93% intra-observer agreements (P < 0.001). There was 100% consensus about the prevalence of hypodontia. The highest rate of inter-observer bias was present in distinguishing the mandibular central from the mandibular lateral incisors, with 78% agreement (P < 0.001).
Statistical analysis
Descriptive statistics were calculated. The data were analyzed using a chi-square test with power > 0.85. The level of significance was set at 0.01.
RESULTS
The patients’ mean age was 13.9 ± 2.7 years (13.7 ± 2.2 in females, 14.3 ± 3.0 in males). Of them, 2012 (59.7%) were females and 1362 (40.3%) were males. Congenital missing was observed in the permanent dentition of 176 orthodontic patients (5.21% of the sample, 95% confidence interval for the prevalence = 4.4 to 6.0%) including 118 females (5.86% of females) and 58 males (4.25% of males, male-to-female ratio = 1:1.38). There was no significant difference between the prevalence of hypodontia in males and females (P = 0.202).
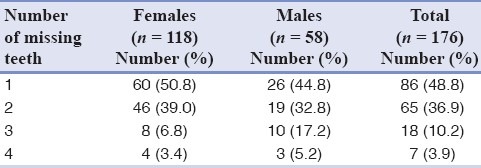
A total of 298 teeth (excluding third molars) were missing (166 in females and 132 in males). Therefore, an average number of 1.69 missing teeth per individual was calculated (average of 1.40 missing teeth for each girl, and 2.32 missing teeth for each boy). The most common tooth types were the maxillary lateral incisor (37.2%), the mandibular second premolar (22.1%), and the mandibular central incisor (10.7%, [Figure 1]). Among the individuals with hypodontia, 85% had congenital missing of one or two teeth (P=0.000, [Table 2]). There was no significant difference between the number of missing teeth in males and females (P=0.160, [Table 2]).
Figure 1.
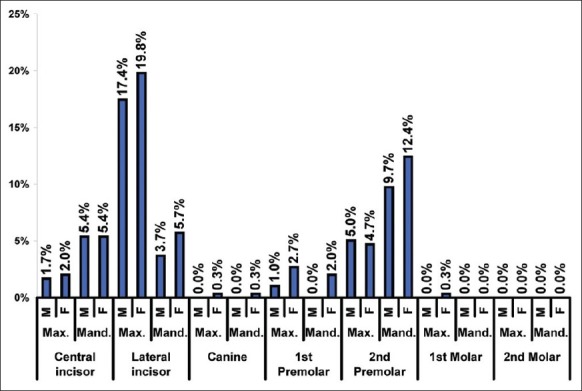
Frequency distribution (%) of the missing teeth (n = 298). Max. = Maxilla; Mand. = Mandible; F = Female; M = Male
Table 2.
Distribution of the number of missing teeth
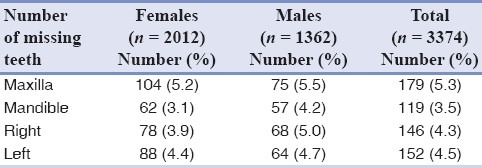
The prevalence rates for CM in the maxilla and mandible were 5.3 and 3.5% (n = 3374 maxillae + 3374 mandibles, P=0.001, [Table 3]), respectively. The difference between maxillary and mandibular missing teeth in males and females was not statistically significant (P=0.301, [Table 3]). Also no significant differences were seen between the right and left sides of males and females (P=0.437, [Table 3]), and in the right and left sides of the overall population (P=0.728, [Table 3]). Hypodontia prevalence in the right and left quadrants (n=3374 left + 3374 right quadrants) was 4.3 and 4.5%, respectively [Table 3]. The difference was not significant (P=0.691).
Table 3.
The number of missing teeth with respect to the affected jaws and sides
There were 73 anterior and 113 posterior missing teeth. These were not significantly different (P=0.319).
Bilateral hypodontia was observed in 78 patients (44.3%). The most common bilateral missing teeth were the maxillary lateral incisor (55.8%) and the mandibular second premolar (22.0%). Of the teeth missing bilaterally, 18 pairs were missing simultaneously in the maxilla and mandible, among which, the second premolar was the most frequently absent tooth (38.8%). The lateral incisor was the most frequent unilaterally missing tooth (39.7%) followed by the mandibular second premolar (36.7%).
DISCUSSION
Environmental and genetic factors contribute to the occurrence of hypodontia.[5] These include infection, trauma, and medicines, as well as genes associated with certain syndromes.[2,4,5,7] Considering the high frequency of hypodontia and its serious aesthetical, physiological, functional, and even emotional complications (particularly during the turbulent adolescence years),[5] its early diagnosis seems to be necessary for enabling clinical teams to plan alternative preventive multidisciplinary treatment modalities.[5,7,10,12,14] For example, pediatric or general dentists can facilitate treatments by diagnosing CM of primary teeth and through early referrals of patients; as absence of primary teeth is highly associated with missing of permanent successors.[5,11] They might also ensure retention of the reduced teeth number,[5] in cases such as palatal impaction of maxillary[ canines caused by missing laterals, in which, early extraction of deciduous canines might guide the eruption of the permanent ones in the correct position.[25]
The participants’ age might confound the results. Calcification of teeth usually last until the age 9 or 10 (particularly in boys). In addition, occasionally, mineralization of premolars may be delayed.[11,12,20,23] Therefore, until the age 10, the absence of premolars in radiography cannot certainly indicate congenital missing,[11,12,20] and thus reading images of children before 10 years of age might reduce the reliability. This is supported by another study, which revealed that prevalence of hypodontia in a population of children at the age seven was determined to be higher than its prevalence in the same population documented two years later.[12] Delayed development of premolars might also disrupt the findings in terms of the most frequently missing teeth, as studies with younger subjects might show higher prevalence of CM in lower premolars.[6] In view of the mentioned factors, patients younger than 10 years were excluded from this study. Furthermore, to increase the reliability of the findings, the authors also excluded all patients with any extraction histories. In some studies, this was overlooked,[2,7,9] while some others only excluded extractions of permanent teeth.[10] Nevertheless, extraction of primary teeth might also cause agenesis in permanent dentition,[2,4,5] and therefore should be excluded as well.
Prevalence
Prevalence of hypodontia may vary based on the ethnicity and continents.[5,7,11] Although diverse results have been reported, in general, it is lower in North America than in Europe, [11] while it might be as small as 1% in the Australian aborigines and African Negroes.[5] The prevalence might differ considerably even in studies conducted in one country (e.g., 2.6 to 6.5% in Turkey,[1,12,18] 8.1 to 11.3% in Germany,[19,22] 7.5 to 9.4% in Japan,[3,16] and 4.5 to 6.5% in Norway).[21,23] The prevalence observed in this study was within the broad range reported in studies on Asian populations (2.6 to 11.2%).[1,3,6,10–12,18]
Prevalence of hypodontia may be affected by population types. Children with hypodontia may be more prone to visit orthodontists compared to individuals without missing, and this might compromise the generalizability of our findings.[6,12] According to the hypodontia definition, radiographic examination is necessary for establishing the prevalence of congenital tooth missing, and clinical examinations may cover merely 70% of actual cases of hypodontia.[3] On the other hand, taking radiographs from children without any therapeutic reasons was not ethical.[1] Therefore, radiographs taken from orthodontic patients were used in this study. All studies conducted recently were as well limited to recruit dental patients only.[1,3,8–10,12,13,15–22] Also, it should be taken into consideration that the rates reported in most studies on orthodontic patients did not differ considerably from those observed in epidemiological studies (less than 9.6%),[12] which implies the validity of the findings of such studies. Furthermore, the authors tried to increase the generalizability by cluster sampling from several private and government clinics, something only present in few studies,[8,21] but not in the other ones.[1,3,9,12,15,16,18,19,22]
Patterns of missing
When a few teeth are missing, as a rule, the most distal tooth of any given type is the most likely to be affected by environment and to be absent.[5,12,26] Overall, the most missing teeth seem to be mandibular second premolars followed by maxillary lateral incisors.[5,11] This pattern may depend on the ethnicity.[1,5,11,16] Studies dealing with epidemiological samples from European and Caucasian populations mostly reported higher missing prevalence of the mandibular second premolar followed by either the maxillary or mandibular central incisors, or the maxillary second premolars.[9,16,19,26] However, the mandibular lateral incisor appears to be the most frequently missing tooth in Japanese people,[16] although there are also some reports of the mandibular second premolars as the most missing teeth.[3] Additionally, CM of the mandibular incisor is supposed to be common in Asian populations.[3]
Consistent with the findings of several other studies on orthodontic patients,[1,8,12,13,15,18,19] the maxillary lateral incisor was the most frequently missing tooth in this sample, followed by the mandibular second premolar. However, some studies on orthodontic patients found a higher hypodontia prevalence for mandibular laterals,[10] and some others observed a greater rate for CM of mandibular second premolars, followed by the maxillary second premolars and maxillary lateral incisors.[20] The differences might root in the minimum age[6] and the ethnicity of the included subjects.[3,9,16,26]
Maxilla versus mandible
According to the literature, there seems to be no overall significant difference between the prevalence of CM in the maxilla and mandible.[11,13] We found, however, that hypodontia was more common in the maxilla; which was in line with some studies,[5,12,15,18] and in contrast to some others, which had found a greater missing rate in the mandible.[10]
Anterior verus posterior
Few studies have evaluated the difference between the hypodontia rate in the anterior and posterior segments.[18,20] Some studies showed a greater level of missing in the anterior segment.[18] However, this study could not find such a difference.
Unilateral versus bilateral
In the present study, bilateral missing was observed about twice as frequently as unilateral missing. This was similar to the results of some studies,[1,13] and contrary to certain other ones.[10] On this subject, a review shows that in general, unilateral missing is more common than bilateral hypodontia. Bilateral missing is seen mostly in the maxillary lateral incisors.[11]
Gender
Gender might affect the prevalence of congenital missing.[7,11] Several investigators have reported a significantly higher missing prevalence among females,[6,11,15] while this study as well as some others did not find such a significant difference between hypodontia prevalence in males and females.[3,13,16,23] Our results were consistent with the male-to-female ratios summarized in reviews of the literature (1:1.37 and 1:1.4).[7,11] The higher rate observed in females might be associated with the biological differences as well as probably the presence of a greater orthodontic treatment need in females with hypodontia, due to their more apparent aesthetical concerns. Nevertheless, the literature does not confirm this, as several studies on schoolchildren showed higher frequencies in females,[6,23] and some other studies did not find such a difference in orthodontic patients,[10] or even reported greater prevalence rates in male orthodontic or .dental patients.[9,12,20] It is also notable that in spite of the fact that more females were affected, each male patient in this study had an average of CM greater than that of each female (2.32 compared to 1.40). Thus, despite the lower number of males with congenital missing, the occurrence of hypodontia might be of more concern in males, as the number of affected teeth is one factor for determination of treatment need.[12]
CONCLUSION
The prevalence of hypodontia was within the range reported previously. The maxillary lateral incisors and mandibular second premolars were the most commonly missing teeth. Maxillary teeth were more prone to be absent. Hypodontia prevalence was not affected by left / right or anterior / posterior types of occurrence. Females were more likely to experience dental agenesis, although not significantly. Nevertheless, due to the higher number of congenital missing per patient in males, hypodontia seemed to be more serious in males, in terms of treatment need.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Altug-Atac AT, Erdem D. Prevalence and distribution of dental anomalies in orthodontic patients. Am J Orthod Dentofacial Orthop. 2007;131:510–4. doi: 10.1016/j.ajodo.2005.06.027. [DOI] [PubMed] [Google Scholar]
- 2.De Coster PJ, Marks LA, Martens LC, Huysseune A. Dental agenesis: Genetic and clinical perspectives. J Oral Pathol Med. 2009;38:1–17. doi: 10.1111/j.1600-0714.2008.00699.x. [DOI] [PubMed] [Google Scholar]
- 3.Goya HA, Tanaka S, Maeda T, Akimoto Y. An orthopantomographic study of hypodontia in permanent teeth of Japanese pediatric patients. J Oral Sci. 2008;50:143–50. doi: 10.2334/josnusd.50.143. [DOI] [PubMed] [Google Scholar]
- 4.Pemberton TJ, Das P, Patel PI. Hypodontia: Genetics and future perspectives. Braz J Oral Sci. 2005;4:695–709. [Google Scholar]
- 5.Nunn JH, Carter NE, Gillgrass TJ, Hobson RS, Jepson NJ, Meechan JG, et al. The interdisciplinary management of hypodontia: Background and role of paediatric dentistry. Br Dent J. 2003;194:245–51. doi: 10.1038/sj.bdj.4809925. [DOI] [PubMed] [Google Scholar]
- 6.Nik-Hussein NN. Hypodontia in the permanent dentition: A study of its prevalence in Malaysian children. Aust Orthod J. 1989;11:93–5. [PubMed] [Google Scholar]
- 7.Wu CC-L, Wong RW-K, Hägg U. A review of hypodontia: the possible etiologies and orthodontic, surgical and restorative treatment options—conventional and futuristic. Hong Kong Dent J. 2007;4:113–21. [Google Scholar]
- 8.Gomes RR, da Fonseca JAC, Paula LM, Faber J, Acevedo AC. Prevalence of hypodontia in orthodontic patients in Brasilia, Brazil. Eur J Orthod. 2010;32:302–6. doi: 10.1093/ejo/cjp107. [DOI] [PubMed] [Google Scholar]
- 9.Tallón-Walton V, Nieminen P, Arte S, Carvalho-Lobato P, Ustrell-Torrent JM, Manzanares-Céspedes MC. An epidemiological study of dental agenesis in a primary health area in Spain: Estimated prevalence and associated factors. Med Oral Patol Oral Cir Bucal. 2010;15:e569–74. doi: 10.4317/medoral.15.e569. [DOI] [PubMed] [Google Scholar]
- 10.Chung CJ, Han JH, Kim KH. The pattern and prevalence of hypodontia in Koreans. Oral Dis. 2008;14:620–5. doi: 10.1111/j.1601-0825.2007.01434.x. [DOI] [PubMed] [Google Scholar]
- 11.Polder BJ, Van’t Hof MA, Van der Linden FP, Kuijpers-Jagtman AM. A meta-analysis of the prevalence of dental agenesis of permanent teeth. Community Dent Oral Epidemiol. 2004;32:217–26. doi: 10.1111/j.1600-0528.2004.00158.x. [DOI] [PubMed] [Google Scholar]
- 12.Sisman Y, Uysal T, Gelgor IE. Hypodontia.Does the Prevalence and Distribution Pattern Differ in Orthodontic Patients? Eur J Dent. 2007;1:167–73. [PMC free article] [PubMed] [Google Scholar]
- 13.Silva Meza R. Radiographic assessment of congenitally missing teeth in orthodontic patients. Int J Pediatr Dent. 2003;13:112–6. doi: 10.1046/j.1365-263x.2003.00436.x. [DOI] [PubMed] [Google Scholar]
- 14.Kokich VG, Kokich VO. Congenitally missing mandibular second premolars: Clinical options. Am J Orthod Dentofacial Orthop. 2006;130:437–44. doi: 10.1016/j.ajodo.2006.05.025. [DOI] [PubMed] [Google Scholar]
- 15.Fekonja A. Hypodontia in orthodontically treated children. Eur J Orthod. 2005;27:457–60. doi: 10.1093/ejo/cji027. [DOI] [PubMed] [Google Scholar]
- 16.Endo T, Ozoe R, Yoshino S, Shimooka S. Hypodontia patterns and variations in craniofacial morphology in Japanese orthodontic patients. Angle Orthod. 2006;76:996–1003. doi: 10.2319/082905-303. [DOI] [PubMed] [Google Scholar]
- 17.Tavajohi-Kermani H, Kapur R, Sciote JJ. Tooth agenesis and craniofacial morphology in an orthodontic population. Am J Orthod Dentofacial Orthop. 2002;122:39–47. doi: 10.1067/mod.2002.123948. [DOI] [PubMed] [Google Scholar]
- 18.Celikoglu M, Kazanci F, Miloglu O, Oztek O, Kamak H, Ceylan I. Frequency and characteristics of tooth agenesis among an orthodontic patient population. Med Oral Patol Oral Cir Bucal. 2010;15:e797–801. doi: 10.4317/medoral.15.e797. [DOI] [PubMed] [Google Scholar]
- 19.Behr M, Proff P, Leitzmann M, Pretzel M, Handel G, Schmalz G, et al. Survey of congenitally missing teeth in orthodontic patients in Eastern Bavaria. Eur J Orthod. 2011;33:32–6. doi: 10.1093/ejo/cjq021. [DOI] [PubMed] [Google Scholar]
- 20.Ng’ang’a RN, Ng’ang’a PM. Hypodontia of permanent teeth in a Kenyan population. East Afr Med J. 2001;78:200–3. doi: 10.4314/eamj.v78i4.9063. [DOI] [PubMed] [Google Scholar]
- 21.Nordgarden H, Jensen JL, Storhaug K. Reported prevalence of congenitally missing teeth in two Norwegian counties. Community Dent Health. 2002;19:258–61. [PubMed] [Google Scholar]
- 22.Sterzik G, Steinbicker V, Karl N. The etiology of hypodontia. Fortschr Kieferorthop. 1994;55:61–9. doi: 10.1007/BF02174358. [DOI] [PubMed] [Google Scholar]
- 23.Aasheim B, Ogaard B. Hypodontia in 9-year-old Norwegians related to need of orthodontic treatment. Scand J Dent Res. 1993;101:257–60. doi: 10.1111/j.1600-0722.1993.tb01115.x. [DOI] [PubMed] [Google Scholar]
- 24.Flores-Mir C. Increased hypodontia through the twentieth century. Evid Based Dent. 2006;7:15. doi: 10.1038/sj.ebd.6400371. [DOI] [PubMed] [Google Scholar]
- 25.Jacobs SG. The impacted maxillary canine. Further observations on aetiology, radiographic localization, prevention / interception of impaction, and when to suspect impaction. Aust Dent J. 1996;41:310–6. doi: 10.1111/j.1834-7819.1996.tb03139.x. [DOI] [PubMed] [Google Scholar]
- 26.Jorgenson RJ. Clinician's view of hypodontia. J Am Dent Assoc. 1980;101:283–6. doi: 10.14219/jada.archive.1980.0186. [DOI] [PubMed] [Google Scholar]