

Abstract
Segmental clavicle fractures are uncommon injuries. When they do present, they tend to comprise a distal and mid-shaft fracture. A clavicular injury with proximal and distal fractures is a rarer presentation still which is sparsely covered in the literature. These injuries, which have been termed bipolar, are easily missed at presentation and due to their infrequency the optimal method of management for these patients is unclear. We describe the successful non-operative management of a bipolar clavicle fracture and review the existing literature.
Key words: bipolar clavicle fracture, segmental fracture, non-operative management.
Case Report
A 70-year-old female presented to the Emergency Department with pain over the right clavicle following a fall down a flight of seven stairs. She was assessed and managed according to advanced trauma life support protocols with an unremarkable primary survey. On secondary survey she was found to be tender over the medial and lateral aspects of the right clavicle. There was no evidence of pneumothorax, brachial plexus or vascular injury. Radiographs revealed a Jäger and Breitner type I extra-articular distal right clavicle fracture (Figure 1A).1 The medial end of the clavicle was not well visualised on standard radiographs. However, a subsequent computed tomography (CT) scan revealed a co-existing extra-articular Craig 3a fracture of the proximal right clavicle (Figure 1B).2 There were no other significant injuries. As the fractures were virtually undisplaced and in a low-demand patient, a decision was made with the patient's consent to proceed with non-operative management. She was initially immobilised in a broad arm sling and reviewed with serial x-rays in the fracture clinic. Gentle mobilisation was started at 4 week stage. A radiograph and CT scan at two months revealed bridging callus at both fracture sites (Figure 2). By six months she had a full range of pain free movement with minimal bony deformity. A further CT scan at eight months revealed both fractures had united and started to remodel (Figure 3). Two and eight month CT scans were performed to monitor enlarged intrathoracic lymph nodes noted on the original CT, these resolved without intervention and without evidence of malignancy by eight months.
Figure 1.
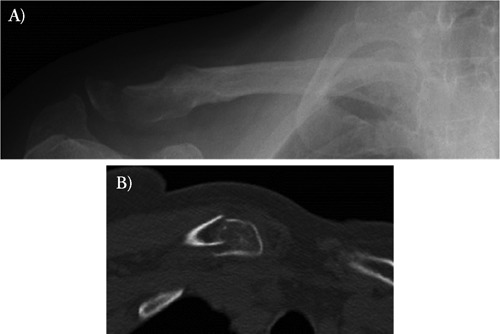
A) Anterior-posterior right clavicle radiograph on presentation clearly showing distal clavicle fracture; B) computed tomography image of proximal clavicle showing fracture which was not clearly evident on plain films.
Figure 2.
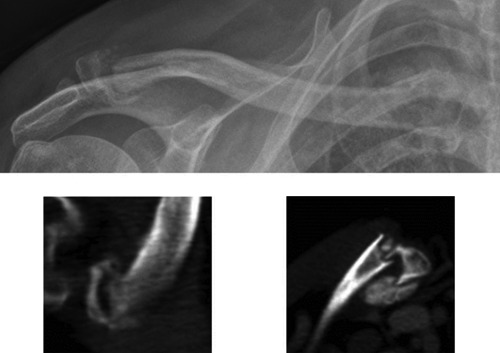
Anterior-posterior radiograph and computed tomography scan images of distal (left image) and proximal (right image) ends of the right clavicle at two months showing callus formation.
Figure 3.
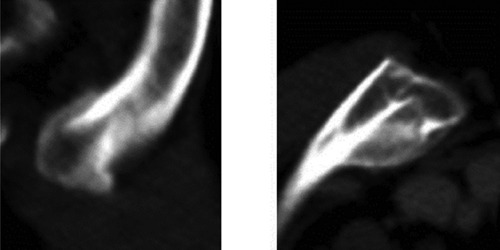
Computed tomography scan images of distal (left image) and proximal (right image) ends of the right clavicle at eight months post-injury showing consolidation of the fracture.
Discussion
Clavicle fractures are common, comprising 2.6–4% of all adult fractures and 44% of shoulder girdle injuries. Of all clavicle fractures, midshaft fractures are most prevalent, comprising between 69% and 82%, distal fractures account for 21% to 28% and proximal fractures comprise between 2% and 3%.3–6 Two peaks of incidence have been described: the first, in young males who sustain midshaft fractures after a direct injury to the clavicle during sports; the second, in elderly females who tend to sustain osteoporosis-related fractures during domestic falls. Fractures of the proximal or distal clavicle are more common in elderly patients.3,4 Segmental clavicle fractures (combined mid-shaft and proximal fracture, or mid-shaft with distal fracture) are uncommon. In a review of 614 clavicle fractures, only 0.8% of patients had segmental injuries.7 Bipolar injuries (combined proximal and distal fractures) are less prevalent still. As far as the authors are aware, only three case reports of such fractures have been published to date.8–10
Isolated clavicle fractures are believed to result from a direct force onto the tip of the shoulder, most commonly the result of a simple fall or sports injury.11 Most medial fractures involve a high-energy impact, which is consistent with our case, following a fall down seven stairs. It has been hypothesised that segmental clavicle fractures are caused by two separate but sequential forces to the clavicle.8,12 Although determining the exact mechanism of injury is not possible, it seems likely that our patient sustained multiple direct injuries, in succession, to the right clavicle during her fall. She reported falling in a stepwise manner rather than directly to the floor from a height.
The majority of clavicle fractures can be treated conservatively. Mid-shaft fractures are generally treated non-operatively, although some authors argue that operative intervention improves functionality and reduces rates of non-union in displaced fractures.13 However, this needs to be weighed against the risk of surgical complications. Undisplaced distal clavicle fractures warrant conservative treatment. However, displaced distal fractures, particularly those medial to the coraco-clavicular ligaments (Neer type II), have a significant risk of non-union and there is a strong argument for them to be managed surgically.14 Many operative techniques have been described for the treatment of these fractures, including coraco-clavicular screws, anatomically contoured locking plates and clavicular hook plates. More recently, arthroscopic ligament reconstruction techniques of treating distal fractures have also been described.6 Proximal clavicle fractures are generally undisplaced and the mainstay of treatment is non-operative.3
Segmental long-bone fractures are generally unstable injuries with a high risk of non-union, and non-operative treatment is often considered unacceptable, with poor outcomes.8,15 Consensus has not been reached on how segmental clavicle fractures should be managed. Most reported cases of segmental clavicle fractures have been treated non-operatively. The literature regarding bipolar clavicle injuries is scarce. One case has been described in a 54 year-old assault-victim, in which the proximal fracture was initially missed. Both proximal and distal fractures were displaced and this was treated with open reduction and internal fixation.8 The authors conclude that all segmental fractures should be considered for operative fixation due to an unstable intermediate fracture segment and a high risk of non-union. A similar case was reported in a 17 year-old male involved in a road traffic accident, sustaining ipsilateral combined medial and lateral clavicle fractures. Both fractures were treated with locking plates, in view of a displaced lateral fracture, medial to the coraco-acromial ligaments (Neer II).10 Although most medial fractures can be managed conservatively, the authors felt that there was a risk of rapid union at one fracture site and delayed or non-union at the other, therefore the medial clavicle fracture was fixed concurrently.9,16 A case in Singapore of a 76-year-old man involved in a motorcycle accident who sustained concomitant proximal and distal fractures of the right clavicle with ipsilateral sterno-clavicular joint dislocation, was treated conservatively with good results. They do not state the degree of displacement of the fractures.10
Conclusions
This case highlights that a segmental injury should always be considered in any patient with a clavicle fracture, with a history of sequential forces to the clavicle. Proximal clavicle fractures comprise 2–3% of clavicle fractures and the diagnosis may be missed.3–5,8,9,16 CT scan is not routinely required for diagnosing medial clavicle fractures but it can be a valuable tool for visualising the proximal clavicle when there is suspicion of an injury which is not evident on plain radiography. Management of bipolar clavicle fractures should be based on individual fracture pattern and patient circumstance. It is important to evaluate the initial displacement of the fracture fragments and, in the case of undisplaced fragments at both fracture sites, conservative management is a viable treatment option.
References
- 1.Jäger M, Breitner S. [Therapy related classification of lateral clavicular fracture] Unfallheilkunde. 1984;87:467–73. [Article in German] [PubMed] [Google Scholar]
- 2.Craig EV. Rockwood CA, Jr, Matsen FA., 3rd. The shoulder. Philadelphia: WB Saunders; 1990. Fractures of the clavicle; pp. 367–412. [Google Scholar]
- 3.Khan K, Bradnock TJ, Scott C, Robinson CM. Current concepts review. Fractures of the clavicle. J Bone Joint Surg Am. 2009;91:447–60. doi: 10.2106/JBJS.H.00034. [DOI] [PubMed] [Google Scholar]
- 4.Nordqvist A, Petersson C. The incidence of fractures of the clavicle. Clin Orthop Relat Res. 1994;300:127–32. [PubMed] [Google Scholar]
- 5.Postacchini F, Gumina S, De Santis P, Albo F. Epidemiology of clavicle fractures. J Shoulder Elbow Surg. 2002;11:452–6. doi: 10.1067/mse.2002.126613. [DOI] [PubMed] [Google Scholar]
- 6.Pujalte GGA, Housner JA. Extremity conditions. Management of clavicle fractures. Curr Sports Medicine Rep. 2008;7:275–80. doi: 10.1249/JSR.0b013e3181873046. [DOI] [PubMed] [Google Scholar]
- 7.Throckmorton T, Kuhn JE. Fractures of the medial end of the clavicle. J Should Elbow Surg Am. 2007;16:49–54. doi: 10.1016/j.jse.2006.05.010. [DOI] [PubMed] [Google Scholar]
- 8.Heywood R, Clasper J. An unusual case of segmental clavicle fracture. J R Army Med Corps. 2005;151:93–4. doi: 10.1136/jramc-151-02-06. [DOI] [PubMed] [Google Scholar]
- 9.Miller D, Smith KD, McClelland D. Case Report: bipolar segmental clavicle fracture. Eur J Orthop Surg Traumatol. 2009;19:337–9. [Google Scholar]
- 10.Pang KP, Yung SW, Lee TS, Pang CE. Bipolar clavicular injury. Med J Malaysia. 2003;58:621–4. [PubMed] [Google Scholar]
- 11.Stanley D, Trowbridge EA, Norris SH. The mechanism of clavicular fracture. A Clinical and biomechanical analysis. J Bone Joint Surg Br. 1988;70:461–4. doi: 10.1302/0301-620X.70B3.3372571. [DOI] [PubMed] [Google Scholar]
- 12.O'Neill PJ, Cosgarea AJ, McFarland EG. Unusual double clavicle fracture in a lacrosse player. Clin J Sport Med. 2000;10:69–71. doi: 10.1097/00042752-200001000-00013. [DOI] [PubMed] [Google Scholar]
- 13.Canadian Orthopaedic Trauma Society. Nonoperative treatment compared with plate fixation of displaced midshaft clavicular fractures. A multicenter-randomized clinical trial. J Bone Joint Surg Am. 2007;89:1–10. doi: 10.2106/JBJS.F.00020. [DOI] [PubMed] [Google Scholar]
- 14.Banerjee R, Waterman B, Padalecki J, Robertson W. Management of distal clavicle fractures. JAAOS. 2011;19:392–401. doi: 10.5435/00124635-201107000-00002. [DOI] [PubMed] [Google Scholar]
- 15.Melis GC, Sotgiu F, Lepori M, Guido P. Intramedullary nailing in segmental tibial fractures. J Bone Joint Surg Am. 1981;63:1310–8. [PubMed] [Google Scholar]
- 16.Robinson CM. Fractures of the clavicle in the adult, epidemiology and classification. J Bone Joint Surg Br. 1998;80:476–84. doi: 10.1302/0301-620x.80b3.8079. [DOI] [PubMed] [Google Scholar]