

Abstract
Background
Acupuncture has been provided in nurse-led group clinics in St Albans since 2008. It is funded by a commissioning group within the National Health Service, on a trial basis, for patients with knee osteoarthritis who would otherwise be referred to an orthopaedic surgeon.
Aim
To evaluate the patients seen in the service's first year of operation and their outcome up to the end of 2010.
Methods
Service evaluation was made of patient data from the referral centre and the acupuncture clinics, including baseline characteristics, attendance data and Measure Yourself Medical Outcome Profile (MYMOP) symptom, function and well-being scores over at least 2 years.
Results
114 patients were offered acupuncture, of whom 90 patients were assessed in the acupuncture clinics. 41 of these were still attending after 1 year and 31 (34%) after 2 years. MYMOP scores showed clinically significant improvements at 1 month for pain (4.2 (SD 1.2) to 2.9 (SD 1.4)), stiffness (4.1 (SD 1.3) to 2.9 (SD 1.3)) and function (4.5 (SD 1.1) to 3.3 (SD 1.2)) which continued up to 2 years. Well-being scores did not change.
Conclusions
This is the first evaluation of nurse-led group (multibed) acupuncture clinics for patients with knee osteoarthritis to include a 2 year follow-up. It shows the practicability of offering a low-cost acupuncture service as an alternative to knee surgery and the service's success in providing long-term symptom relief in about a third of patients. Using realistic assumptions, the cost consequences for the local commissioning group are an estimated saving of £100 000 a year. Sensitivity analyses are presented using different assumptions.
Background
Knee osteoarthritis is common, causing significant pain in 17% of the UK population over the age of 50 years.1 Conservative treatment is sometimes unsatisfactory: core treatment is with exercise,2 which has a relatively small mean effect size (standardised mean difference 0.40, 95% CI 0.3 to 0.5 for pain).3 Non-steroidal drugs are commonly used but evidence of long-term effect is inadequate and adverse reactions are well documented, including gastrointestinal haemorrhage, cardiovascular events such as stroke and nephrotoxicity and cardiovascular events such as stroke.4 Total knee replacement (TKR) surgery is now routine and about 76 500 were performed in England in 2010.5 The operation is effective and cost-effective6 but is not the appropriate choice for everyone who is eligible. The cost, at over £5000, is not trivial.
West Herts Primary Care Trust revised its care pathway in 2006, setting up the musculoskeletal clinical assessment and treatment services (MSK CATS) to improve patient care and reduce referrals and costs. These were operated by four commissioning groups, one of which, the St Albans and Harpenden practice-based commissioning group (STAHCOM), covers the St Albans and Harpenden area with 13 practices and about 180 000 patients. The locality is residential city, suburbs and surrounding countryside. The population is largely middle class and the county of Hertfordshire has a favourable deprivation index, being ranked 139th out of 149 English authorities.7
STAHCOM decided to offer acupuncture to patients who were being considered for referral for TKR. Acupuncture was already provided in primary care St Albans by JF and MR within the NHS,8–10 and so a service with two clinics specifically for knee pain was set up with nurses providing acupuncture to groups of patients, to save costs, see figure 1.11 In a model similar to that in the Royal London Hospital for Integrated Medicine,12 groups are not organised in formal cohorts, but patients simply attend on a rolling recruitment basis, which has benefits including greater flexibility of appointments. The acupuncture service was opened in 2008 on a trial basis, in two locations in GP surgeries in St Albans. The clinics have received national acclaim, winning in 2008 a Prince's Foundation Integrated Health Award as well as an NHS Alliance Acorn Award in the integrated and complementary healthcare category.
Figure 1.

Patients receiving acupuncture in a group clinic in St Albans.
Patients access the service by means of a GP's referral letter which is triaged by the MSK CATS team, including a consultant orthopaedic surgeon, senior physiotherapist (extended scope practitioner) and general practitioners with interest and expertise in musculoskeletal medicine. If surgical referral is a likely outcome, the physiotherapist telephones the patient to assess whether they meet three clinic entry criteria (unrelieved pain, reduced walking distance and night pain).11 Subsequently, this information, the referral letter and the x-ray film are reviewed with the consultant orthopaedic surgeon. Any patients with a clinical or radiological diagnosis of osteoarthritis who are judged to qualify for referral to an orthopaedic surgeon are offered acupuncture treatment first.
The acupuncture service is provided by two clinics and funded by the health service. Acupuncture is given at weekly intervals for 1 month, then reduced progressively to 6 weekly. Hitherto funding has been continued for patients who have found the treatment beneficial.11 Patients who do not respond to manual acupuncture are given electroacupuncture (EA). Acupuncture is discontinued at 6 weeks if there is still no response and the patient referred back to MSK CATS for consideration of further treatment.
The effect of acupuncture is evaluated using MYMOP, a self-completed measure of four items: two symptoms, function on a nominated activity and well-being, each during the previous week.13 It is scored on scales of zero to six, six being worst. For this service, the MYMOP was modified by defining the two scored symptoms as pain and stiffness. Patients completed the modified MYMOP at 1 and 6 months, then every 6 months.
It was decided to evaluate the outcomes of the patients who were referred to the group acupuncture service during its first year of operation. This service evaluation was conducted in parallel with a qualitative study of the acceptability of the clinics.14
Methods
We examined routine clinical data collected from both clinics for all patients assessed in the MSK CATS who were offered acupuncture before referral to an orthopaedic surgeon during the acupuncture service's first year of operation: January to December 2008. Anonymised data on these patients were extracted from computerised health service records up to December 2010—that is, a minimum of 2 years follow-up. Missing data were checked with clinicians. Patients discontinuing treatment were classified as ‘lost to follow-up’ except when improvement was clearly documented as the reason for discharge, in which case they were classified as ‘improved, treatment suspended’. Data on patient flow were presented in a CONSORT (Consolidated Standards of Reporting Trials)-style flow chart.15 Outcomes scores and other data were summarised descriptively and analysed using the t-test function of Excel 2010.
No additional data were sought or collected from patients for the purpose of this report, which thus meets the criteria of service evaluation not requiring independent ethical review.16
Results
Of the 114 patients considered for surgery and offered acupuncture during 2008, 90 (79%) accepted and attended one of the clinics. Patient flow during the following 24 months is shown in figure 2.
Figure 2.

Flow chart of 114 patients considered for knee joint replacement surgery. CATS MSK, musculoskeletal clinical assessment and treatment services
MSK CATS referral service
During the reference year, the MSK CATS service considered surgical referral for 114 patients who had the following characteristics. The mean VAS pain score was 6.1 (SD 2.2). Forty-eight reported night pain, 40 reported none (23 did not reply). Their assessment of their walking ability was: homebound = 7; 10 min (or 100 yards)=26; walk longer but <30 min (or one mile) = 25; at least half an hour (or one mile) = 34; no information = 21. Fifty would accept surgery, four said ‘yes as a last resort’ and 29 would decline.
When asked what were their expectations of treatment, 75 said pain reduction, five said increased mobility and four said surgery. Fifteen did not want acupuncture and requested referral elsewhere instead.
Group acupuncture service
A total of 90 patients (23 men, 26%) were assessed in the two clinics in 2008, with mean age 71 (SD 9.5) years. Duration of symptoms was >5 years in 53/88 (60%), 1–5 years in 26/88 (30%) and <1 year in 8/88 (9%). Baseline modified MYMOP scores for the whole cohort were pain 4.2 (SD 1.3), stiffness 4.3 (SD 1.4), reduced activity 4.6 (SD 1.1) and general well-being 2.9 (SD 1.6). When choosing their ‘worst affected activity’, 65 nominated walking, 15 climbing hills or stairs, five general mobility and five named other activities, including bathing, bowls, cycling, dancing and tennis. Data were missing on three.
The clinics provided these 90 patients with a total of 1489 treatments (mean 16.5 per patient, SD 9.5) up to the end of 2010. Acupuncture was given to both knees in 50 patients, right knee only in 22 and left only in 18.
After 1 month, 84 were still attending the service, of whom 46 continued to receive manual acupuncture and 27 had EA (data missing on 11). After 6 months, 57 (63%) were still attending and MYMOP scores for this group are given in table 1. After 12 months, 41 (46%) were still attending and at 2 years, 31 (34%) still continued acupuncture, having by then received a mean of 27 (SD 4.2) treatments each. Figure 3 shows that the initial improvement in scores was sustained over this period, though these data are somewhat limited by the smaller number of responses in later evaluations.
Table 1.
Measure Yourself Medical Outcome Profile (MYMOP) scores at baseline and 1 and 6 months for those still receiving treatment and providing data at 6 months
| Time | Pain (n = 42) | Stiffness (n = 41) | Activity (n = 42) | General well-being (n = 41) |
|---|---|---|---|---|
| Baseline | 4.2 (1.2) | 4.1 (1.3) | 4.5 (1.1) | 2.9 (1.8) |
| One month | 2.9 (1.4) | 2.9 (1.3) | 3.3 (1.2) | 2.4 (1.4) |
| Six months | 2.5 (1.3) | 2.6 (1.2) | 2.8 (1.4) | 2.1 (1.4) |
Higher scores worse (SD).
Figure 3.
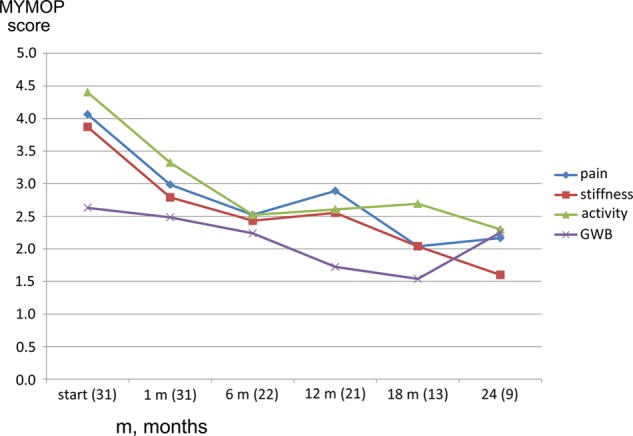
Modified Measure Yourself Medical Outcome Profile (MYMOP) scores over time in the patients who continued treatment for 24 months (number of responses at each time point in parentheses). GWB, general well-being.
Predicting responders
We explored baseline characteristics to see if any might predict the likelihood of response at 6 months. Responders were of similar age (70.8, SD 9.8 years compared with 71.4, SD 9.1 years for those who stopped), marginally less likely to be male (23% compared with 30% of dropouts) and had marginally worse MYMOP scores for symptoms and activity (see table 2). None of these differences was statistically significant.
Table 2.
Comparison of baseline Measure Yourself Medical Outcome Profile (MYMOP) scores of those continuing and those stopping acupuncture at 6 months
| Pain | Stiffness | Activity | General well-being | |
|---|---|---|---|---|
| Continuing (n = 57) | 4.2 (1.2) | 4.1 (1.3) | 4.5 (1.1) | 2.9 (1.8) |
| Stopping (n = 27) | 4.6 (1.3) | 4.7 (1.2) | 4.7 (1.2) | 2.8 (1.4) |
| p Value (t test) | 0.124 | 0.069 | 0.498 | 0.759 |
Higher scores worse (SD).
At 24 months, there were no meaningful differences in age or baseline MYMOP scores between those who were still receiving treatment and those who had stopped (data not shown). Use of EA was not in itself associated with continued benefit, since 29% of those still in treatment at 2 years were receiving EA, compared with 37% at 1 month.
Discussion
About 80% of patients with knee osteoarthritis who attended MSK CATS in 2008 and were considered candidates for TKR surgery were willing to try acupuncture first. Ninety patients were screened for acupuncture in this NHS service offering treatment in groups. Of these 90 patients, we know that at least 31 had not had TKR within the following 2 years.
The strengths of this evaluation are the completeness of MSK CATS and clinic records and the detail of patient follow-up attendance data throughout their association with the clinics. Given the age and health status of many who attended, it is remarkable that only 30% of patients had to be classified as lost to follow-up. The evaluation's limitations include missing MYMOP scores on a proportion of patients owing to pressures on clinic nurses’ time and lack of administrative support and lack of information on the eventual outcome of patients who discontinued acupuncture. Another limitation is due to a subtle shift in reason for referral to MSK CATS over time: GPs started to refer patients to MSK CATS specifically for acupuncture treatment, including some who did not want, or were not fit for, surgery. It was decided that to deny them acupuncture would be unethical and so some patients who do not meet the criteria were included on a case-by-case basis.
Estimating the cost consequences of these acupuncture clinics is necessarily somewhat speculative. We set out our data, assumptions and estimations in the web-based Appendix. Practices charge £20 per treatment, which comfortably covers running costs. The estimated cost to the primary care trust of providing acupuncture for these 90 patients was £16 440 in the first year and about £30 000 over the whole period of this evaluation. The NHS tariff cost of uncomplicated TKR (code 9HB21C) is £5456.17 A total of 41 patients had acupuncture and not surgery in the first 12 months, of whom 31 had not had surgery at the end of 2 years—and anecdotally were unlikely to undergo surgery in the near future since none discussed this with nurses in the clinics. Deferring treatment costs frees up resources for the current year, and health economists reflect this benefit by ‘discounting’ costs at the current rate, which is 3.5%.18
Assuming that only about two-thirds of patients offered surgery would take up the offer in the first year, our ‘best guess’ estimate of realistic cost consequences is that the acupuncture service would achieve savings of about £100 000 a year. Sensitivity analysis using different assumptions suggests that maximum savings might be in the region of £171 000 a year and in the ‘worst-case scenario’ the service could generate net costs of about £7000 a year.
We are reluctant to extrapolate the data from this service evaluation to other health trusts and other settings, but we note that there are four commissioning groups in this primary care health trust and there are about 100 similar trusts in England altogether.
The numbers of recorded episodes of TKR for STAHCOM and the neighbouring three commissioning groups are presented in figure 4. The original data are presented in the web-based Appendix. Rate fluctuations are considerable and likely to be due to many factors, but in the third and fourth years after introduction of the acupuncture service in the STAHCOM commissioning group, this group had the lowest proportional number of TKRs: about 3% lower than the Dacorum area practised-based commissioning group (DACCOM) in 2010 and 10% lower in 2011. The same differences are seen using 2007 or 2008 as baseline, but using 2006 as baseline, STAHCOM shared the lowest place with DACCOM. In addition, orthopaedic surgeons reported to one of us (MB) that referrals from the MSK CATS were more appropriate in STAHCOM than the other commissioning groups, which could be partly due to the availability of acupuncture.
Figure 4.
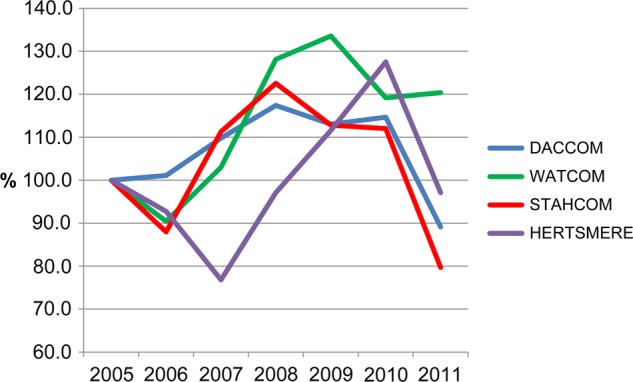
Annual episodes of knee replacement surgery for St Albans and Harpenden practice based commissioning group (STAHCOM) compared with neighbouring groups (data standardised to 2005–6 baseline). Acupuncture clinic started in 2008.
The savings achieved by avoiding TKR in some patients could be used to make acupuncture treatment available for others, even if not specifically to avoid surgery. For example, some decline the offer—as many as 30% of patients in one survey19—and others are not eligible. Criteria for surgery are highly variable and there is no clear indication who will have the best results.20 Although TKR is successful in the sense that revision rates are low, as many as 15% of patients experience severe knee pain 3–4 years later21 and 18% are dissatisfied with the results.22 Experts recommend that all conservative options should be offered before resorting to surgery.20 The evidence published on acupuncture in patients with knee osteoarthritis shows that it is safe23 and effective in reducing pain and improving function,24 thus qualifying it as an appropriate conservative treatment for this condition.
Similar cost savings from reduced use of secondary care through acupuncture have been described before. Three randomised controlled trials of acupuncture for knee pain reported an incidental finding of reduced demand for surgery.25–27 Lindall used (individual) acupuncture in primary care for patients who would otherwise have been referred to orthopaedic or rheumatology outpatients: savings were calculated to be about £232 per patient (1999 figures) in consultation costs alone.28 Other reports have suggested that acupuncture achieves reduced drug expenditure.29 30 Formal economic analyses have assessed cost-effectiveness of acupuncture for knee osteoarthritis as £3889 per quality-adjusted life-year (QALY) for health costs alone31 and €22 314 per QALY from a societal perspective.32
Possible concerns about delaying surgery include risk of clinical deterioration. There is evidence that surgery in patients with a worse condition is less likely to be successful, particularly with valgus deformity progressing beyond 25°.33 It is important to monitor all patients attending such clinics specifically for valgus deformity and for overall function for example with the Oxford Knee Score.34
In conclusion, this first evaluation of nurse-led group acupuncture clinics for patients with knee osteoarthritis, including 2 year follow-up, shows the practicability of offering a low-cost acupuncture service as an alternative to knee surgery and its success in achieving long-term symptom relief in about a third of patients. The realistic cost consequences for the local commissioning group are an estimated saving of about £100 000 a year.
Additional data are published online only. To view this file please visit the journal online (http://dx.doi.org/10.1136/acupmed-2012-010151).
Summary points.
Nurse-led group acupuncture is offered to patients who would be referred for orthopaedic surgery.
80% of patients accept, and 30% who try it gain sufficient symptom relief to avoid surgery.
Savings for this commissioning group were about £100,000 per annum.
Acknowledgments
Julie Brumby ran the MSK CATS and provided data on the first year's patients. James Ferguson and Michael Cannell, both GPs at Midway Surgery, facilitated the clinic at that site. Stephanie Martin-Smith also ran the clinic at Parkbury House Surgery.
Footnotes
Contributors: Concept: JF and MR planned and set up the clinic in Parkbury House surgery; PR James Ferguson and Michael Cannell (see Acknowledgements) set up the clinic in Midway Surgery; MB facilitated the clinics within STAHCOM commissioning group;MR, PR and Stephanie Martin-Smith (see Acknowledgements) delivered the acupuncture and collected the clinic data; Julie Brumby (see Acknowledgements) collected MSK CATS referral service data; AW planned the evaluation, analysed the data, drafted the report and is guarantor for the study.
Competing interests: AW has received lecture fees and travel expenses from the British Medical Acupuncture Society (BMAS) related to the present work. AW is paid by BMAS as editor of the journal Acupuncture in Medicine and receives royalties on books on acupuncture. The Peninsula Medical School received a research grant from BMAS to cover the costs of another researcher for work related to this study. MR has been paid by BMAS for lecturing. PR: no competing interest declared; JF is a partner in one of the practices where a knee clinic takes place and receives payment as a practice for each treatment; MB: no competing interest declared.
Patient consent: Obtained.
Ethics approval: Meets the criteria of service evaluation.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Jinks C, Jordan K, Ong BN, et al. A brief screening tool for knee pain in primary care (KNEST). 2. Results from a survey in the general population aged 50 and over. Rheumatology (Oxford) 2004;43:55–61 [DOI] [PubMed] [Google Scholar]
- 2.National Collaborating Centre for Chronic Conditions Osteoarthritis: national clinical guideline for care and management in adults. London: Royal College of Physicians, 2008 [PubMed] [Google Scholar]
- 3.Fransen M, McConnell S, Bell M. Exercise for osteoarthritis of the hip or knee. Cochrane Database Syst Rev 2008;4:CD004376. [DOI] [PubMed] [Google Scholar]
- 4.Salvo F, Fourrier-Reglat A, Bazin F, et al. Cardiovascular and gastrointestinal safety of NSAIDs: a systematic review of meta-analyses of randomized clinical trials. Clin Pharmacol Ther 2011;89:855–66 [DOI] [PubMed] [Google Scholar]
- 5. www.hesonline.nhs.uk/ (accessed 9 Feb 2012)
- 6.Dakin H, Gray A, Fitzpatrick R, et al. Rationing of total knee replacement: a cost-effectiveness analysis on a large trial data set. BMJ Open 2012;2:e000332. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.The English Indices of Deprivation 2010: County summaries. www.communities.gov.uk (accessed 20 Feb 2012)
- 8.Freedman J. An audit of 500 acupuncture patients in general practice. Acupunct Med 2002;20:30–4 [DOI] [PubMed] [Google Scholar]
- 9.Freedman J, Richardson M. Introducing voluntary donations to fund primary care acupuncture—a user survey. Acupunct Med 2005;23:137–40 [DOI] [PubMed] [Google Scholar]
- 10.Richardson M, Freedman J. A model for acupuncture training in primary care. Acupunct Med 2005;23:135–6 [DOI] [PubMed] [Google Scholar]
- 11.Freedman J, Richardson M. Setting up an acupuncture knee clinic under Practice Based Commissioning. Acupunct Med 2008;26:183–7 [DOI] [PubMed] [Google Scholar]
- 12.Berkovitz S, Cummings M, Perrin C, et al. High volume acupuncture clinic (HVAC) for chronic knee pain—audit of a possible model for delivery of acupuncture in the National Health Service. Acupunct Med 2008;26:46–50 [DOI] [PubMed] [Google Scholar]
- 13.Paterson C, Langan CE, McKaig GA, et al. Assessing patient outcomes in acute exacerbations of chronic bronchitis: the measure your medical outcome profile (MYMOP), medical outcomes study 6-item general health survey (MOS-6A) and EuroQol (EQ-5D). Qual Life Res 2000;9:521–7 [DOI] [PubMed] [Google Scholar]
- 14.Asprey A, Paterson C, White A. ‘All in the same boat’: a qualitative study of patients’ attitudes and experiences in group acupuncture clinic. Acupunct Med 2012. doi: 10.1136/acupmed-2012-010150 [DOI] [PubMed] [Google Scholar]
- 15.Schulz KF, Altman DG, Moher D. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. BMJ 2010;340:c332. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.National Research Ethics Service Defining research. National patient safety agency. London: National Patient Safety Agency, 2010 [Google Scholar]
- 17.Major Knee Procedures for non Trauma Category 2 without CC; March 2011. www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_124356 (accessed 21 Feb 2012)
- 18.NICE Guide to the methods of technology appraisal 2008. Section 5.6.1. http://www.nice.org.uk/media/B52/A7/TAMethodsGuideUpdatedJune2008.pdf (accessed 2 May 2012)
- 19.Mitchell HL, Hurley MV. Management of chronic knee pain: a survey of patient preferences and treatment received. BMC Musculoskelet Disord 2008;9:123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Dieppe P, Lim K, Lohmander S. Who should have knee joint replacement surgery for osteoarthritis? Int J Rheum Dis 2011;14:175–80 [DOI] [PubMed] [Google Scholar]
- 21.Wylde V, Hewlett S, Learmonth ID, et al. Persistent pain after joint replacement: prevalence, sensory qualities and postoperative determinants. Pain 2011;152:566–72 [DOI] [PubMed] [Google Scholar]
- 22.Wylde V, Dieppe P, Hewlett S, et al. Total knee replacement: is it really an effective procedure for all? Knee 2007;14:417–23 [DOI] [PubMed] [Google Scholar]
- 23.Yamashita H. Safety of acupuncture for osteoarthritis of the knee —a review of randomized controlled trials. Acupunct Med 2006;24(Supp):S49–52 [Google Scholar]
- 24.Manheimer E, Cheng K, Linde K, et al. Acupuncture for peripheral joint osteoarthritis. Cochrane Database Syst Rev 2010(1):CD001977. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Christensen BV, Iuhl IU, Vilbek H, et al. Acupuncture treatment of severe knee osteoarthrosis: a long-term study. Acta Anaesthesiologica Scandinavica 1992;36:519–25 [DOI] [PubMed] [Google Scholar]
- 26.Williamson L, Wyatt MR, Yein K, et al. Severe knee osteoarthritis: a randomized controlled trial of acupuncture, physiotherapy (supervised exercise) and standard management for patients awaiting knee replacement. Rheumatology (Oxford) 2007;46:1445–9 [DOI] [PubMed] [Google Scholar]
- 27.Soni A, Joshi A, Mudge N, et al. Supervised exercise plus acupuncture for moderate to severe knee OA: a small randomised controlled trial. Acupunct Med 2012;30:176–81 [DOI] [PubMed] [Google Scholar]
- 28.Lindall S. Is acupuncture for pain relief in general practice cost-effective? Acupunct Med 1999;17:97–100 [Google Scholar]
- 29.Downey P. Acupuncture in the normal general practice consultation: an assessment of clinical and cost effectiveness. Acupunct Med 1995;13:45–7 [Google Scholar]
- 30.Bourne IHJ. Economic aspects of tender spot injection therapy. Acupunct Med 1996;14:114–16 [Google Scholar]
- 31.Whitehurst DG, Bryan S, Hay EM, et al. Cost-effectiveness of acupuncture care as an adjunct to exercise-based physical therapy for osteoarthritis of the knee. Phy Ther 2011;91:630–41 [DOI] [PubMed] [Google Scholar]
- 32.Reinhold T, Witt CM, Jena S, et al. Quality of life and cost-effectiveness of acupuncture treatment in patients with osteoarthritis pain. Eur J Health Econ 2008;9:209–19 [DOI] [PubMed] [Google Scholar]
- 33.Rajgopal A, Dahiya V, Vasdev A, et al. Long-term results of total knee arthroplasty for valgus knees: soft-tissue release technique and implant selection. J Orthop Surg (Hong Kong) 2011;19:60–3 [DOI] [PubMed] [Google Scholar]
- 34.Conaghan PG, Emerton M, Tennant A. Internal construct validity of the Oxford Knee Scale: evidence from Rasch measurement. Arthritis Rheum-Arthritis Care Res 2007;57:1363–7 [DOI] [PubMed] [Google Scholar]