

Abstract
Urinary fistula is an acknowledged complication of partial nephrectomy. We describe a case of a urinary fistula that failed to respond to conventional treatment and the subsequent use of percutaneous Hystoacryl® glue to achieve its resolution.
Case report
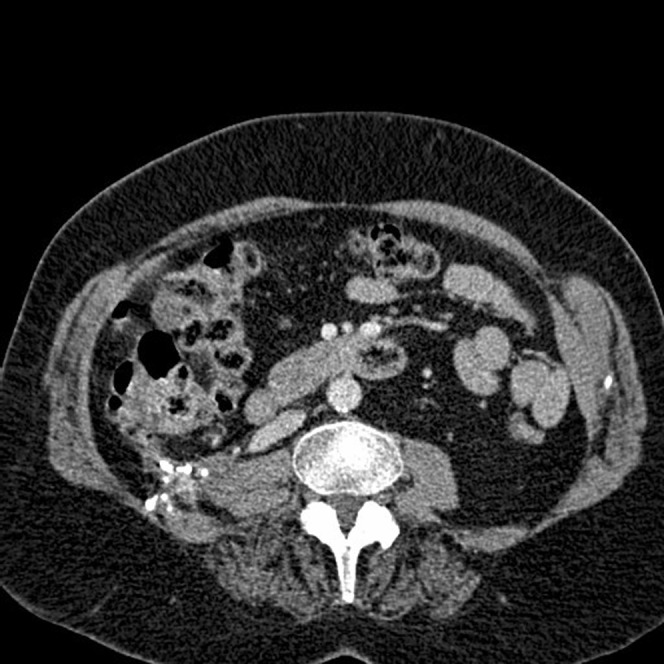
A 57-year-old woman underwent an uncomplicated right lower pole partial nephrectomy for Fuhrman grade 3 pT1NxMx clear cell renal cell carcinoma, through a right loin 11th rib incision. At outpatient review meeting 1 month after discharge, she was well and reported only mild discomfort in the region of the wound. Renal CT after 1 year demonstrated no evidence of disease recurrence; however, a 10 cm diameter urinoma was identified anterior to the right kidney compressing the pelviureteric junction (PUJ) and upper ureter (Figure 1). Her renal function was normal.
Figure 1.
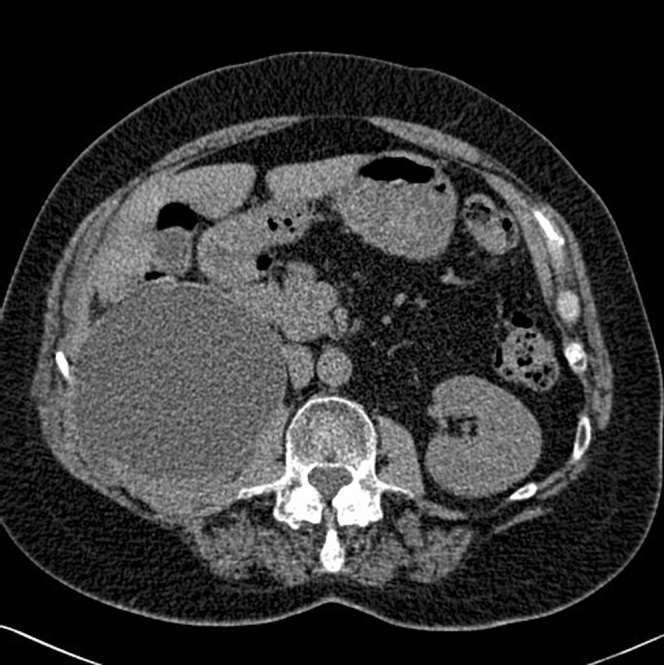
CT scan showing a right-sided urinoma.
After multidisciplinary discussion, percutaneous drainage of the perinephric collection was performed, which resulted in continuous daily urine drainage of 20–100 ml that persisted for the next month, despite the added intervention of a right nephrostomy 2 weeks after drain insertion (Figure 2). The nephrostomy was deliberately placed through the point of leakage. A right retrograde pyelogram was performed and confirmed a lower pole urinary fistula and a PUJ obstruction. A right JJ ureteric stent was sited; however, urine drainage continued from the lower pole leak.
Figure 2.
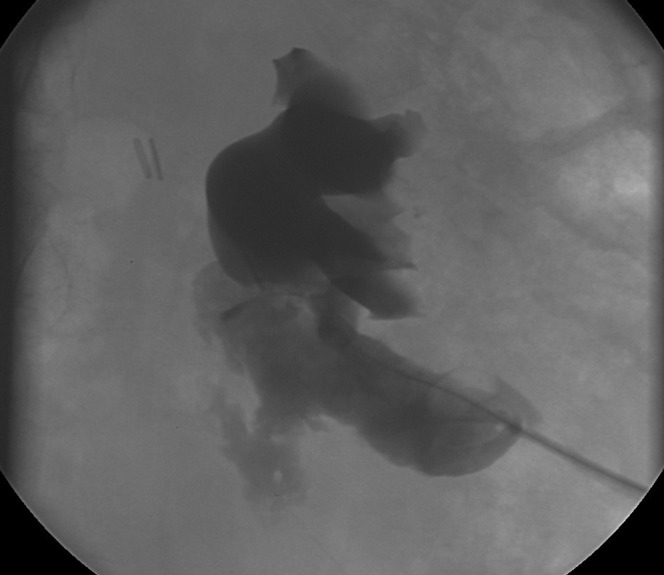
Nephrostogram demonstrating urinary leak.
As the urinary fistula had not responded to conventional management and nephrostomy was not a tolerable long-term option for the patient, the following options were considered:
Gluing of the urinary leak site.
Open repair of the kidney defect.
Right nephrectomy.
An elective decision was made to glue the defect via the right nephrostomy tube. Under local anaesthetic and fluoroscopic guidance, Histoacryl® glue (B Braun, Melsungen, Germany) was injected using a catheter guidewire technique. 6 ml of a 50:50 Histoacryl®:lipiodol mixture was used. This was injected on withdrawal of a catheter along the leakage tract at the lower pole defect (Figures 3 and 4). An 8 Fr drain was left in the space outside the kidney in case further perinephric collection ensued; the right JJ stent remained in situ. Urinary drainage ceased and the drain was removed 5 days later. An ultrasound scan performed 2 weeks after the gluing process demonstrated a small perinephric collection. The JJ stent was removed 4 weeks later. Follow-up renal ultrasound performed 6 months later revealed no collection around the kidney and, clinically, the patient's right loin pain had resolved. CT scans performed at 8 months and 18 months after gluing demonstrated no evidence of a residual collection or renal tract obstruction. High-attenuation artefact was noted in the region of the lower pole right kidney, consistent with lipiodol superglue (Figure 5). The patient remains well with normal renal function.
Figure 3.
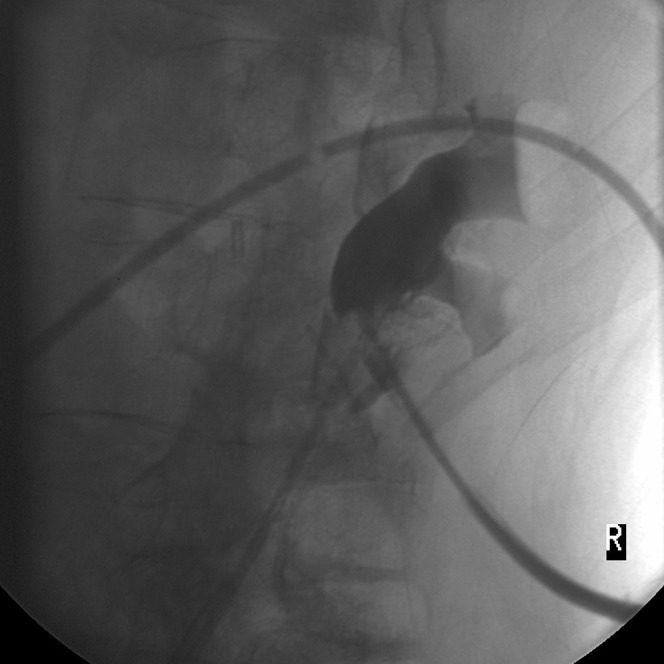
Fluoroscopic-guided gluing of the nephrostomy tract.
Figure 4.
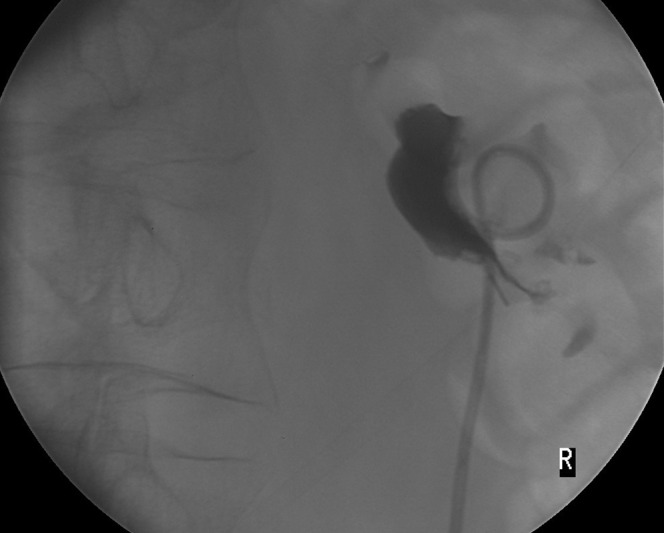
Plain film image immediately after gluing.
Figure 5.
CT image 6 months after gluing, showing no collection and glue artefact.
Discussion
Repair of the collecting system after surgery is one of the major challenges facing the surgeon during partial nephrectomy. A urinary fistula is an acknowledged complication of nephron-sparing surgery [1–3]. Percutaneous drainage and endoscopic ureteric stent placement are accepted management strategies for persistent urinary leak, with reported median times for fistula closure of up to 46 days [1, 2]. Although Meeks et al [4] recently described percutaneous fulguration of a leaking calyx after partial nephrectomy using a flexible ureteroscope when conservative measures had failed, we considered radiological intervention in this case to be the least traumatic approach. To our knowledge, we report the first case of a urinary fistula after open partial nephrectomy being managed successfully with Histoacryl® glue ablation of the renal leak.
Fibrin glues and their sealant properties are not a new concept within urology. Animal model work has examined the ability of fibrin glues to withstand collecting system burst pressures significantly above physiological levels [5]. Glue use as a primary sealant in surgery at various levels of the urinary tract has been reported in the literature (Table 1). We are aware, however, of only one other case report documenting glue use in the closure of a urinary tract fistula, in which Seo et al [11] used fibrin glue to stop urine leakage after laparoscopic partial nephrectomy.
Table 1. Glue use in urological surgery.
Histoacryl® glue use in the urinary tract, as far as we are aware, has not been reported; although its application in wound closure and obliteration of bleeding gastric varices is well documented [12, 13], its value in fistula closure is less well known (Table 2). Potential concerns relating to glue use in vivo include the possibility of a foreign body response, tissue damage from the exothermic reaction prior to setting and, specifically when used in the kidney, the induction of lithiasis; however, there is no evidence to support this. Glue spillage into the collecting system, causing iatrogenic upper urinary tract obstruction, is a potentially severe complication of the technique; therefore, the operator must be familiar and comfortable with glue use.
Table 2. Superglue use in fistulae.
In conclusion, we have demonstrated that, in cases where a urinary fistula persists after partial nephrectomy, Histocryl® glue sealant of the leak is a safe, minimally invasive, last line of intervention if conventional management, in the form of a JJ stent and nephrostomy, has failed or has prolonged morbidity. To facilitate glue use, the selection of kidney access route for nephrostomy must be carefully considered.
References
- 1.Polascik TJ, Pound CR, Maxwell MV, Partin AW, Marshall FF. Partial nephrectomy: technique, complications and pathological findings. J Urol 1995;154:1312–8 [DOI] [PubMed] [Google Scholar]
- 2.Stephenson AJ, Hakimi AA, Snyder ME, Russo P. Complications of radical and partial nephrectomy in a large contemporary cohort. J Urol 2004;171:130–4 [DOI] [PubMed] [Google Scholar]
- 3.Pasticier G, Timsit MO, Badet L, De LaTorreAbril L, Halila M, Fassi-Fehri H, et al. Nephron-sparing surgery for renal cell carcinoma: detailed analysis of complications over a 15-year period. Eur Urol 2006;49:485–90 [DOI] [PubMed] [Google Scholar]
- 4.Meeks JJ, Smith ND, Lesani OA, Nadler RB. Percutaneous endoscopic management of persistent urine leak after partial nephrectomy. J Endourol 2008;22:485–8 [DOI] [PubMed] [Google Scholar]
- 5.Kouba E, Tornehl C, Lavelle J, Wallen E, Pruthi RS. Partial nephrectomy with fibrin glue repair: measurement of vascular and pelvicalyceal hydrodynamic bond integrity in a live and abbatoir porcine model. J Urol 2004;172:326–30 [DOI] [PubMed] [Google Scholar]
- 6.Levinson AK, Swanson DA, Johnson DE, Greskovich FJ, 3rd, Stephenson RA, Lichtiger B. Fibrin glue for partial nephrectomy. Urology 1991;38:314–6 [DOI] [PubMed] [Google Scholar]
- 7.Pruthi RS, Chun J, Richman M. The use of a fibrin sealant during laparoscopic partial nephrectomy. BJU 2004;93:813–7 [DOI] [PubMed] [Google Scholar]
- 8.Eden CG, Sultana SR, Murray KHA, Carruthers RK. Extraperitoneal laparoscopic dismembered fibrin-glued pyeloplasty: medium-term results. Br J Urol 1997;80:382–9 [DOI] [PubMed] [Google Scholar]
- 9.Kram HB, Ocampo HP, Yamaguchi MP, Nathan RC, Shoemaker WC. Fibrin glue in renal and ureteral trauma. Urology 1989;33:215–8 [DOI] [PubMed] [Google Scholar]
- 10.Pfab R, Ascherl R, Blumel G, Hartung R. Local haemostasis of nephrostomy tract with fibrin adhesive sealing in percutaneous nephrolithotomy. Eur Urol 1987;13:118–21 [DOI] [PubMed] [Google Scholar]
- 11.Seo IY, Lee YH, Rim JS. Percutaneous fibrin glue injection for urine leakage in laparoscopic partial nephrectomy. J Endourol 2008;22:959–62 [DOI] [PubMed] [Google Scholar]
- 12.Amiel GE, Sukhotnik I, Kawar B, Siplovich L. Use of N-butyl-2-cyanoacrylate in elective surgical incisions-longterm outcomes 1. J Am Coll Surg 1999;189:21–5 [DOI] [PubMed] [Google Scholar]
- 13.Huang YH, Yeh HZ, Chen GH, Chang CS, Wu CY, Poon SK, et al. Endoscopic treatment of bleeding gastric varices by N-butyl-2-cyanoacrylate (Histoacryl) injection: long term safety and efficacy. Gastrointest Endosc 2000;52:160–7 [DOI] [PubMed] [Google Scholar]
- 14.Papini RP, Niranjan NS. Superglue sealant for persistent leakage of cerebrospinal fluid. Plast Reconstr Surg 1993;91:371–2 [DOI] [PubMed] [Google Scholar]
- 15.Goh PM, Kum CK, Toh EH. Endoscopic patch closure of malignant eosophagotracheal fistula using Histoacryl glue. Surg Endosc 1994;8:1434–5 [DOI] [PubMed] [Google Scholar]
- 16.Santos F, Campos J, Freire J, Andrade A, Tavora I, Castelo HB. Enterocutaneous fistulas: an unusual solution. Hepatogastroenterology 1997;44:1085–9 [PubMed] [Google Scholar]
- 17.Cekirge S, Oquzkurt L, Saatci I, Boyvat F, Balkanci F. Embolization of a high-output post nephrectomy aortocaval fistula with Gianturco coils and cyanoacrylate. Cardiovasc Intervent Radiol 1996;19:56–8 [DOI] [PubMed] [Google Scholar]
- 18.Seewald S, Brand B, Groth S, Omar S, Mendoza G, Seitz U, et al. Endoscopic sealing of pancreatic fistula by using N-butyl-2-cyanoacrylate. Gastrointest Endosc 2004;59:463–70 [DOI] [PubMed] [Google Scholar]