

Abstract
We present a case of synchronous bilateral inoperable lung cancer which required treatment with external beam radiotherapy to a radical dose. Intensity-modulated radiotherapy (IMRT) was used. More conformal dose distribution within the planning target volume was obtained using IMRT than the conventional technique. Dose–volume constraints defined for the lungs were met. Treatment was subsequently delivered using a seven-field IMRT plan. The patient remains alive and disease-free 48 months after the completion of radiotherapy. IMRT can be considered an effective treatment for synchronous bilateral lung cancer.
Synchronous multiple lung cancer was first described in 1924 when Beyreuther identified two separate primary lung tumours in a patient with pulmonary tuberculosis [1]. Its actual incidence remains unknown. However, the recent widespread use of CT and positron emission tomography (PET) in the staging of lung cancer has led to an increase in its rate of detection. The lesions can be unilateral or bilateral. It can often be difficult to distinguish true synchronous multiple primary lung cancer (MPLC) from solitary lung metastasis. MPLCs are of similar histology in more than 80% of cases [2]. Molecular testing of tumour specimens may potentially aid diagnosis. According to the commonly used criteria set by Martini and Melamed [3], MPLC can still be diagnosed even if the two tumours are of the same histology provided the following criteria are met: they must be situated in different lobes or segments of the lung and arise from carcinoma in situ. There must also be an absence of tumour cells in the common lymphatics and no extrapulmonary metastases at presentation. MPLC has not been recognised as a distinct entity in the latest revision of the tumour, node, metastases (TNM) classification. Thus, patients with synchronous bilateral lung nodules will be classed as having M1a disease [4,5].
A pragmatic approach to the management of patients presenting with synchronous bilateral lung nodules involves searching for distant metastases using CT, PET and if necessary cervical mediastinoscopy. If no further lesions are found, management with curative intent can be considered. Palliative radiotherapy in this situation is associated with a poor overall median survival of only 7 months [6]. Radical treatment can take the form of either surgery or radiotherapy. Surgical management of patients with synchronous bilateral lung nodules involves staged bilateral thoracotomies with an interval of 4–6 weeks between the procedures. Those with synchronous unilateral cancers can be managed with pneumonectomy, bilobectomy, multiple wedge resections or a combination of lobectomy and wedge resection [7].
There are currently no published data on the outcome of patients with synchronous bilateral lung cancer treated with conventionally fractionated external beam radiotherapy to a radical dose. The aim of this report is to describe such a case in which intensity-modulated radiotherapy (IMRT) was used. Dosimetric comparison between IMRT and three-dimensional (3D) conformal radiotherapy (CRT) is also presented.
Case study
A 74-year-old male was admitted to hospital with a community-acquired pneumonia that was slow to recover. Subsequent investigations revealed synchronous bilateral lung lesions in both the left upper lobe and right lower lobe bronchi with tumour diameters of 1.8 cm and 1.1 cm, respectively. Histology from these two lesions showed moderately differentiated squamous cell carcinoma. Molecular analysis of tumour specimens was not available at that time. No other sites of disease were found on mediastinoscopy, CT and PET. Martini and Melamed [3] criteria for synchronous MPLC were met. The patient’s Karnofsky performance score was 90 with pre-treatment forced expiratory volume in 1 s (FEV1) of 2.88 l (94.5% predicted), forced vital capacity (FVC) of 3.68 l (90% predicted) and a FEV1-to-FVC ratio of 78.3. Surgical resection was not possible owing to the close proximity of the lesion to the left upper lobe of the carina. Radical radiotherapy was deemed to be the most appropriate curative option by the multidisciplinary team.
Radiotherapy treatment planning
At the Suffolk Oncology Centre, all computerised treatment planning is performed using the Varian Eclipse treatment planning system (Varian Medical Systems, Palo Alto, CA). Radiotherapy plans are calculated using the Eclipse pencil beam algorithm. Our centre has been running an IMRT programme since June 2001, utilising the Helios inverse planning software with Millenium 120 dynamic multileaf collimators (MLCs) (Varian Medical Systems).
The treatment objective for this patient was to deliver a potentially curative dose of 64 Gy to both planning target volumes (PTVs) in 32 fractions using 6 MV photons treating once daily, 5 days a week over 6.5 weeks. The organs at risk (OARs) were the uninvolved lungs and the spinal cord. The volume of lung irradiated to 20 Gy (V20) was minimised and kept below 32%. Constraints were also set so that the mean lung dose (MLD) remained below 20 Gy, the maximum dose to the spinal cord was less than 45 Gy and the PTVs received a minimum dose of 95%. The V20 and MLD were defined using the volume of the combined lungs including the PTV.
The patient was immobilised in a supine position with his arms raised above his head on a perspex chest board. Multislice axial CT images were obtained from the cricoid cartilage to the superior aspect of the second lumbar vertebra with intravenous contrast and a slice width of 2.5 mm. The gross tumour volumes (GTVs) were delineated. These were grown isotropically with a 1.5 cm margin to form the PTVs, which account for tumour motion and geometric uncertainties. The contrast was set to water-equivalent electron density for planning.
An initial attempt was made using the 3D CRT technique. Separate plans were produced for both the left and right PTVs with each plan normalised to its isocentre, which was placed in the middle of its respective PTV. The left- and right-sided plans were then summed together to create the best conformal solution. Figure 1 demonstrates the beam arrangements. The right-sided PTV was treated with two fields while the larger left-sided PTV was treated with three fields. The resulting PTV coverage was unsatisfactory. This was mainly owing to an area of overlap between the two PTVs measuring 2.5 cm in length in the superior to inferior direction. Only 76% of the combined PTV received at least 95% of the prescription dose. The maximum dose within the PTV was 79 Gy or 123% of the prescribed dose. The minimum dose was 54 Gy or 85% of the prescribed dose. 37.5% of the PTV received more than 107% of the prescription dose.
Figure 1.
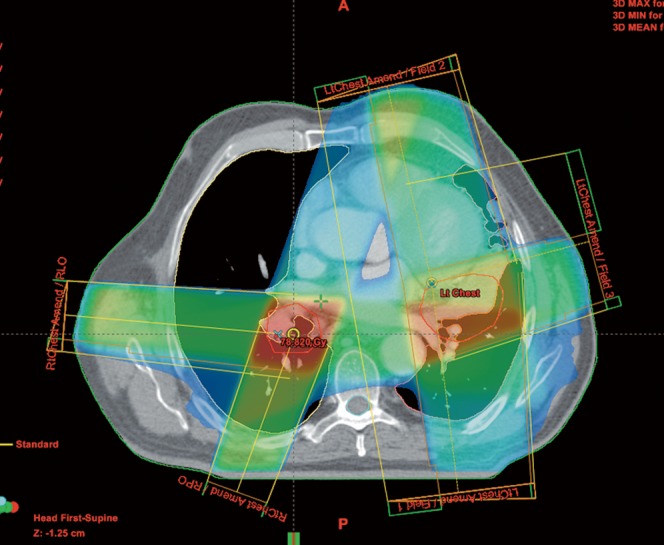
Beam arrangements for the conventional three-dimensional conformal plan.
The IMRT solution was thus explored. It offered the potential to improve PTV coverage, reduce dose inhomogeneity within the PTV and simplify treatment delivery by using a single plan with one isocentre. Seven equally spaced coplanar 6 MV fields were applied (Figure 2). Upper and lower constraints were placed on the PTVs. Upper constraints were also set for the spinal cord while dose–volume histogram (DVH) constraints were used to keep lung doses within tolerance. The plan was optimised using inverse planning. No plan normalisation was employed. The prescription dose was the median dose to the PTV.
Figure 2.
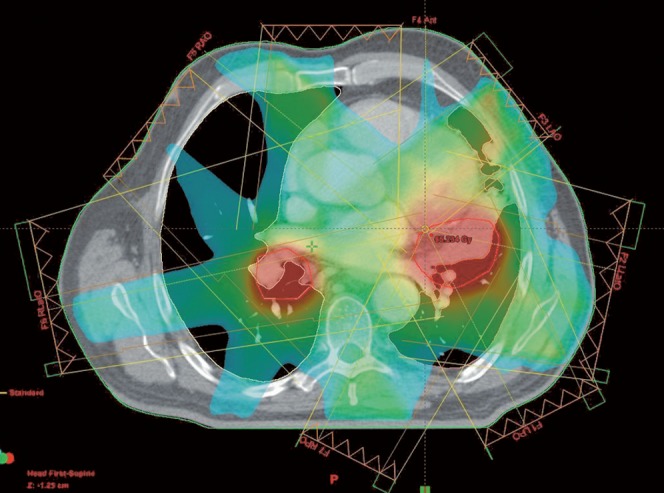
Beam arrangements for the seven-field intensity-modulated radiotherapy plan.
Both the IMRT and 3D CRT plans were then evaluated slice-by-slice for the 3D dose distribution. DVH data for the OARs and PTV were also assessed. Table 1 shows a summary of the dose parameters for both plans.
Table 1. Dose parameters for both 3D CRT and IMRT plans.
| 3D CRT | IMRT | |
| PTV (maximum) | 79.3 Gy (123.9%) | 65.8 Gy (102.8%) |
| PTV (minimum) | 54.3 Gy (84.8%) | 56.9 Gy (88.9%) |
| Percentage PTV covered by the | 76.0% | 99.6% |
| 95% isodose | ||
| Mean dose to PTV | 66.1 Gy | 63.7 Gy |
| Spinal cord (maximum) | 5.6 Gy | 37.5 Gy |
| Combined lungs | ||
| V5 | 45.0% | 60.0% |
| V20 | 24.1% | 32.4% |
| V30 | 19.9% | 13.2% |
| Mean dose | 14.1 Gy | 14.5 Gy |
3D CRT, three-dimensional conformal radiotherapy; IMRT, intensity-modulated radiotherapy; PTV, planning target volume.
A visual inspection of the IMRT plan revealed better PTV coverage and improved dose homogeneity compared with the summed conformal plan. Figure 3 shows a comparison between the DVHs of the two plans. Using the conformal technique, there was a 39.1% variation in dose within the PTV.
Figure 3.

Dose–volume histograms for both the conventional three-dimensional conformal (triangles) and intensity-modulated radiotherapy (squares) plans showing planning target volume (red), combined lungs (purple) and spinal cord (blue).
In terms of the OARs, both the V20 and MLD were used to correlate the risk of radiation pneumonitis following radiotherapy. The MLDs were similar for both plans. However, the V20 was higher in the IMRT plan. It was 32.4% for the IMRT plan and 24.1% for the 3D CRT plan. The corresponding values for V5 were 60% for IMRT and 45% for 3D CRT. In the conformal plan, the beam directions were chosen such that a section of the anterior right lung was completely spared. This was not possible with the seven equally spaced fields of IMRT.
The IMRT plan was delivered using a Varian 2100EX linear accelerator system (Varian Medical System). The patient received the prescribed dose of 64 Gy in 32 fractions over 6.5 weeks to both lesions simultaneously. The treatment was well tolerated with no reported toxicities. Treatment was completed on time. There was no treatment-related pneumonitis (TRP). The patient remained alive 48 months after the completion of radiotherapy with no evidence of disease recurrence on bronchoscopy, CT and PET. Results of his lung function tests post therapy remained stable with an FEV1 of 2.60 l (85.4% predicted), FVC of 3.31 l (81.7% predicted) and a FEV1-to-FVC ratio of 78.5.
Discussion
The aim of radical radiotherapy is to deliver a radiation dose to the PTV that will result in tumour cell death while minimising the risk of damage to the surrounding normal tissues. In this report, we describe a case of synchronous bilateral inoperable lung cancer which was successfully treated with external beam radiotherapy. IMRT was used because the 3D CRT plan provided suboptimal PTV coverage. Both the V20 and MLD remained within the constraints of the lung. The patient did not experience any TRP. IMRT should be considered in situations such as this where the 3D CRT solution is unsatisfactory.
There is very little published data on the use of radiotherapy in patients with synchronous bilateral lung cancer. Palliative radiotherapy is an option, but is associated with poor median overall survival [6]. The Indiana University has reported their experience using stereotactic body radiotherapy for the curative treatment of patients with bilateral MPLC. Eight patients had synchronous tumours. Between 7 and 10 non-coplanar beams were used. Treatment was delivered in 3–4 fractions with radiation doses varying between 48 Gy and 66 Gy. No grade 3 or 4 toxicity was observed. Two of these patients developed disease progression following radiotherapy, one of whom had a local recurrence within the radiation field [8].
In the presence of tumour–lung interface, dose calculation using the pencil beam algorithm will not be as accurate as the convolution superposition or the analytical anisotropic algorithms. Differences in tissue density between the tumour and the surrounding lung will give rise to areas of electronic disequilibrium. This in turn affects the accuracy of dose computation using pencil beam, with overestimation of the dose within the PTV due to electron transport out of the target into the surrounding low-density lung tissue and underestimation of the width of the beam penumbra and hence the V20 and MLD [9,10]. These effects will be augmented with the smaller fields used in IMRT. Our centre has since switched over to the convolution superposition algorithm for dose calculation in lung radiotherapy.
TRP remains a dose-limiting toxicity in thoracic radiotherapy. Its clinical diagnosis, assessment and scoring can be difficult [11]. There had been numerous studies attempting to identify clinical and dosimetric parameters associated with TRP following chest radiotherapy. These studies had produced inconsistent results because different TRP definitions, study populations, radiotherapy techniques and treatment regimens were used. It is not surprising that no parameters had been identified that consistently predict TRP risk across studies [12]. The recently published QUANTEC (quantitative analysis of normal tissue effects in the clinic) review acknowledged the difficulty in recommending dose–volume constraints for the lungs and suggested placing limits on the MLD and V20 to minimise TRP risk [13].
One of the concerns surrounding the use of IMRT in the treatment of non-small cell lung cancer (NSCLC) is the large volume of uninvolved lung exposed to low doses of radiation. Recent evidence from the laboratory using a rat model suggested a larger impact on pulmonary function from irradiating large lung volumes with a low dose than from irradiating small volumes of lung with a large dose [14]. In a retrospective analysis using data from patients with NSCLC treated with concurrent chemotherapy and 3D CRT, V5 was found on multivariate analysis to be the most significant factor associated with TRP [15]. However, reports from the use of IMRT in NSCLC seem to suggest lower rates of TRP compared with 3D CRT. Yom et al [16] noted an 8% rate of grade 3 and higher TRP at 12 months with IMRT compared with 32% with 3D CRT among patients receiving concurrent chemoradiation for advanced NSCLC. This was despite a higher V5 and a larger median gross tumour volume within the IMRT group, which included patients whose tumours could not be optimally treated with 3D CRT. This suggests that V5 may not be the only determinant factor for TRP in patients with NSCLC receiving IMRT. In a retrospective review of 55 patients with inoperable NSCLC treated with IMRT at the Memorial Sloan-Kettering Cancer Centre, an 11% rate of grade 3 acute pulmonary toxicity was reported, lower than that observed with studies involving 3D CRT [17]. Additional work is certainly needed to better define the relationship between V5 and TRP in lung IMRT.
Conclusions
IMRT can be considered an effective treatment for patients with synchronous bilateral lung cancer.
References
- 1.Beyreuther H. Multiplicitat von carcinomen bei ein fall von sog: ‘schneeberger’ lungenkrebs mit tuberculose. Virchows Arch Pathol Anat 1924;250:230–6 [Google Scholar]
- 2.Trousse D, Barlesi F, Loundou A, Tasei AM, Doddoli C, Giudicell R, et al. Synchronous multiple primary lung cancer: An increasing clinical occurrence requiring multidisciplinary management. J Thorac Cardiovasc Surg 2007;133:1193–200 [DOI] [PubMed] [Google Scholar]
- 3.Martini N, Melamed MR. Multiple primary lung cancers. J Thorac Cardiovasc Surg 1975;70:606–12 [PubMed] [Google Scholar]
- 4.Postmus P, Brambilla E, Chansky K, Crowley J, Goldstraw P, Patz EF, Jr, et al. The IASLC lung cancer staging project: proposals for revision of the M descriptors in the forthcoming (seventh) edition of the TNM classification of lung cancer. J Thorac Oncol 2007;2:686–93 [DOI] [PubMed] [Google Scholar]
- 5.Goldstraw P, Crowley J, Chansky K, Giroux DJ, Groome PA, Rami-Porta R, et al. The IASLC lung cancer staging project: proposals for the revision of the TNM stage groupings in the forthcoming (seventh) edition of the TNM classification of malignant tumours. J Thorac Oncol 2007;2:706–14 [DOI] [PubMed] [Google Scholar]
- 6.Ampil FL, Chin HW. Palliative radiotherapy for synchronous bilateral lung cancers. Am J Clin Oncol 2001;24:385–7 [DOI] [PubMed] [Google Scholar]
- 7.Adebonojo SA, Moritz DM, Danby CA. The results of modern surgical therapy for multiple primary lung cancers. Chest 1997;112:693–701 [DOI] [PubMed] [Google Scholar]
- 8.Sinha B, McGarry RC. Stereotactic body radiotherapy for bilateral primary lung cancers: the Indiana University experience. Int J Radiat Oncol Biol Phys 2006;66:1120–4 [DOI] [PubMed] [Google Scholar]
- 9.Vanderstraeten B, Reynaert N, Paelinck L, Madani I, De Wagter C, De Gersem W, et al. Accuracy of patient dose calculation for lung IMRT: a comparison of Monte Carlo, convolution/superposition, and pencil beam computations. Med Phys 2006;33:3149–58 [DOI] [PubMed] [Google Scholar]
- 10.Davidson SE, Popple RA, Ibbott GS, Followill DS. Technical note: Heterogeneity dose calculation accuracy in IMRT: study of five commercial treatment planning systems using an anthropomorphic thorax phantom. Med Phys 2008;35:5434–9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Kocak Z, Evans ES, Zhou S, Miller KL, Floz RJ, Shafman TD, et al. Challenges in defining radiation pneumonitis in patients with lung cancer. Int J Radiat Oncol Biol Phys 2005;62:635–8 [DOI] [PubMed] [Google Scholar]
- 12.Bradley JD, Hope A, El Naqa I, Apte A, Lindsey PE, Bosch W, et al. A nomogram to predict radiation pneumonitis, derived from a combined analysis of RTOG 9311 and institutional data. Int J Radiat Oncol Biol Phys 2007;69:985–92 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Marks LB, Bentzen SM, Deasy JO, Kong FM, Bradley JD, Vogelius IS, et al. Radiation dose-volume effects in the lung. Int J Radiat Oncol Biol Phys 2010;76:S70–6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Semenenko VA, Molthen RC, Li C, Morrow NV, Li R, Ghosh SN, et al. Irradiation of varying volumes of rat lung to same mean lung dose: a little to a lot or a lot to a little? Int J Radiat Oncol Biol Phys 2008;71:838–47 [DOI] [PubMed] [Google Scholar]
- 15.Wang S, Liao Z, Wei X, Liu HH, Tucker SL, Hu C, et al. Analysis of clinical and dosimetric factors associated with treatment-related pneumonitis (TRP) in patients with non-small-cell lung cancer (NSCLC) treated with concurrent chemotherapy and three-dimensional conformal radiotherapy (3D-CRT). Int J Radiat Oncol Biol Phys 2006;66:1399–407 [DOI] [PubMed] [Google Scholar]
- 16.Yom SS, Liao Z, Liu HH, Tucker SL, Hu CS, Wei X, et al. Initial evaluation of treatment-related pneumonitis in advanced-stage non-small-cell lung cancer patients treated with concurrent chemotherapy and intensity-modulated radiotherapy. Int J Radiat Oncol Biol Phys 2007;68:94–102 [DOI] [PubMed] [Google Scholar]
- 17.Sura S, Gupta V, Yorke E, Jackson A, Amols H, Rosenzweig KE. Intensity-modulated radiation therapy (IMRT) for inoperable non-small cell lung cancer: the Memorial Sloan-Kettering Cancer Center (MSKCC) experience. Radiother Oncol 2008;87:17–23 [DOI] [PMC free article] [PubMed] [Google Scholar]