

The Oxford English Dictionary (1) defines a phenotype as the “sum total of observable characteristics of an individual, regarded as the consequences of the interaction of the individual’s genotype and environment; a variety of an organism distinguished by observable characteristics rather than underlying genetic features.” Wikipedia (2) expands this definition to” any observable characteristic or trait of an organism such as its morphology, development, biochemical, or physiologic properties or behavior.” One key element of these definitions is that a phenotype is defined by a characteristic that is observable by the naked eye, by images or by blood tests. A genotype is often the source of phenotypic variation, but a genotype is only relevant to phenotypes when it creates an observable difference between two organisms with the same disease; thus a genotype expression can create phenotypic variation when the effect of the genotype is observable.
Examples of phenotypes in medicine include treatment defining phenotypes such as when a woman with breast cancer has a tumor that is estrogen receptor positive and therefore is treated with tamoxifen. If her tumor were estrogen-receptor negative, she would not be so treated. Another example constitutes families who inherit the BRCA gene which alters the prevention approach to their breast cancer or ovarian cancer and a third is when a phenotype alters the conceptualization of disease biology such as when Marshall suggested that gastric ulcers might actually be caused by bacteria, a prophetic suggestion confirmed when the H. pylori bacterium was discovered and characterized in ulcers.
The overall goal of this paper is to explore the existence of distinct phenotypes in osteoarthritis. To accomplish this goal, I will posit criteria to use to define phenotypes and then will suggest which phenotypes exist and which do not.
Ultimately, there are hundreds of phenotypes that could be defined in osteoarthritis. To be meaningful for clinical practice and for epidemiologic studies, phenotype distinctions should be confined to those that affect treatment or prevention decisions and to those which clearly have a fundamental effect on the way we view disease biology and/or disease etiology. Since our knowledge of disease and our ability to observe or image aspects of disease are continually changing, it is likely that new insights will, in turn, support the existence of new or evolving phenotypes. Therefore, any elaboration of disease phenotypes is necessarily limited to current knowledge and technology.
The most common factors defining phenotypes are risk or etiologic factors in addition to genetic variation. For example, hip osteoarthritis phenotypes are defined based on developmental hip abnormalities such as congenital dysplasia. Hips with developmental abnormalities often need early surgeries and are therefore different phenotypes than those without such early changes. Among the most common factors differentiating disease phenotypes is extent of disease. In cancer, TNM classifications which describe the extent and severity of a cancer often define different treatment choices. For example, breast cancer that is small and limited in scopewithin the breast might be treated with a lumpectomy, whereas metastatic disease would require chemotherapy.
Since osteoarthritis is widely regarded as a final common pathway of joint destruction for multiple different pathophysiologic etiologies including trauma, developmental etiologies, primary cartilaginous disorders, and even crystal induced arthritis, differentiating these etiologies might provide different phenotypes of osteoarthritis. Identifying different phenotypes in osteoarthritis may be highly relevant to treatment and prevention development in this disease. Therefore, isolating phenotypes in osteoarthritis may be critical to development of effective treatment and disease prevention. If treatment works only in one sub-type, for example, a treatment targeted to bone marrow lesions, we will miss the therapeutic effect of that treatment if it is tested in everyone with osteoarthritis, because many do not have bone marrow lesions. If, on the other hand, treatment does not work in a subset of disease with a particular common feature, we may miss the effect of treatment on the less common subset that does not have this feature. An example of this might be if malalignment of the knee creates too much focal stress for a chondroprotective agent to work. The same considerations would be relevant for disease prevention as for disease treatment.
Epidemiologists approach phenotypic distinctions by invoking sufficient cause models (see figure). Each of these pie charts constitutes a hypothetical cause of osteoarthritis. For example, on the left, we could hypothesize that 40% of knee osteoarthritis was due to a combination of risk factors including obesity, getting older, and being a women. Since not all overweight, older women develop knee osteoarthritis, an unknown set of causes is also invoked. What is relevant about this particular sufficient cause pie is that if any of the causes is removed (e.g., if obesity were eliminated), a sufficient cause of disease would no longer occur and knee osteoarthritis prevalence would decrease. Thus, if obesity were eliminated, up to 40% of knee osteoarthritis would no longer occur. In the middle figure is another pie of disease caused by knee injury along with age and combined with the usual unknown set of causes because not all people with injury who are older get osteoarthritis. On the right, we postulate that roughly 15% of knee OA is due to genetic causes and that genes could translate into a phenotype if the effects of the gene created an observable characteristic, a phenotype. The hypothetical pie charts depicted do not account for 100% of knee OA, because there must be other causal pathways that determine other phenotypes in disease.
The remainder of this paper will address three specific issues. First, what is the evidence supporting the validity of widely used phenotypes in osteoarthritis? Second, what are other likely phenotypes, not currently widely hypothesized as being phenotypes in OA? And lastly, how will we determine and confirm phenotype distinctions that might be of importance in osteoarthritis?
The Validity of Widely Used Phenotypes
Generalized vs. Joint Specific Osteoarthritis
The first widely used phenotype in osteoarthritis consists of differentiating between generalized arthritis and joint specific disease. Recent work from the consortia carrying out meta-analyses of genome wide association studies in osteoarthritis has suggested that there is at least one polymorphism that is associated with a heightened risk of generalized disease (3) the GDF 5 allele. According to results from both meta-analyses of Asian populations (4) and European populations (3), an allele in the GDF 5 intron which decreases the quantity but does not affect the structure of GDF 5, confers an increased risk of osteoarthritis, perhaps because it depletes cartilage of an anabolic stimulus or because of effects on skeletal development. Heightened risks of hip, knee and, to a lesser extent, hand osteoarthritis, have been seen among populations where this GDF 5 allele is carried. The GDF 5 results suggest that there is a generalized entity, perhaps conferred by genetic transmittal that increases the risk of osteoarthritis in multiple joints. Having said that, most studies examining the heritability of osteoarthritis in populations (5;6) have suggested that most heritability is conferred by the inheritance of genes that confer a heightened risk of joint specific and not generalized osteoarthritis. Those families with hip osteoarthritis transmit an increased risk of hip osteoarthritis but not of osteoarthritis in other joints. The same is true for osteoarthritis in the hands to the point where even inheritance of thumb based osteoarthritis is separate from inheritance of osteoarthritis in the DIP and PIP hand joints (5). Recently, MacGregor (6) and colleagues found no association at all between the genetic inheritance of osteoarthritis in the DIP joints and osteoarthritis in the hips and almost no association between hand and knee osteoarthritis. This suggests that much of the genetic basis for osteoarthritis occurs on a joint specific basis and may relate to joint shape or developmental abnormalities.
The genetics of osteoarthritis provides evidence that both generalized and joint specific phenotypes of osteoarthritis exist, but that joint specific disease, even driven by genetic considerations, may be the more common.
Secondary versus Primary OA
Osteoarthritis due to identifiable causes, which by themselves can cause disease without the contribution of other likely risk factors, has been characterized as a separate phenotype from primary osteoarthritis and has been conceptualized as an uncommon cause of osteoarthritis. Causes of secondary OA include major joint injury, metabolic disorders, and possibly crystal disease. Osteoarthritis, without an identifiable cause, is labeled as primary disease.
The proportion of osteoarthritis that is secondary is likely to be substantially higher than previously believed. For example, in the Framingham Study, a community based sample of persons selected without regard to knee osteoarthritis or knee pain, 40-60% of older men had meniscal tears on MRI, most of them incidental and unrelated to pain. Older women also had a high rate of meniscal tears, although less than men (7). Englund et al (8) reported that these tears, often asymptomatic, led to a marked increase risk in the development of osteoarthritis over the subsequent thirty months. (The tears could represent the first evidence of the OA process) The high rate of osteoarthritis among those with incidental tears and the high prevalence of incidental tears suggests that up to 50% of osteoarthritis in the community may be due to meniscal tear and that does not count minor and/or unrecognized injuries that may predispose to the development of osteoarthritis. The high prevalence of metabolic factors, such as the existence of crystals within the joint, which may also predispose to disease, suggests that secondary OA may be more the rule than the exception, at least for knee osteoarthritis. Ultimately, as we better understand the pathogenesis of osteoarthritis in subsets of persons with disease, primary disease may become a meaningless concept. Thus, this phenotypic distinction may not serve well in the pursuit of a better understanding of the pathogenesis of disease.
Incident versus Progressive Osteoarthritis
In epidemiologic circles, the distinction is often made between the new onset of the disease (incident disease) and the presence of disease which can progress after it has occurred (progressive disease). The distinction between these two stages of disease depends on whether disease can be clearly characterized as present or absent (such medical conditions as hip fracture and myocardial infarction are good examples of easily defined disease incidence). In osteoarthritis, on the other hand, many persons in the community have evidence of disease such as definite osteophytes in one joint, and it is unclear who has disease and who does not nor when exactly disease begins. Is disease present when there is a small osteophyte without symptoms in one joint only, for example? Does it become manifest when the osteophyte becomes larger and definite? Defining incidence and progression is challenging; and the distinction between these phenotypes is less clear-cut than is optimal. Using thresholds to define the existence of disease is necessary; in order to study disease, but recognition that these thresholds that demarcate present disease from absent disease do not necessarily represent distinct phenotypes is important.
Suggested Phenotypes
Many persons with osteoarthritis in the community do not have any pain (9) and would not necessarily want to be treated for a structural abnormality that is causing them no problems. Thus, it might be useful to distinguish between those with painful versus non- painful osteoarthritis.
Among those with pain, there are a set of unique manifestations that probably represent activation of the central nervous system to create a chronic painful disorder with elements of dysfunctional pain. These patients have receptor field enlargement (the feeling of pain beyond their joints) and often on testing have evidence of generalized hypersensitivity to pain (10). Such persons probably should be recognized as having a separate phenotype as they may need and respond to treatment that is different from that targeted toward specific joint pain. Thus, it is useful to separate out persons with osteoarthritis who have a painful disorder that includes dysfunctional elements of pain and those with osteoarthritis perhaps at a milder stage who have functional pain only and do not have evidence of central nervous system activation.
One suggested phenotype includes knees with malalignment severe enough to drive the disease process. We have found repeated evidence (11) (12) (13) that knees that are sufficiently malaligned progress to worse disease without the presence of other known risk factors. For example, we have reported that obesity is not a risk factor for progression of disease in knees that are malaligned, whereas it is a risk factor among knees with osteoarthritis that are in neutral alignment (11). Malalignment confers high focal stress, a level of stress that probably transcends the ability of cartilage or bone within the joint to withstand it. Evidence for this includes the strong association of malalignment with the presence of bone marrow lesions (14) which on histology are traumatic lesions to bone including micro-cracks suggesting that malalignment actually damages bone (15). If this is so, it is likely that the overlying cartilage also is damaged solely by malalignment. The implications for the presence of this malaligned phenotype is that treatments targeted towards cartilage protection are not likely to work in knees that are malaligned. If conventional risk factors such as obesity do not confer an increased risk in such malaligned knees, then it seems likely that drugs to protect cartilage will be insufficiently effective to prevent progression in such knees (sufficient cause figure 2). As shown in the figure, malalignment itself is sufficient to cause progression of disease along with the usual unknown set of risk factors; obesity and other known risk factors are not included in this pie because they are not necessary to cause disease. This malalignment based sufficient cause accounts for up to 60% of knee osteoarthritis progression with the minority being accounted for by known risk factors such as obesity and age.
Figure 2.
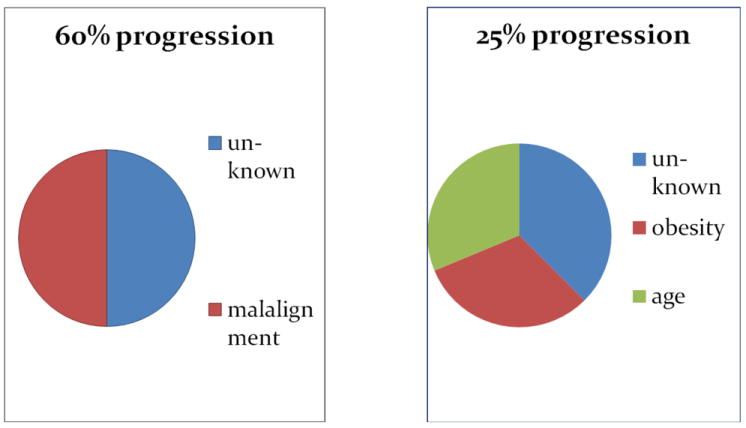
Percent of Progressive Knee OA Among Knee OA cases
Identifying and Validating Phenotypic Distinctions
We next turn to approaches to confirm these phenotypes and identify yet other new phenotypes in osteoarthritis. Epidemiologic and statistical approaches to identify sub-types of disease include factor or cluster analyses, statistical approaches which take a large population and break them into clustered sub-groups within that population. While ideal as a statistical tool, cluster and factor analyses have not, by themselves, characterized a disease phenotype, but have been used to corroborate ones that have been clinically identified. Another theoretical approach would be to take a genome wide association study that identified specific SNPs as related to disease that then, in turn, identified genes whose functions were known and then tested whether those genes conferred a particular observable, distinct phenotype of disease different from disease not caused by these genes.
Another approach to defining subtypes of disease would include the epidemiologic approaches used to characterize the malalignment phenotype in which it was discovered that known risk factors such as obesity did not operate when particular other risk factors were present. If this can be confirmed in multiple studies, then that would identify a confirmed subtype. Lastly and importantly, biological understandings of disease are the most likely source for identifying new phenotypes that can be tested then in clinical populations.
Once subtypes have been hypothesized or identified, it is challenging to confirm them. Confirmation in independent studies is absolutely critical. Ioannidis (16) working in the genetics field, has noted that over 90% of initial reports of genetic associations are not confirmed in subsequent studies. This is also likely to be the case for proposed subtypes in osteoarthritis. The initial finding of a subtype is often exciting, but confirming that subtype in large, more definitive studies is often extremely challenging. The phenotype, as noted earlier, must define response to treatment or prevention strategy or must provide evidence that it is important for understanding biological differences among types of disease. Large studies are best for both identifying subtypes and for confirming these subtypes.
Figure 1.
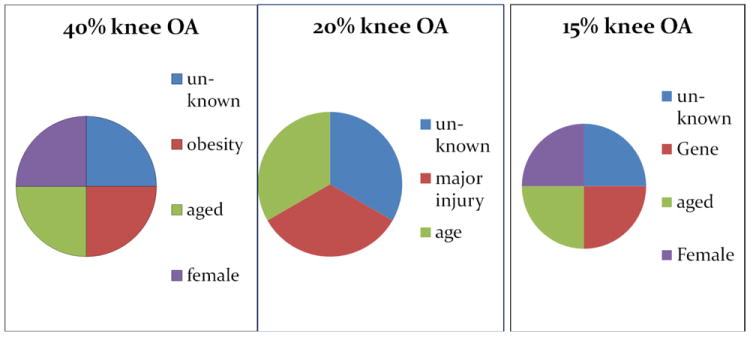
Percent of Knee OA Due to Hypothesized Causes of Knee OA
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Reference List
- 1.Phenotype. Oxford English Dictionary; 2008. Dec, [2010 Jan 13]. Available from: URL: http://dictionary.oed.com/cgi/entry/50177331?query_type=word&queryword=phenotype&first=1&max_to_show=10&sort_type=alpha&result_place=1&search_id=S9yI-jMFnwg-5689&hilite=50177331. [Google Scholar]
- 2.Phenotype. 2009 Oct 20; http://en.wikipedia.org/wiki/Phenotype.
- 3.Evangelou E, Chapman K, Meulenbelt I, Karassa F, Loughlin J, Carr A, et al. Large-scale analysis of association between GDF5 and FRZB variants and osteoarthritis of the hip, knee, and hand. Arthritis & Rheumatism. 2009;60(6):1710–21. doi: 10.1002/art.24524. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Miyamoto Y, Mabuchi A, Shi D, Kubo T, Takatori Y, Saito S, et al. A functional polymorphism in the 5’ UTR of GDF5 is associated with susceptibility to osteoarthritis. Nat Genet. 2007;39(4) doi: 10.1038/2005. [DOI] [PubMed] [Google Scholar]
- 5.Hunter DJ, Demissie S, Cupples LA, Aliabadi P, Felson DT. A genome scan for joint-specific hand osteoarthritis susceptibility: The Framingham Study. Arthritis Rheum. 2004 Aug;50(8):2489–96. doi: 10.1002/art.20445. [DOI] [PubMed] [Google Scholar]
- 6.MacGregor A, Li Q, Spector TD, Williams FMK. The genetic influence on radiographic osteoarthritis is site specific at the hand, hip and knee. Rheumatology (Oxford) 2009;(48):277–80. doi: 10.1093/rheumatology/ken475. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Englund M, Guermazi A, Gale D, Felson DT. Incidental meniscal findings on knee MRI in middle aged and elderly persons in the United States. N Engl J Med. 2008;359(11):1108–15. doi: 10.1056/NEJMoa0800777. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Englund M, Guermazi A, Roemer F, Felson DT. Meniscal tear in knees without surgery and the development of radiographic osteoarthritis among middle-aged and elderly persons. The MOST Study. Arthritis & Rheumatism. 2009;60(3):831–9. doi: 10.1002/art.24383. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Hannan MT, Felson DT, Pincus T. Analysis of the discordance between radiographic changes and knee pain in osteoarthritis of the knee. J Rheumatol. 2000 Jun;27(6):1513–7. [PubMed] [Google Scholar]
- 10.Kosek E, Ordeberg G. Lack of pressure pain modulation by heterotopic noxious conditioning stimulation in patients with painful osteoarthritis before, but not following, surgical pain relief. Pain. 2000;88(1):69–78. doi: 10.1016/S0304-3959(00)00310-9. [DOI] [PubMed] [Google Scholar]
- 11.Niu J, Zhang YQ, Torner J, Nevitt M, Lewis CE, Aliabadi P, et al. Is obesity a risk factor for progressive radiographic knee osteoarthritis? Arthritis & Rheumatism. 2009;61(3):329–35. doi: 10.1002/art.24337. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Nevitt M, Zhang Y, Javaid M, Felson DT. High systemic bone density, fractures and the risk of incident and progressive radiographic knee OA: the MOST Study. Ann Rheum Dis. 2009 doi: 10.1136/ard.2008.099531. In press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Felson DT, Goggins J, Niu J, Zhang Y, Hunter DJ. The effect of body weight on progression of knee osteoarthritis is dependent on alignment. Arthritis Rheum. 2004 Dec;50(12):3904–9. doi: 10.1002/art.20726. [DOI] [PubMed] [Google Scholar]
- 14.Felson DT, McLaughlin S, Goggins J, Lavalley MP, Gale ME, Totterman S, et al. Bone marrow edema and its relation to progression of knee osteoarthritis. Ann Intern Med. 2003 Sep 2;139(5 Pt 1):330–6. doi: 10.7326/0003-4819-139-5_part_1-200309020-00008. [DOI] [PubMed] [Google Scholar]
- 15.Taljanovic MS, Graham AR, Benjamin JB, Gmitro AF, Krupinski EA, Schwartz SA, et al. Bone marrow edema pattern in advanced hip osteoarthritis: quantitative assessment with magnetic resonance imaging and correlation with clinical examination, radiographic findings, and histopathology. Skeletal Radiol. 2008;37:423–31. doi: 10.1007/s00256-008-0446-3. [DOI] [PubMed] [Google Scholar]
- 16.Ioannidis JPA. Why most published research findings are false. PLoS Med. 2005;2(8):e124. doi: 10.1371/journal.pmed.0020124. [DOI] [PMC free article] [PubMed] [Google Scholar]